Brain Neoplasms: Practice Essentials, Pathophysiology, Etiology (original) (raw)
Brain tumors may originate from neural elements within the brain, or they may represent spread of distant cancers. Primary brain tumors arise from CNS tissue and account for roughly half of all cases of intracranial neoplasms. The remainder of brain neoplasms are caused by metastatic lesions.
In adults, two thirds of primary brain tumors arise from structures above the tentorium (supratentorial), whereas in children, two thirds of brain tumors arise from structures below the tentorium (infratentorial). Gliomas, metastases, meningiomas, pituitary adenomas, and acoustic neuromas account for 95% of all brain tumors. See the image below.
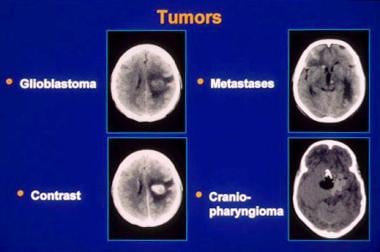
Brain neoplasms. CT images of several tumor types. Slide courtesy of UMASS Continuing Education Office.
Signs and Symptoms
Presenting complaints of patients with an intracranial neoplasm tend to be similar for primary brain tumors and intracranial metastases. The onset of symptoms usually is insidious, but an acute episode may occur with bleeding into the tumor, or when an intraventricular tumor suddenly occludes the third ventricle.
Manifestations may be nonspecific and include the following:
- Headache
- Altered mental status
- Ataxia
- Nausea
- Vomiting
- Weakness
- Gait disturbance
CNS neoplasms also may manifest as follows:
- Focal seizures
- Fixed visual changes
- Speech deficits
- Focal sensory abnormalities
Headache associated with intracranial neoplasms have the following characteristics:
- Often is a late complaint
- Usually not an isolated finding
- The worst symptom in only one half of patients
- Usually nonspecific and resembles tension-type headaches [1, 2]
- In patients with established headache, may manifest as a change in the headache pattern
- New onset of headaches in middle-aged or older patients is worrisome
- The location of the headache reliably indicates the side of the head affected, but it does not indicate the precise site of the tumor
- Headaches are more common with posterior fossa tumors
- Headache is a more frequent symptom of intracranial tumor in pediatric patients
- Nausea and/or vomitting (40%)
Although often described as characteristic of tumor headaches, the following clincial features are not commonly present [1] :
- Pain that is worse in the early morning than at other times
- Exacerbation with Valsalva maneuvers, bending over, or rising from a recumbent position
No physical finding or pattern of findings unmistakably identifies a patient with a CNS neoplasm. Based on their location, intracranial tumors may produce a focal or generalized deficit, but signs may be lacking (especially if the tumor is confined to the frontal lobe) or even falsely localizing. Findings may include the following:
- Papilledema, which is more prevalent with pediatric brain tumors, reflects an increase in intracranial pressure (ICP) of several days or longer
- Diplopia may result from displacement or compression of the sixth cranial nerve at the base of the brain
- Impaired upward gaze, called Parinaud syndrome, may occur with pineal tumors
- Tumors of the occipital lobe specifically may produce homonymous hemianopia or partial visual field deficits
- Anosmia may occur with frontal lobe tumors
- Brainstem and cerebellar tumors induce cranial nerve palsies, ataxia, incoordination, nystagmus, pyramidal signs, and sensory deficits on one or both sides of the body
See Presentation for more detail.
Diagnosis
With clinical suspicion of cancer, obtain routine laboratory studies on admission, including the following:
- Complete blood cell count (CBC)
- Coagulation studies
- Electrolyte levels
- Comprehensive metabolic panel
Obtain neuroimaging studies in patients with symptoms suggestive of an intracranial neoplasm, such as the following:
- Acute mental status changes
- New-onset seizures
- Focal motor or sensory deficits, including gait disturbance
- Suspicious headache
- Signs of elevated ICP (eg, papilledema)
- Generally, CT is the imaging modality of choice for the ED physician.
Although some tumors exhibit a characteristic appearance, do not make an unequivocal diagnosis based solely on radiologic findings. Generally, computed tomography (CT) is the imaging modality of choice for the emergency department physician. CT findings are as follows:
- Most tumors demonstrate enhancement with contrast material administration
- Tumors may appear hypodense, isodense, or hyperdense or have mixed density
- Metastases to the brain tend to be multiple, but certain tumors (eg, renal cell carcinomas) tend to produce solitary metastatic brain lesions
As magnetic resonance imaging (MRI) becomes increasingly available, it may supplant CT as the imaging procedure of choice. Features of MRI for imaging intracranial neoplasms are as follows:
- MRI is most helpful for identifying tumors in the posterior fossa (including acoustic neuromas) and hemorrhagic lesions
- MRI is useful in patients with an allergy to iodinated contrast material or renal insufficiency
- Drawbacks to MRI include incompatibility with certain medical equipment, longer imaging times (increased risk of motion artifact), and poor visualization of the subarachnoid space
- Neither CT nor MRI can be used to differentiate tumor recurrence from radionecrosis
See Workup for more detail.
Management
Acute treatment for cerebral edema from intracranial neoplasms is as follows:
- Corticosteroids may dramatically reduce signs and symptoms, bringing relief within a few hours
- Dexamethasone is the agent of choice
- Recommended doses generally range from 4-24 mg daily
Definitive treatment is as follows:
- Generally, care of patients with a brain tumor is multidisciplinary, requiring assistance from a neurosurgeon, an oncologist, a radiologist, and an expert in radiation therapy
- Management varies greatly depending on tumor location, tissue type, and comorbid conditions
- Surgical treatment options may include tumor removal or debulking, installation of a ventricular shunt, and placement of radioactive implants
See Treatment and Medication for more detail.
For patient education resources, see Brain Cancer.