Asthma: Practice Essentials, Background, Anatomy (original) (raw)
Practice Essentials
Asthma is a common chronic disease worldwide and affects approximately 25 million persons in the United States. [1] It is the most common chronic disease in childhood, affecting an estimated 6 million US children. The pathophysiology of asthma is complex and involves airway inflammation, intermittent airflow obstruction, and bronchial hyperresponsiveness. See the image below.
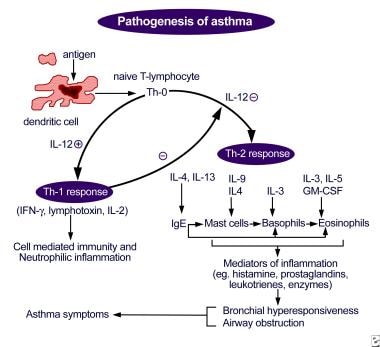
Pathogenesis of asthma. Antigen presentation by the dendritic cell with the lymphocyte and cytokine response leading to airway inflammation and asthma symptoms.
Signs and symptoms
Signs and symptoms of asthma include the following:
- Wheezing
- Coughing
- Shortness of breath
- Chest tightness/pain
Other nonspecific symptoms in infants or young children may be a history of recurrent bronchitis, bronchiolitis, or pneumonia; a persistent cough with colds; and/or recurrent croup or chest rattling.
See Clinical Presentation for more detail.
Diagnosis
Updated guidelines from the National Asthma Education and Prevention Program (NAEPP) highlight the importance of correctly diagnosing asthma, by establishing the following: [2]
- Episodic symptoms of airflow obstruction are present
- Airflow obstruction or symptoms are at least partially reversible
- Exclusion of alternative diagnoses
Spirometry with postbronchodilator response should be obtained as the primary test to establish the asthma diagnosis. Pulse oximetry measurement is desirable in all patients with acute asthma to exclude hypoxemia. The chest radiograph remains the initial imaging evaluation in most individuals with symptoms of asthma, but in most patients with asthma, chest radiography findings are normal or may indicate hyperinflation. Exercise spirometry is the standard method for assessing patients with exercise-induced bronchoconstriction.
See Workup for more detail.
Management
For all but the most severely affected patients, the ultimate goal is to prevent symptoms, minimize morbidity from acute episodes, and prevent functional and psychological morbidity to provide a healthy (or near healthy) lifestyle appropriate to the age of child.
Pharmacologic treatment
Pharmacologic management includes the use of relief and control agents. Control agents include inhaled corticosteroids, long-acting bronchodilators (beta-agonists and anticholinergics), theophylline (Theo-24, Theochron, Uniphyl), leukotriene modifiers, anti-IgE antibodies, anti-interleukin (IL)–5 antibodies, and anti–IL-4/IL-13 antibodies. Relief medications include short-acting bronchodilators, systemic corticosteroids, and ipratropium (Atrovent).
The pharmacologic treatment of asthma is based on stepwise therapy. Asthma medications should be added or deleted as the frequency and severity of the patient's symptoms change.
Allergen avoidance
Environmental exposures and irritants can play a strong role in symptom exacerbations. The use of skin testing or in vitro testing to assess sensitivity to perennial indoor allergens is important. Once the offending allergens are identified, counsel patients on how to avoid them. Efforts should focus on the home, where specific triggers include dust mites, animals, cockroaches, mold, and pollen.
See Treatment and Medication for more detail.
![]()
Background
Asthma is a common chronic disease worldwide and affects approximately 25 million persons in the United States. It is the most common chronic disease in childhood, affecting an estimated 4.7 million children, and it is a common cause of hospitalization for children in the United States. [1]
The pathophysiology of asthma is complex and involves airway inflammation, intermittent airflow obstruction, and bronchial hyperresponsiveness. The mechanism of inflammation in asthma may be acute, subacute, or chronic, and the presence of airway edema and mucus secretion also contributes to airflow obstruction and bronchial reactivity. Varying degrees of mononuclear cell and eosinophil infiltration, mucus hypersecretion, desquamation of the epithelium, smooth muscle hyperplasia, and airway remodeling are present. [3, 4, 5]
Airway hyperresponsiveness or bronchial hyperreactivity in asthma is an exaggerated response to numerous exogenous and endogenous stimuli. The mechanisms involved include direct stimulation of airway smooth muscle and indirect stimulation by pharmacologically active substances from mediator-secreting cells such as mast cells or nonmyelinated sensory neurons. The degree of airway hyperresponsiveness generally correlates with the clinical severity of asthma.
Spirometry with postbronchodilator response should be obtained as the primary test to establish the asthma diagnosis. Pulse oximetry measurement is desirable in all patients with acute asthma to exclude hypoxemia. The chest radiograph remains the initial imaging evaluation in most individuals with symptoms of asthma, but in most patients with asthma, chest radiography findings are normal or may indicate hyperinflation. Exercise spirometry is the standard method for assessing patients with exercise-induced bronchospasm.
Physical findings vary with the severity of the asthma and with the absence or presence of an acute episode and its severity. The severity of asthma is classified as intermittent, mild persistent, moderate persistent, or severe persistent. Patients with asthma of any level of severity may have mild, moderate, or severe exacerbations.
Pharmacologic management includes the use of relief and control agents. Control agents include inhaled corticosteroids, long-acting bronchodilators (beta-agonists and anticholinergics), theophylline (Theo-24, Theochron, Uniphyl), leukotriene modifiers, anti-IgE antibodies, anti–IL-5 antibodies, and anti–IL-4/IL-13 antibodies. Relief medications include short-acting bronchodilators, systemic corticosteroids, and ipratropium (Atrovent). With severe exacerbations, indications for hospitalization are based on findings after the patient receives 3 doses of an inhaled bronchodilator. In general, patients should be assessed every 1-6 months for asthma control.
![]()
Anatomy
The airways of the lungs consist of the cartilaginous bronchi, membranous bronchi, and gas-exchanging bronchi termed the respiratory bronchioles and alveolar ducts. While the first 2 types function mostly as anatomic dead space, they also contribute to airway resistance. The smallest non-gas-exchanging airways, the terminal bronchioles, are approximately 0.5 mm in diameter; airways are considered small if they are less than 2 mm in diameter. [6]
Airway structure consists of the following:
- Mucosa, which is composed of epithelial cells that are capable of specialized mucous production and a transport apparatus
- Basement membrane
- A smooth-muscle matrix extending to the alveolar entrances
- Predominantly fibrocartilaginous or fibroelastic-supporting connective tissue.
Cellular elements include mast cells, which are involved in the complex control of releasing histamine and other mediators. Basophils, eosinophils, neutrophils, and macrophages also are responsible for extensive mediator release in the early and late stages of bronchial asthma. Stretch and irritant receptors reside in the airways, as do cholinergic motor nerves, which innervate the smooth muscle and glandular units. In bronchial asthma, smooth muscle contraction in an airway is greater than that expected for its size if it were functioning normally, and this contraction varies in its distribution.
![]()
Pathophysiology
The 2020 Expert Panel Report 3 (EPR-3) of the National Asthma Education and Prevention Program (NAEPP) noted several key changes in the understanding of the pathophysiology of asthma: [2]
- The critical role of inflammation has been further substantiated, but evidence is emerging for considerable variability in the pattern of inflammation, thus indicating phenotypic differences that may influence treatment responses
- Of the environmental factors, allergic reactions remain important. Evidence also suggests a key and expanding role for viral respiratory infections in these processes
- The onset of asthma for most patients begins early in life, with the pattern of disease persistence determined by early, recognizable risk factors including atopic disease, recurrent wheezing, and a parental history of asthma
- Current asthma treatment with anti-inflammatory therapy does not appear to prevent progression of the underlying disease severity
The pathophysiology of asthma is complex and involves the following components:
- Airway inflammation
- Intermittent airflow obstruction
- Bronchial hyperresponsiveness
Airway inflammation
The mechanism of inflammation in asthma may be acute, subacute, or chronic, and the presence of airway edema and mucus secretion also contributes to airflow obstruction and bronchial reactivity. Varying degrees of mononuclear cell and eosinophil infiltration, mucus hypersecretion, desquamation of the epithelium, smooth muscle hyperplasia, and airway remodeling are present. [3] See the image below.
Pathogenesis of asthma. Antigen presentation by the dendritic cell with the lymphocyte and cytokine response leading to airway inflammation and asthma symptoms.
Some of the principal cells identified in airway inflammation include mast cells, eosinophils, epithelial cells, macrophages, and activated T lymphocytes. T lymphocytes play an important role in the regulation of airway inflammation through the release of numerous cytokines. Other constituent airway cells, such as fibroblasts, endothelial cells, and epithelial cells, contribute to the chronicity of the disease. Other factors, such as adhesion molecules (eg, selectins, integrins), are critical in directing the inflammatory changes in the airway. Finally, cell-derived mediators influence smooth muscle tone and produce structural changes and remodeling of the airway.
The presence of airway hyperresponsiveness or bronchial hyperreactivity in asthma is an exaggerated response to numerous exogenous and endogenous stimuli. The mechanisms involved include direct stimulation of airway smooth muscle and indirect stimulation by pharmacologically active substances from mediator-secreting cells such as mast cells or nonmyelinated sensory neurons. The degree of airway hyperresponsiveness generally correlates with the clinical severity of asthma.
A study by Balzar et al reported changes in airway resident mast cell populations from a large group of subjects with asthma and normal control subjects. [7] A greater proportion of chymase-positive mast cells in the airways and increased prostaglandin D2 levels were identified as important predictors of severe asthma as compared with other steroid-treated subjects with asthma.
Chronic inflammation of the airways is associated with increased bronchial hyperresponsiveness, which leads to bronchospasm and typical symptoms of wheezing, shortness of breath, and coughing after exposure to allergens, environmental irritants, viruses, cold air, or exercise. In some patients with chronic asthma, airflow limitation may be only partially reversible because of airway remodeling (hypertrophy and hyperplasia of smooth muscle, angiogenesis, and subepithelial fibrosis) that occurs with chronic untreated disease.
Airway inflammation in asthma may represent a loss of normal balance between two "opposing" populations of Th lymphocytes. Two types of Th lymphocytes have been characterized: Th1 and Th2. Th1 cells produce interleukin (IL)-2 and IFN-α, which are critical in cellular defense mechanisms in response to infection. Th2, in contrast, generates a family of cytokines (IL-4, IL-5, IL-6, IL-9, and IL-13) that can mediate allergic inflammation. A study by Gauvreau et al found that IL-13 has a role in allergen-induced airway responses. [8]
The current "hygiene hypothesis" of asthma illustrates how this cytokine imbalance may explain some of the dramatic increases in asthma prevalence in westernized countries. [9] This hypothesis is based on the concept that the immune system of the newborn is skewed toward Th2 cytokine generation (mediators of allergic inflammation). Following birth, environmental stimuli such as infections activate Th1 responses and bring the Th1/Th2 relationship to an appropriate balance. However, unequivocal support for the "hypgiene hypothesis" has not been demonstrated. [10]
Airflow obstruction
Airflow obstruction can be caused by a variety of changes, including acute bronchoconstriction, airway edema, chronic mucous plug formation, and airway remodeling. Acute bronchoconstriction is the consequence of immunoglobulin E-dependent mediator release upon exposure to aeroallergens and is the primary component of the early asthmatic response. Airway edema occurs 6-24 hours following an allergen challenge and is referred to as the late asthmatic response. Chronic mucous plug formation consists of an exudate of serum proteins and cell debris that may take weeks to resolve. Airway remodeling is associated with structural changes due to long-standing inflammation and may profoundly affect the extent of reversibility of airway obstruction. [11]
Airway obstruction causes increased resistance to airflow and decreased expiratory flow rates. These changes lead to a decreased ability to expel air and may result in hyperinflation. The resulting overdistention helps maintain airway patency, thereby improving expiratory flow; however, it also alters pulmonary mechanics and increases the work of breathing.
Bronchial hyperresponsiveness
Hyperinflation compensates for the airflow obstruction, but this compensation is limited when the tidal volume approaches the volume of the pulmonary dead space; the result is alveolar hypoventilation. Uneven changes in airflow resistance, the resulting uneven distribution of air, and alterations in circulation from increased intra-alveolar pressure due to hyperinflation all lead to ventilation-perfusion mismatch. Vasoconstriction due to alveolar hypoxia also contributes to this mismatch. Vasoconstriction is also considered an adaptive response to ventilation/perfusion mismatch.
In the early stages, when ventilation-perfusion mismatch results in hypoxia, hypercarbia is prevented by the ready diffusion of carbon dioxide across alveolar capillary membranes. Thus, patients with asthma who are in the early stages of an acute episode have hypoxemia in the absence of carbon dioxide retention. Hyperventilation triggered by the hypoxic drive also causes a decrease in PaCO2. An increase in alveolar ventilation in the early stages of an acute exacerbation prevents hypercarbia. With worsening obstruction and increasing ventilation-perfusion mismatch, carbon dioxide retention occurs. In the early stages of an acute episode, respiratory alkalosis results from hyperventilation. Later, the increased work of breathing, increased oxygen consumption, and increased cardiac output result in metabolic acidosis. Respiratory failure leads to respiratory acidosis due to retention of carbon dioxide as alveolar ventilation decreases.
![]()
Etiology
Factors that can contribute to asthma or airway hyperreactivity may include any of the following:
- Environmental allergens (eg, house dust mites; animal allergens, especially cat and dog; cockroach allergens; and fungi)
- Viral respiratory tract infections
- Exercise, hyperventilation
- Gastroesophageal reflux disease
- Chronic sinusitis or rhinitis
- Aspirin or nonsteroidal anti-inflammatory drug (NSAID) hypersensitivity, sulfite sensitivity
- Use of beta-adrenergic receptor blockers (including ophthalmic preparations)
- Obesity [12]
- Environmental pollutants, tobacco smoke
- Occupational exposure
- Irritants (eg, household sprays, paint fumes)
- Various high- and low-molecular-weight compounds (eg, insects, plants, latex, gums, diisocyanates, anhydrides, wood dust, and fluxes; associated with occupational asthma)
- Emotional factors or stress
- Perinatal factors (prematurity and increased maternal age; maternal smoking and prenatal exposure to tobacco smoke; breastfeeding has not been definitely shown to be protective)
Aspirin-induced asthma
The triad of asthma, aspirin sensitivity, and nasal polyps affects 5-10% of patients with asthma. Most patients experience symptoms during the third to fourth decade. A single dose can provoke an acute asthma exacerbation, accompanied by rhinorrhea, conjunctival irritation, and flushing of the head and neck. It can also occur with other nonsteroidal anti-inflammatory drugs and is caused by an increase in eosinophils and cysteinyl leukotrienes after exposure. [13]
A study by Beasley et al demonstrated some epidemiological evidence that exposure to acetaminophen is associated with an increased risk of asthma. [14] However, no clinical studies have directly linked asthma symptoms with acetaminophen use.
Primary treatment is avoidance of these medications, but leukotriene antagonists have shown promise in treatment, allowing these patients to take daily aspirin for cardiac or rheumatic disease. Aspirin desensitization has also been reported to decrease sinus symptoms, allowing daily dosing of aspirin. [15]
Gastroesophageal reflux disease
The presence of acid in the distal esophagus, mediated via vagal or other neural reflexes, can significantly increase airway resistance and airway reactivity. Patients with asthma are 3 times more likely to also have GERD. [16] Some people with asthma have significant gastroesophageal reflux without esophageal symptoms. Gastroesophageal reflux was found to be a definite asthma-causing factor (defined by a favorable asthma response to medical antireflux therapy) in 64% of patients; clinically silent reflux was present in 24% of all patients. [16]
Work-related asthma
Occupational factors are associated with 10-15% of adult asthma cases. More than 300 specific occupational agents have been associated with asthma. High-risk jobs include farming, painting, janitorial work, and plastics manufacturing. Given the prevalence of work-related asthma, the American College of Chest Physicians (ACCP) supports consideration of work-related asthma in all patients presenting with new-onset or worsening asthma. An ACCP consensus statement defines work-related asthmas as including occupational asthma (ie, asthma induced by sensitizer or irritant work exposures) and work-exacerbated asthma (ie, preexisting or concurrent asthma worsened by work factors). [17]
Two types of occupational asthma are recognized: immune-related and non-immune-related. Immune-mediated asthma has a latency of months to years after exposure. Non-immune-mediated asthma, or irritant-induced asthma (reactive airway dysfunction syndrome), has no latency period and may occur within 24 hours after an accidental exposure to high concentrations of respiratory irritants. Pay careful attention to the patient's occupational history. Those with a history of asthma who report worsening of symptoms during the week and improvement during the weekends should be evaluated for occupational exposure. Peak-flow monitoring during work (optimally, at least 4 times a day) for at least 2 weeks and a similar period away from work is one recommended method to establish the diagnosis. [17]
To see complete information on Allergic and Environmental Asthma, please go to the main article by clicking here.
Viral exposure in children
Evidence suggests that rhinovirus illness during infancy is a significant risk factor for the development of wheezing in preschool children and a frequent trigger of wheezing illnesses in children with asthma. [18] Human rhinovirus C (HRVC) is a newly identified genotype of HRV found in patients with respiratory tract infections. A study of children with acute asthma who presented to the emergency department found HRVC present in the majority of patients. The presence of HRVC was also associated with more severe asthma. [19]
Approximately 80-85% of childhood asthma episodes are associated with prior viral exposure. Prior childhood pneumonia due to infection by respiratory syncytial virus, Mycoplasma pneumoniae, and/or Chlamydia species was found in more than 50% of a small sample of children aged 7-9 years who later had asthma. [20] Treatment with antibiotics appropriate for these organisms improves the clinical signs and symptoms of asthma.
Sinusitis
Of patients with asthma, 50% have concurrent sinus disease. Sinusitis is the most important exacerbating factor for asthma symptoms. Either acute infectious sinus disease or chronic inflammation may contribute to worsening airway symptoms. Treatment of nasal and sinus inflammation reduces airway reactivity. Treatment of acute sinusitis requires at least 10 days of antibiotics to improve asthma symptoms. [21]
Exercise-induced asthma
Exercise-induced asthma (EIA), or exercise-induced bronchoconstriction (EIB), is an asthma variant defined as a condition in which exercise or vigorous physical activity triggers acute bronchoconstriction in persons with heightened airway reactivity. It is observed primarily in persons who have asthma (exercise-induced bronchoconstriction in asthmatic persons) but can also be found in patients with normal resting spirometry findings with atopy, allergic rhinitis, or cystic fibrosis and even in healthy persons, many of whom are elite or cold weather athletes (exercise-induced bronchoconstriction in athletes). Exercise-induced bronchoconstriction is often a neglected diagnosis, and the underlying asthma may be silent in as many as 50% of patients, except during exercise. [22, 23]
The pathogenesis of exercise-induced bronchoconstriction is controversial. The disease may be mediated by water loss from the airway, heat loss from the airway, or a combination of both. The upper airway is designed to keep inspired air at 100% humidity and body temperature at 37°C (98.6°F). The nose is unable to condition the increased amount of air required for exercise, particularly in athletes who breathe through their mouths. The abnormal heat and water fluxes in the bronchial tree result in bronchoconstriction, occurring within minutes of completing exercise. Results from bronchoalveolar lavage studies have not demonstrated an increase in inflammatory mediators. These patients generally develop a refractory period, during which a second exercise challenge does not cause a significant degree of bronchoconstriction.
Factors that contribute to exercise-induced bronchoconstriction symptoms (in both persons with asthma and athletes) include the following:
- Exposure to cold or dry air
- Environmental pollutants (eg, sulfur, ozone)
- level of bronchial hyperreactivity
- Chronicity of asthma and symptomatic control
- Duration and intensity of exercise
- Allergen exposure in atopic individuals
- Coexisting respiratory infection
The assessment and diagnosis of exercise-induced bronchoconstriction is made more often in children and young adults than in older adults and is related to high levels of physical activity. Exercise-induced bronchoconstriction can be observed in persons of any age based on the level of underlying airway reactivity and the level of physical exertion.
Genetics
Research on genetic mutations casts further light on the synergistic nature of multiple mutations in the pathophysiology of asthma. Polymorphisms in the gene that encodes platelet-activating factor hydrolase, an intrinsic neutralizing agent of platelet-activating factor in most humans, may play a role in susceptibility to asthma and asthma severity. [24]
Evidence suggests that the prevalence of asthma is reduced in association with certain infections (Mycobacterium tuberculosis, measles, or hepatitis A); rural living; exposure to other children (eg, presence of older siblings and early enrollment in childcare); and less frequent use of antibiotics. Furthermore, the absence of these lifestyle events is associated with the persistence of a Th2 cytokine pattern. Under these conditions, the genetic background of the child, with a cytokine imbalance toward Th2, sets the stage to promote the production of immunoglobulin E (IgE) antibody to key environmental antigens (eg, dust mites, cockroaches, Alternaria, and possibly cats). Therefore, a gene-by-environment interaction occurs in which the susceptible host is exposed to environmental factors that are capable of generating IgE, and sensitization occurs.
A reciprocal interaction is apparent between the 2 subpopulations, in which Th1 cytokines can inhibit Th2 generation and vice versa. Allergic inflammation may be the result of an excessive expression of Th2 cytokines. Alternatively, studies suggest the possibility that the loss of normal immune balance arises from a cytokine dysregulation in which Th1 activity in asthma is diminished. [25]
In addition, some studies highlight the importance of genotypes in children's susceptibility to asthma and response to specific antiasthma medications. [27, 28, 29]
Obesity
A study by Cottrell et al explored the relationship between asthma, obesity, and abnormal lipid and glucose metabolism. [30] The study found that community-based data linked asthma, body mass, and metabolic variables in children. Specifically, these findings described a statistically significant association between asthma and abnormal lipid and glucose metabolism beyond body mass association. Evidence is accumulating that individuals with a high body mass index have worse asthma control and sustained weight loss improves asthma control. [31]
Accelerated weight gain in early infancy is associated with increased risks of asthma symptoms according to one study of preschool children. [32]
![]()
Epidemiology
Asthma affects 5-10% of the US population or an estimated 25 million persons, including 4.7 million children. [1, 17] The overall prevalence rate of exercise-induced bronchospasm is 3-10% of the general population if persons who do not have asthma or allergy are excluded, but the rate increases to 12-15% of the general population if patients with underlying asthma are included. Asthma affects an estimated 300 million individuals worldwide. Annually, the World Health Organization (WHO) has estimated that 15 million disability-adjusted life-years are lost and 250,000 asthma deaths are reported worldwide. [33]
In the United States, asthma prevalence, especially morbidity and mortality, is higher in blacks than in whites. Although genetic factors are of major importance in determining a predisposition to the development of asthma, environmental factors play a greater role than racial factors in asthma onset. A national concern is that some of the increased morbidity is due to differences in asthma treatment afforded certain minority groups. Larger asthma-associated lung function deficits are reported in Hispanics, especially females. [34]
Asthma is common in industrialized nations such as Canada, England, Australia, Germany, and New Zealand, where much of the asthma data have been collected. The prevalence rate of severe asthma in industrialized countries ranges from 2-10%. Trends suggest an increase in both the prevalence and morbidity of asthma, especially in children younger than 6 years. Factors that have been implicated include urbanization, air pollution, passive smoking, and change in exposure to environmental allergens.
Asthma predominantly occurs in boys in childhood, with a male-to-female ratio of 2:1 until puberty, when the male-to-female ratio becomes 1:1. Asthma prevalence is greater in females after puberty, and the majority of adult-onset cases diagnosed in persons older than 40 years occur in females. Boys are more likely than girls to experience a decrease in symptoms by late adolescence.
Asthma prevalence is increased in very young persons and very old persons because of airway responsiveness and lower levels of lung function. [35] Two thirds of all asthma cases are diagnosed before the patient is aged 18 years. Approximately half of all children diagnosed with asthma have a decrease or disappearance of symptoms by early adulthood. [36]
![]()
Prognosis
International asthma mortality is reported as high as 0.86 deaths per 100,000 persons in some countries. US asthma mortality rates in 2009 were reported at 1 death per 100,000 persons. Mortality is primarily related to lung function, with an 8-fold increase in patients in the lowest quartile, but mortality has also been linked with asthma management failure, especially in young persons. Other factors that impact mortality include age older than 40 years, cigarette smoking more than 20 pack-years, blood eosinophilia, forced expiratory volume in one second (FEV1) of 40-69% predicted, and greater reversibility. [37]
The estimate of lost work and school time from asthma is approximately 100 million days of restricted activity. Approximately 500,000 annual hospitalizations (40.6% in individuals aged 18 y or younger) are due to asthma. Each year, an estimated 1.7 million people (47.8% of them aged 18 years or younger) require treatment in an emergency department. [38] For 2019-2020, the annual expenditures for healthcare utilization due to asthma and COPD was an estimated $82.0 billion. [39]
Nearly one half of children diagnosed with asthma will have a decrease in symptoms and require less treatment by late adolescence or early adulthood. In a study of 900 children with asthma, 6% required no treatment after 1 year, and 39% only required intermittent treatment.
Patients with poorly controlled asthma develop long-term changes over time (i.e., with airway remodeling). This can lead to chronic symptoms and a significant irreversible component to their disease. Many patients who develop asthma at an older age also tend to have chronic symptoms.
![]()
Patient Education
The need for patient education about asthma and the establishment of a partnership between patient and clinician in the management of the disease was emphasized by the National Asthma Education and Prevention Program Coordinating Committee (NAEPPCC) in its updated 2020 guidelines. [2]
The key points of education include the following:
- Patient education should be integrated into every aspect of asthma care
- All members of the healthcare team, including nurses, pharmacists, and respiratory therapists, should provide education.
- Clinicians should teach patients asthma self-management based on basic asthma facts, self-monitoring techniques, the role of medications, inhaler use, and environmental control measures. [40, 41, 42]
- Treatment goals should be developed for the patient and family.
- A written, individualized, daily self-management plan should be developed.
- Several well-validated asthma action plans are now available and are key in the management of asthma and should therefore be reviewed: ACT (Asthma Control Test), ATAQ (Asthma Therapy Assessment Questionnaire), and ACQ (Asthma Control Questionnaire). [43]
School-based asthma education programs improved knowledge of asthma, self-efficacy, and self-management behaviors in children aged 4-17 years, according to a systematic literature review by Coffman et al, but the programs had less effect on quality of life, days of symptoms, nights with symptoms, and school absences. [44]
The 2019 Veterans Administration/Department of Defense (VA/DoD) clinical practice guideline for primary care management of asthma concurs with NAEPPCC in recommending self-management education for both the patient and caregiver as part of the treatment program. [45]
For patient education resources, visit the Asthma Center. Also, see the patient education articles Asthma, Asthma FAQs, Asthma in Children, and Asthma Medications.
A patient education video of an overview of asthma is provided below.
Asthma is characterized by chronic inflammation and asthma exacerbations, where an environmental trigger initiates inflammation, which makes it difficult to breathe. This video covers the pathophysiology of asthma, signs and symptoms, types, and treatment.
![]()
- CDC. Asthma: most recent national asthma data. CDC. Available at https://www.cdc.gov/asthma/most_recent_national_asthma_data.htm. May 10, 2023; Accessed: June 26, 2024.
- [Guideline] Expert Panel Working Group of the National Heart, Lung, and Blood Institute (NHLBI) administered and coordinated National Asthma Education and Prevention Program Coordinating Committee (NAEPPCC), et al. 2020 Focused Updates to the Asthma Management Guidelines: A Report from the National Asthma Education and Prevention Program Coordinating Committee Expert Panel Working Group. J Allergy Clin Immunol. 2020 Dec. 146 (6):1217-1270. [QxMD MEDLINE Link]. [Full Text].
- Han X, Krempski JW, Nadeau K. Advances and novel developments in mechanisms of allergic inflammation. Allergy. 2020 Dec. 75 (12):3100-3111. [QxMD MEDLINE Link].
- Chung KF, Adcock IM. Precision medicine for the discovery of treatable mechanisms in severe asthma. Allergy. 2019 Sep. 74 (9):1649-1659. [QxMD MEDLINE Link].
- Cevhertas L, Ogulur I, Maurer DJ, Burla D, Ding M, Jansen K, et al. Advances and recent developments in asthma in 2020. Allergy. 2020 Dec. 75 (12):3124-3146. [QxMD MEDLINE Link].
- Postma DS, Brightling C, Baldi S, Van den Berge M, Fabbri LM, Gagnatelli A, et al. Exploring the relevance and extent of small airways dysfunction in asthma (ATLANTIS): baseline data from a prospective cohort study. Lancet Respir Med. 2019 May. 7 (5):402-416. [QxMD MEDLINE Link].
- Balzar S, Fajt ML, Comhair SA, Erzurum SC, Bleecker E, Busse WW, et al. Mast cell phenotype, location, and activation in severe asthma: data from the severe asthma research program. Am J Respir Crit Care Med. 2011 Feb 1. 183(3):299-309. [QxMD MEDLINE Link]. [Full Text].
- Gauvreau GM, Boulet LP, Cockcroft DW, et al. Effects of Interleukin-13 Blockade on Allergen-induced Airway Responses in Mild Atopic Asthma. Am J Respir Crit Care Med. 2011 Apr 15. 183(8):1007-14. [QxMD MEDLINE Link].
- Anderson WJ, Watson L. Asthma and the hygiene hypothesis. N Engl J Med. 2001 May 24. 344(21):1643-4. [QxMD MEDLINE Link].
- Brooks C, Pearce N, Douwes J. The hygiene hypothesis in allergy and asthma: an update. Curr Opin Allergy Clin Immunol. 2013 Feb. 13 (1):70-7. [QxMD MEDLINE Link].
- Sears MR. Consequences of long-term inflammation. The natural history of asthma. Clin Chest Med. 2000 Jun. 21(2):315-29. [QxMD MEDLINE Link].
- Camargo CA Jr, Weiss ST, Zhang S, Willett WC, Speizer FE. Prospective study of body mass index, weight change, and risk of adult-onset asthma in women. Arch Intern Med. 1999 Nov 22. 159(21):2582-8. [QxMD MEDLINE Link].
- Henderson WR Jr. Role of leukotrienes in asthma. Ann Allergy. 1994 Mar. 72(3):272-8. [QxMD MEDLINE Link].
- Beasley RW, Clayton TO, Crane J, Lai CK, Montefort SR, Mutius E, et al. Acetaminophen use and risk of asthma, rhinoconjunctivitis, and eczema in adolescents: international study of asthma and allergies in childhood phase three. Am J Respir Crit Care Med. 2011 Jan 15. 183(2):171-8. [QxMD MEDLINE Link].
- Comert S, Karakaya G. Kalyoncu AF. Aspirin desensitization treatment for the management of aspirin-exacerbated respiratory disease. J Respir Res. 2016. 2:24-7.
- Harding SM, Guzzo MR, Richter JE. The prevalence of gastroesophageal reflux in asthma patients without reflux symptoms. Am J Respir Crit Care Med. 2000 Jul. 162(1):34-9. [QxMD MEDLINE Link].
- Tarlo SM, Balmes J, Balkissoon R, Beach J, Beckett W, Bernstein D, et al. Diagnosis and management of work-related asthma: American College Of Chest Physicians Consensus Statement. Chest. 2008 Sep. 134(3 Suppl):1S-41S. [QxMD MEDLINE Link].
- Lemanske RF Jr, Jackson DJ, Gangnon RE, Evans MD, Li Z, Shult PA, et al. Rhinovirus illnesses during infancy predict subsequent childhood wheezing. J Allergy Clin Immunol. 2005 Sep. 116(3):571-7. [QxMD MEDLINE Link].
- Bizzintino J, Lee WM, Laing IA, Vang F, Pappas T, Zhang G, et al. Association between human rhinovirus C and severity of acute asthma in children. Eur Respir J. 2011 May. 37(5):1037-42. [QxMD MEDLINE Link]. [Full Text].
- Martin RJ, Kraft M, Chu HW, Berns EA, Cassell GH. A link between chronic asthma and chronic infection. J Allergy Clin Immunol. 2001 Apr. 107(4):595-601. [QxMD MEDLINE Link].
- Hamilos DL. Gastroesophageal reflux and sinusitis in asthma. Clin Chest Med. 1995 Dec. 16(4):683-97. [QxMD MEDLINE Link].
- McFadden ER Jr. Exercise-induced airway obstruction. Clin Chest Med. 1995 Dec. 16(4):671-82. [QxMD MEDLINE Link].
- Randolph C. Exercise-induced asthma: update on pathophysiology, clinical diagnosis, and treatment. Curr Probl Pediatr. 1997 Feb. 27(2):53-77. [QxMD MEDLINE Link].
- Ito S, Noguchi E, Shibasaki M, Yamakawa-Kobayashi K, Watanabe H, Arinami T. Evidence for an association between plasma platelet-activating factor acetylhydrolase deficiency and increased risk of childhood atopic asthma. J Hum Genet. 2002. 47(2):99-101. [QxMD MEDLINE Link].
- Bousquet J, Jeffery PK, Busse WW, Johnson M, Vignola AM. Asthma. From bronchoconstriction to airways inflammation and remodeling. Am J Respir Crit Care Med. 2000 May. 161(5):1720-45. [QxMD MEDLINE Link].
- Drazen JM, Yandava CN, Dube L, Szczerback N, Hippensteel R, Pillari A, et al. Pharmacogenetic association between ALOX5 promoter genotype and the response to anti-asthma treatment. Nat Genet. 1999 Jun. 22(2):168-70. [QxMD MEDLINE Link].
- Thompson EE, Pan L, Ostrovnaya I, Weiss LA, Gern JE, Lemanske RF Jr, et al. Integrin beta 3 genotype influences asthma and allergy phenotypes in the first 6 years of life. J Allergy Clin Immunol. 2007 Jun. 119(6):1423-9. [QxMD MEDLINE Link].
- Wechsler ME, Lehman E, Lazarus SC, Lemanske RF Jr, Boushey HA, Deykin A, et al. beta-Adrenergic receptor polymorphisms and response to salmeterol. Am J Respir Crit Care Med. 2006 Mar 1. 173(5):519-26. [QxMD MEDLINE Link]. [Full Text].
- Cottrell L, Neal WA, Ice C, Perez MK, Piedimonte G. Metabolic abnormalities in children with asthma. Am J Respir Crit Care Med. 2011 Feb 15. 183(4):441-8. [QxMD MEDLINE Link]. [Full Text].
- Juel CT, Ali Z, Nilas L, Ulrik CS. Asthma and obesity: does weight loss improve asthma control? a systematic review. J Asthma Allergy. 2012. 5:21-6. [QxMD MEDLINE Link].
- Sonnenschein-van der Voort AM, Jaddoe VW, Raat H, Moll HA, Hofman A, de Jongste JC, et al. Fetal and infant growth and asthma symptoms in preschool children: the generation R study. Am J Respir Crit Care Med. 2012 Apr 1. 185(7):731-7. [QxMD MEDLINE Link].
- Bateman ED, Hurd SS, Barnes PJ, Bousquet J, Drazen JM, FitzGerald M, et al. Global strategy for asthma management and prevention: GINA executive summary. Eur Respir J. 2008 Jan. 31(1):143-78. [QxMD MEDLINE Link]. [Full Text].
- Zhang Y, McConnell R, Gilliland F, Berhane K. Ethnic differences in the effect of asthma on pulmonary function in children. Am J Respir Crit Care Med. 2011 Mar 1. 183(5):596-603. [QxMD MEDLINE Link]. [Full Text].
- Burrows B, Barbee RA, Cline MG, Knudson RJ, Lebowitz MD. Characteristics of asthma among elderly adults in a sample of the general population. Chest. 1991 Oct. 100(4):935-42. [QxMD MEDLINE Link].
- Martin AJ, Landau LI, Phelan PD. Lung function in young adults who had asthma in childhood. Am Rev Respir Dis. 1980 Oct. 122(4):609-16. [QxMD MEDLINE Link].
- Sly RM. Changing asthma mortality. Ann Allergy. 1994 Sep. 73(3):259-68. [QxMD MEDLINE Link].
- Moorman JE, Rudd RA, Johnson CA, King M, Minor P, Bailey C, et al. National surveillance for asthma--United States, 1980-2004. MMWR Surveill Summ. 2007 Oct 19. 56(8):1-54. [QxMD MEDLINE Link].
- National Heart, Lung, and Blood Institute. Aggregate Cost of Care and Healthcare Utilization. NHLBI.NIH.gov. Available at https://www.nhlbi.nih.gov/research/data/healthcare-costs. 2019-2020; Accessed: June 26, 2024.
- Bailey WC, Richards JM Jr, Brooks CM, Soong SJ, Windsor RA, Manzella BA. A randomized trial to improve self-management practices of adults with asthma. Arch Intern Med. 1990 Aug. 150(8):1664-8. [QxMD MEDLINE Link].
- Ignacio-Garcia JM, Gonzalez-Santos P. Asthma self-management education program by home monitoring of peak expiratory flow. Am J Respir Crit Care Med. 1995 Feb. 151(2 Pt 1):353-9. [QxMD MEDLINE Link].
- Kotses H, Bernstein IL, Bernstein DI, Reynolds RV, Korbee L, Wigal JK, et al. A self-management program for adult asthma. Part I: Development and evaluation. J Allergy Clin Immunol. 1995 Feb. 95(2):529-40. [QxMD MEDLINE Link].
- Nathan RA, Sorkness CA, Kosinski M, Schatz M, Li JT, Marcus P, et al. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. 2004 Jan. 113(1):59-65. [QxMD MEDLINE Link].
- Coffman JM, Cabana MD, Yelin EH. Do school-based asthma education programs improve self-management and health outcomes?. Pediatrics. 2009 Aug. 124(2):729-42. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] The Primary Care Management of Asthma Working Group. VA/DoD Clinical Practice Guideline for the Primary Care Management of Asthma. Version 3.0--2019. Washington (DC): Department of Veteran Affairs, Department of Defense; [Full Text].
- Font-Ribera L, Villanueva CM, Nieuwenhuijsen MJ, et al. Swimming pool attendance, asthma, allergies, and lung function in the Avon Longitudinal Study of Parents and Children cohort. Am J Respir Crit Care Med. 2011 Mar 1. 183(5):582-8. [QxMD MEDLINE Link]. [Full Text].
- Shao W, Chung T, Berdon WE, Mellins RB, Griscom NT, Ruzal-Shapiro C, et al. Fluoroscopic diagnosis of laryngeal asthma (paradoxical vocal cord motion). AJR Am J Roentgenol. 1995 Nov. 165(5):1229-31. [QxMD MEDLINE Link].
- Morris MJ, Deal LE, Bean DR, Grbach VX, Morgan JA. Vocal cord dysfunction in patients with exertional dyspnea. Chest. 1999 Dec. 116(6):1676-82. [QxMD MEDLINE Link].
- Nastasi KJ, Howard DA, Raby RB, Lew DB, Blaiss MS. Airway fluoroscopic diagnosis of vocal cord dysfunction syndrome. Ann Allergy Asthma Immunol. 1997 Jun. 78(6):586-8. [QxMD MEDLINE Link].
- Wynn SR, O'Connell EJ, Frigas E, Payne WS, Sachs MI. Exercise-induced "asthma" as a presentation of bronchial carcinoid. Ann Allergy. 1986 Aug. 57(2):139-41. [QxMD MEDLINE Link].
- Rolfe LM, Rayner CF. A wheezy man with a bony abnormality. Postgrad Med J. 1999 Aug. 75(886):503-4. [QxMD MEDLINE Link]. [Full Text].
- Tucker GF Jr. Pulmonary migraine. Ann Otol Rhinol Laryngol. 1977 Sep-Oct. 86(5 Pt 1):671-6. [QxMD MEDLINE Link].
- Isselbacher KJ. Harrison's Principles of Internal Medicine. Braunwald E, Wilson JD, et al. Heart failure. 13th. McGraw-Hill; 1994. 1001.
- Kim YW, Han SK, Shim YS, Kim KY, Han YC, Seo JW, et al. The first report of diffuse panbronchiolitis in Korea: five case reports. Intern Med. 1992 May. 31(5):695-701. [QxMD MEDLINE Link].
- Bevelaqua F, Schicchi JS, Haas F, Axen K, Levin N. Aortic arch anomaly presenting as exercise-induced asthma. Am Rev Respir Dis. 1989 Sep. 140(3):805-8. [QxMD MEDLINE Link].
- Newman LJ, Platts-Mills TA, Phillips CD, Hazen KC, Gross CW. Chronic sinusitis. Relationship of computed tomographic findings to allergy, asthma, and eosinophilia. JAMA. 1994 Feb 2. 271(5):363-7. [QxMD MEDLINE Link].
- Shapiro GG, Christie DL. Gastroesophageal reflux and asthma. Clin Rev Allergy. 1983 Mar. 1(1):39-56. [QxMD MEDLINE Link].
- Cuevas Hernández MM, Arias Hernández RM. [Pulmonary gammagraphy study in asthmatic children with gastroesophageal reflux]. Rev Alerg Mex. 2008 Nov-Dec. 55(6):229-33. [QxMD MEDLINE Link].
- Bacci E, Cianchetti S, Bartoli M, Dente FL, Di Franco A, Vagaggini B, et al. Low sputum eosinophils predict the lack of response to beclomethasone in symptomatic asthmatic patients. Chest. 2006 Mar. 129(3):565-72. [QxMD MEDLINE Link].
- Green RH, Brightling CE, McKenna S, Hargadon B, Parker D, Bradding P, et al. Asthma exacerbations and sputum eosinophil counts: a randomised controlled trial. Lancet. 2002 Nov 30. 360(9347):1715-21. [QxMD MEDLINE Link].
- Matsumoto H. Serum periostin: a novel biomarker for asthma management. Allergol Int. 2014 Jun. 63 (2):153-60. [QxMD MEDLINE Link].
- Woods AQ, Lynch DA. Asthma: an imaging update. Radiol Clin North Am. 2009 Mar. 47(2):317-29. [QxMD MEDLINE Link].
- Teel GS, Engeler CE, Tashijian JH, duCret RP. Imaging of small airways disease. Radiographics. 1996 Jan. 16(1):27-41. [QxMD MEDLINE Link].
- Enright PL, Lebowitz MD, Cockroft DW. Physiologic measures: pulmonary function tests. Asthma outcome. Am J Respir Crit Care Med. 1994 Feb. 149(2 Pt 2):S9-18; discussion S19-20. [QxMD MEDLINE Link].
- Ali SS, O'Connell C, Kass L, Graff G. Single-breath counting: a pilot study of a novel technique for measuring pulmonary function in children. Am J Emerg Med. 2011 Jan. 29(1):33-6. [QxMD MEDLINE Link].
- Crapo RO, Casaburi R, Coates AL, Enright PL, Hankinson JL, Irvin CG. Guidelines for methacholine and exercise challenge testing-1999. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, July 1999. Am J Respir Crit Care Med. 2000 Jan. 161(1):309-29. [QxMD MEDLINE Link].
- Anderson SD, Charlton B, Weiler JM, Nichols S, Spector SL, Pearlman DS, et al. Comparison of mannitol and methacholine to predict exercise-induced bronchoconstriction and a clinical diagnosis of asthma. Respir Res. 2009 Jan 23. 10:4. [QxMD MEDLINE Link].
- Smith AD, Cowan JO, Brassett KP, Herbison GP, Taylor DR. Use of exhaled nitric oxide measurements to guide treatment in chronic asthma. N Engl J Med. 2005 May 26. 352(21):2163-73. [QxMD MEDLINE Link].
- Rossi OV, Lähde S, Laitinen J, Huhti E. Contribution of chest and paranasal sinus radiographs to the management of acute asthma. Int Arch Allergy Immunol. 1994 Sep. 105(1):96-100. [QxMD MEDLINE Link].
- Pratter MR, Curley FJ, Dubois J, Irwin RS. Cause and evaluation of chronic dyspnea in a pulmonary disease clinic. Arch Intern Med. 1989 Oct. 149(10):2277-82. [QxMD MEDLINE Link].
- Irwin RS. Chronic cough due to gastroesophageal reflux disease: ACCP evidence-based clinical practice guidelines. Chest. 2006 Jan. 129(1 Suppl):80S-94S. [QxMD MEDLINE Link].
- Aras G, Kanmaz D, Kadakal F, Purisa S, Sonmez K, Tuncay E, et al. Gastroesophageal reflux disease in our asthma patients: the presence of dysphagia can influence pulmonary function. Multidiscip Respir Med. 2012 Dec 17. 7 (1):53. [QxMD MEDLINE Link].
- Price D, Musgrave SD, Shepstone L, et al. Leukotriene antagonists as first-line or add-on asthma-controller therapy. N Engl J Med. 2011 May 5. 364(18):1695-707. [QxMD MEDLINE Link].
- Chauhan BF, Ducharme FM. Anti-leukotriene agents compared to inhaled corticosteroids in the management of recurrent and/or chronic asthma in adults and children. Cochrane Database Syst Rev. 2012 May 16. 5:CD002314. [QxMD MEDLINE Link].
- Bruzzese JM, Sheares BJ, Vincent EJ, et al. Effects of a School-based Intervention for Urban Adolescents with Asthma: A Controlled Trial. Am J Respir Crit Care Med. 2011 Apr 15. 183(8):998-1006. [QxMD MEDLINE Link]. [Full Text].
- Scott M, Roberts G, Kurukulaaratchy RJ, Matthews S, Nove A, Arshad SH. Multifaceted allergen avoidance during infancy reduces asthma during childhood with the effect persisting until age 18 years. Thorax. 2012 Dec. 67(12):1046-51. [QxMD MEDLINE Link].
- McCormack MC, Breysse PN, Matsui EC, et al. Indoor particulate matter increases asthma morbidity in children with non-atopic and atopic asthma. Ann Allergy Asthma Immunol. 2011 Apr. 106(4):308-15. [QxMD MEDLINE Link].
- Tung KY, Tsai CH, Lee YL. Microsomal epoxide hydroxylase genotypes/diplotypes, traffic air pollution, and childhood asthma. Chest. 2011 Apr. 139(4):839-48. [QxMD MEDLINE Link].
- Sheikh A, Hurwitz B, Shehata Y. House dust mite avoidance measures for perennial allergic rhinitis. Cochrane Database Syst Rev. 2007 Jan 24. CD001563. [QxMD MEDLINE Link].
- Abramson MJ, Puy RM, Weiner JM. Allergen immunotherapy for asthma. Cochrane Database Syst Rev. 2003. CD001186. [QxMD MEDLINE Link].
- Abramson MJ, Puy RM, Weiner JM. Is allergen immunotherapy effective in asthma? A meta-analysis of randomized controlled trials. Am J Respir Crit Care Med. 1995 Apr. 151(4):969-74. [QxMD MEDLINE Link].
- Bruggenjurgen B, Reinhold T, Brehler R, Laake E, Wiese G, Machate U, et al. Cost-effectiveness of specific subcutaneous immunotherapy in patients with allergic rhinitis and allergic asthma. Ann Allergy Asthma Immunol. 2008 Sep. 101(3):316-24. [QxMD MEDLINE Link].
- Marcus P. Incorporating anti-IgE (omalizumab) therapy into pulmonary medicine practice: practice management implications. Chest. 2006 Feb. 129(2):466-74. [QxMD MEDLINE Link].
- Busse WW, Morgan WJ, Gergen PJ, et al. Randomized trial of omalizumab (anti-IgE) for asthma in inner-city children. N Engl J Med. 2011 Mar 17. 364(11):1005-15. [QxMD MEDLINE Link]. [Full Text].
- Hanania NA, Alpan O, Hamilos DL, et al. Omalizumab in severe allergic asthma inadequately controlled with standard therapy: a randomized trial. Ann Intern Med. 2011 May 3. 154(9):573-82. [QxMD MEDLINE Link].
- Ortega HG, Liu MC, Pavord ID, Brusselle GG, FitzGerald JM, Chetta A, et al. Mepolizumab treatment in patients with severe eosinophilic asthma. N Engl J Med. 2014 Sep 25. 371 (13):1198-207. [QxMD MEDLINE Link]. [Full Text].
- Bel EH, Wenzel SE, Thompson PJ, Prazma CM, Keene ON, Yancey SW, et al. Oral glucocorticoid-sparing effect of mepolizumab in eosinophilic asthma. N Engl J Med. 2014 Sep 25. 371 (13):1189-97. [QxMD MEDLINE Link]. [Full Text].
- Pavord ID, Korn S, Howarth P, Bleecker ER, Buhl R, Keene ON, et al. Mepolizumab for severe eosinophilic asthma (DREAM): a multicentre, double-blind, placebo-controlled trial. Lancet. 2012 Aug 18. 380 (9842):651-9. [QxMD MEDLINE Link].
- Castro M, Zangrilli J, Wechsler ME, Bateman ED, Brusselle GG, Bardin P, et al. Reslizumab for inadequately controlled asthma with elevated blood eosinophil counts: results from two multicentre, parallel, double-blind, randomised, placebo-controlled, phase 3 trials. Lancet Respir Med. 2015 May. 3 (5):355-66. [QxMD MEDLINE Link].
- Bleecker ER, FitzGerald JM, Chanez P, Papi A, Weinstein SF, Barker P, et al. Efficacy and safety of benralizumab for patients with severe asthma uncontrolled with high-dosage inhaled corticosteroids and long-acting β2-agonists (SIROCCO): a randomised, multicentre, placebo-controlled phase 3 trial. Lancet. 2016 Oct 29. 388 (10056):2115-2127. [QxMD MEDLINE Link].
- FitzGerald JM, Bleecker ER, Nair P, Korn S, Ohta K, Lommatzsch M, et al. Benralizumab, an anti-interleukin-5 receptor α monoclonal antibody, as add-on treatment for patients with severe, uncontrolled, eosinophilic asthma (CALIMA): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. 2016 Oct 29. 388 (10056):2128-2141. [QxMD MEDLINE Link].
- Nair P, Wenzel S, Rabe KF, Bourdin A, Lugogo NL, Kuna P, et al. Oral Glucocorticoid-Sparing Effect of Benralizumab in Severe Asthma. N Engl J Med. 2017 Jun 22. 376 (25):2448-2458. [QxMD MEDLINE Link].
- Castro M, Corren J, Pavord ID, Maspero J, Wenzel S, Rabe KF, et al. Dupilumab Efficacy and Safety in Moderate-to-Severe Uncontrolled Asthma. N Engl J Med. 2018 Jun 28. 378 (26):2486-2496. [QxMD MEDLINE Link].
- Rabe KF, Nair P, Brusselle G, Maspero JF, Castro M, Sher L, et al. Efficacy and Safety of Dupilumab in Glucocorticoid-Dependent Severe Asthma. N Engl J Med. 2018 Jun 28. 378 (26):2475-2485. [QxMD MEDLINE Link].
- Menzies-Gow A, Corren J, Bourdin A, Chupp G, Israel E, Wechsler ME, et al. Tezepelumab in Adults and Adolescents with Severe, Uncontrolled Asthma. N Engl J Med. 2021 May 13. 384 (19):1800-1809. [QxMD MEDLINE Link]. [Full Text].
- Castro M, Rubin AS, Laviolette M, Fiterman J, De Andrade Lima M, Shah PL, et al. Effectiveness and safety of bronchial thermoplasty in the treatment of severe asthma: a multicenter, randomized, double-blind, sham-controlled clinical trial. Am J Respir Crit Care Med. 2010 Jan 15. 181(2):116-24. [QxMD MEDLINE Link].
- Keller D. Bronchial Thermoplasty Benefits Asthma Sufferers Long Term. Medscape Medical News. Available at https://www.medscape.com/viewarticle/804695. Accessed: June 4, 2013.
- Wechsler ME, Laviolette M, Rubin AS, Fiterman J, Lapa E Silva JR, Shah PL, et al. Bronchial thermoplasty: Long-term safety and effectiveness in patients with severe persistent asthma. J Allergy Clin Immunol. 2013 Aug 30. [QxMD MEDLINE Link].
- Boggs W. Bronchial Thermoplasty Effective for Severe Persistent Asthma. Medscape [serial online]. Available at https://www.medscape.com/viewarticle/811113. May 23, 2013; Accessed: June 26, 2024.
- O'Byrne PM, Pedersen S, Carlsson LG, et al. Risks of pneumonia in patients with asthma taking inhaled corticosteroids. Am J Respir Crit Care Med. 2011 Mar 1. 183(5):589-95. [QxMD MEDLINE Link].
- Dhuper S, Chandra A, Ahmed A, et al. Efficacy and cost comparisons of bronchodilatator administration between metered dose inhalers with disposable spacers and nebulizers for acute asthma treatment. J Emerg Med. 2011 Mar. 40(3):247-55. [QxMD MEDLINE Link].
- Rowe BH, Keller JL, Oxman AD. Effectiveness of steroid therapy in acute exacerbations of asthma: a meta-analysis. Am J Emerg Med. 1992 Jul. 10(4):301-10. [QxMD MEDLINE Link].
- Rowe BH, Edmonds ML, Spooner CH, Diner B, Camargo CA Jr. Corticosteroid therapy for acute asthma. Respir Med. 2004 Apr. 98(4):275-84. [QxMD MEDLINE Link].
- Agertoft L, Pedersen S. Effect of long-term treatment with inhaled budesonide on adult height in children with asthma. N Engl J Med. 2000 Oct 12. 343(15):1064-9. [QxMD MEDLINE Link].
- Tastepe AI, Kuzucu A, Demircan S, Liman ST, Demirag F. Surgical treatment of tracheal hamartoma. Scand Cardiovasc J. 1998. 32(4):239-41. [QxMD MEDLINE Link].
- Guilbert TW, Morgan WJ, Zeiger RS, Mauger DT, Boehmer SJ, Szefler SJ, et al. Long-term inhaled corticosteroids in preschool children at high risk for asthma. N Engl J Med. 2006 May 11. 354(19):1985-97. [QxMD MEDLINE Link].
- van den Berge M, ten Hacken NH, Cohen J, Douma WR, Postma DS. Small airway disease in asthma and COPD: clinical implications. Chest. 2011 Feb. 139(2):412-23. [QxMD MEDLINE Link].
- Kingston HG, Hirshman CA. Perioperative management of the patient with asthma. Anesth Analg. 1984 Sep. 63(9):844-55. [QxMD MEDLINE Link].
- [Guideline] Global Asthma Network. The Global Asthma Report 2022. Int J Tuberc Lung Dis. 2022 Nov 25. 26 (Supp 1):1-104. [QxMD MEDLINE Link]. [Full Text].
- Scott HA, Gibson PG, Garg ML, Pretto JJ, Morgan PJ, Callister R, et al. Dietary restriction and exercise improve airway inflammation and clinical outcomes in overweight and obese asthma: a randomized trial. Clin Exp Allergy. 2013 Jan. 43 (1):36-49. [QxMD MEDLINE Link].
- [Guideline] Nakamura Y, Tamaoki J, Nagase H, Yamaguchi M, Horiguchi T, Hozawa S, et al. Japanese guidelines for adult asthma 2020. Allergol Int. 2020 Oct. 69 (4):519-548. [QxMD MEDLINE Link].
- [Guideline] Holguin F, Cardet JC, Chung KF, et al. Management of severe asthma: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J. 2020 Jan. 55 (1):343-73. [QxMD MEDLINE Link]. [Full Text].
- Levy ML, Bacharier LB, Bateman E, Boulet LP, Brightling C, Buhl R, et al. Key recommendations for primary care from the 2022 Global Initiative for Asthma (GINA) update. NPJ Prim Care Respir Med. 2023 Feb 8. 33 (1):7. [QxMD MEDLINE Link].
- Berridge MS, Lee Z, Heald DL. Pulmonary distribution and kinetics of inhaled [11C]triamcinolone acetonide. J Nucl Med. 2000 Oct. 41(10):1603-11. [QxMD MEDLINE Link].
- Nelson HS. Advair: combination treatment with fluticasone propionate/salmeterol in the treatment of asthma. J Allergy Clin Immunol. 2001 Feb. 107(2):398-416. [QxMD MEDLINE Link].
- [Guideline] Parsons JP, Hallstrand TS, Mastronarde JG, Kaminsky DA, Rundell KW, Hull JH, et al. An official American Thoracic Society clinical practice guideline: exercise-induced bronchoconstriction. Am J Respir Crit Care Med. 2013 May 1. 187 (9):1016-27. [QxMD MEDLINE Link].
- Tantisira KG, Lasky-Su J, Harada M, et al. Genomewide association between GLCCI1 and response to glucocorticoid therapy in asthma. N Engl J Med. 2011 Sep 29. 365(13):1173-83. [QxMD MEDLINE Link].
- Peters SP, Kunselman SJ, Icitovic N, Moore WC, Pascual R, Ameredes BT, et al. Tiotropium bromide step-up therapy for adults with uncontrolled asthma. N Engl J Med. 2010 Oct 28. 363(18):1715-26. [QxMD MEDLINE Link]. [Full Text].
- Kerstjens HA, Engel M, Dahl R, Paggiaro P, Beck E, Vandewalker M, et al. Tiotropium in Asthma Poorly Controlled with Standard Combination Therapy. N Engl J Med. 2012 Sep 2. [QxMD MEDLINE Link].
- Rank MA, Liesinger JT, Ziegenfuss JY, Branda ME, Lim KG, Yawn BP, et al. The impact of asthma medication guidelines on asthma controller use and on asthma exacerbation rates comparing 1997-1998 and 2004-2005. Ann Allergy Asthma Immunol. 2012 Jan. 108(1):9-13. [QxMD MEDLINE Link].
- Brooks M. FDA Oks New Maintenance Asthma Treatment Arnuity Ellipta. Medscape Medical News. Available at https://www.medscape.com/viewarticle/830213. August 20, 2014; Accessed: June 26, 2024.
- [Guideline] Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention (2024 update). 2024. 1-261. [Full Text].
Author
Michael J Morris, MD, FACP, FCCP Clinical Faculty, Pulmonary Disease/Critical Care Service, Department of Medicine, Brooke Army Medical Center; Assistant Dean for Research, SAUSHEC, Brooke Army Medical Center; Clinical Professor, niversity of Texas Health Science Center at San Antonio, Joe R and Teresa Lozano Long School of Medicine; Professor, Uniformed Services University of the Health Sciences
Michael J Morris, MD, FACP, FCCP is a member of the following medical societies: American Association for Respiratory Care, American College of Chest Physicians, American College of Physicians, The Society of Federal Health Professionals (AMSUS)
Disclosure: Serve(d) as a speaker or a member of a speakers bureau for: Janssen Pharmaceuticals.
Coauthor(s)
Daniel J Pearson, MD, FCCP ICU Medical Director, Respiratory Therapy Medical Director, Soin Medical Center
Daniel J Pearson, MD, FCCP is a member of the following medical societies: American College of Chest Physicians, American College of Physicians, American Heart Association, American Thoracic Society, Society of Critical Care Medicine
Disclosure: Nothing to disclose.
Chief Editor
Zab Mosenifar, MD, FACP, FCCP Geri and Richard Brawerman Chair in Pulmonary and Critical Care Medicine, Professor and Executive Vice Chairman, Department of Medicine, Medical Director, Women's Guild Lung Institute, Cedars Sinai Medical Center, University of California, Los Angeles, David Geffen School of Medicine
Zab Mosenifar, MD, FACP, FCCP is a member of the following medical societies: American College of Chest Physicians, American College of Physicians, American Federation for Medical Research, American Thoracic Society
Disclosure: Nothing to disclose.
Acknowledgements
Edward Bessman, MD, MBA Chairman and Clinical Director, Department of Emergency Medicine, John Hopkins Bayview Medical Center; Assistant Professor, Department of Emergency Medicine, Johns Hopkins University School of Medicine
Edward Bessman, MD, MBA is a member of the following medical societies: American Academy of Emergency Medicine, American College of Emergency Physicians, and Society for Academic Emergency Medicine
Disclosure: Nothing to disclose.
Paul Blackburn, DO, FACOEP, FACEP Attending Physician, Department of Emergency Medicine, Maricopa Medical Center
Paul Blackburn, DO, FACOEP, FACEP is a member of the following medical societies: American College of Emergency Physicians, American College of Osteopathic Emergency Physicians, American Medical Association, and Arizona Medical Association
Disclosure: Nothing to disclose.
Barry E Brenner, MD, PhD, FACEP Professor of Emergency Medicine, Professor of Internal Medicine, Program Director for Emergency Medicine, Case Medical Center, University Hospitals, Case Western Reserve University School of Medicine
Barry E Brenner, MD, PhD, FACEP is a member of the following medical societies: Alpha Omega Alpha, American Academy of Emergency Medicine, American College of Chest Physicians, American College of Emergency Physicians, American College of Physicians, American Heart Association, American Thoracic Society, Arkansas Medical Society, New York Academy of Medicine, New York Academy of Sciences, and Society for Academic Emergency Medicine
Disclosure: Nothing to disclose.
Helen M Hollingsworth, MD Director, Adult Asthma and Allergy Services, Associate Professor, Department of Internal Medicine, Division of Pulmonary and Critical Care, Boston Medical Center
Helen M Hollingsworth, MD is a member of the following medical societies: American Academy of Allergy Asthma and Immunology, American College of Chest Physicians, American Thoracic Society, and Massachusetts Medical Society
Disclosure: Nothing to disclose.
Robert E O'Connor, MD, MPH Professor and Chair, Department of Emergency Medicine, University of Virginia Health System
Robert E O'Connor, MD, MPH is a member of the following medical societies: American Academy of Emergency Medicine, American College of Emergency Physicians, American College of Physician Executives, American Heart Association, American Medical Association, Medical Society of Delaware, National Association of EMS Physicians, Society for Academic Emergency Medicine, and Wilderness Medical Society
Disclosure: Nothing to disclose.
Francisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical Center College of Pharmacy; Editor-in-Chief, Medscape Drug Reference
Disclosure: Medscape Salary Employment