Arachnoiditis Imaging: Practice Essentials, Radiography, Computed Tomography (original) (raw)
Practice Essentials
Arachnoiditis is a broad term denoting inflammation of the meninges and subarachnoid space. It is characterized by thickening of the arachnoid membrane and dura mater adhesions that result in chronic lower back pain. Complications include cranial neuropathies, myelopathy, and radiculopathy. Arachnoiditis has many causes, including infectious, inflammatory, and neoplastic processes. Infectious causes include bacterial, viral, fungal, and parasitic agents. Noninfectious inflammatory etiologies include surgery, intrathecal hemorrhage, and the administration of intrathecal agents, such as myelographic contrast media, anesthetics, and steroids. [1, 2, 3, 4, 5, 6]
The most severe type of arachnoiditis is adhesive arachnoiditis, with scar tissue compressing the nerve roots and ultimately disrupting both blood supply and flow of cerebrospinal fluid. Adhesive arachnoiditis can progress to arachnoiditis ossificans, or ossification of the spinal arachnoid. [1, 7, 8, 9, 10, 2, 3, 4, 5, 6]
Neoplasia includes the hematogenous spread of systemic tumors, such as breast and lung carcinoma, melanoma, and non-Hodgkin lymphoma. Neoplasia also includes direct seeding of the cerebrospinal fluid (CSF) from primary central nervous system (CNS) tumors, such as glioblastoma multiforme, medulloblastoma, ependymoma, and choroid plexus carcinoma. [11]
Imaging modalities
Because of its noninvasive nature, multiplanar capabilities, and superb soft-tissue characterization, magnetic resonance imaging (MRI) is the study of choice for the diagnostic evaluation of arachnoiditis. [12, 13] For patients in whom MRI is contraindicated, computed tomography (CT) myelography is an acceptable alternative. [14, 15, 16] MRI has a reported sensitivity of 92% and specificity of 100% for chronic adhesive arachnoiditis, with the most frequent findings on MRI being loculated arachnoid cysts on several vertebral bodies or the entire spine, spinal cord swelling, cord displacement, cord atrophy, nerve root clumping, syrinx formation, and arachnoid septations. CT myelography can display myelography spread block, thickened or tethered nerve roots, soft tissue mass within the arachnoid space, and intrathecal calcification. MRI is preferred for adhesive arachnoiditis because it can differentiate between benign meningeal calcification and ossification of arachnoid tissue. For arachnoiditis ossificans, noncontrast enhanced CT has been reported to provide more sensitivity than MRI. [1, 7, 8]
In cases of arachnoiditis ossificans, MRI shows irregular thickening and clumping of nerve roots of the cauda equina, and CT can show evidence of the mineral component. Domenicucci et al classified arachnoiditis ossificans as type I (at the thoracic level as a semicircular pattern of ossification involving part of the thecal sac); type II (at either the thoracic or lumbar level as a circular pattern that involves the circumference of the thecal sac); and type III (exclusively at the lumbar level, with ossification of the entire contents of the thecal sac). [8, 9, 10]
In a retrospective study of 29 cases of advanced chronic adhesive arachnoiditis (age, 23-96 years) by Anderson et al, imaging characteristics (29 underwent MRI, and 7 also underwent CT myelography) included loculated CSF collections (n = 23); nerve root clumping, enhancement, and displacement (n = 15); cord swelling with increased T2 signal (n = 12); arachnoid septations (n = 11); cord atrophy (n = 6); syrinx (n = 5); and intrathecal calcifications (n = 3). [7]
(Neural effects of arachnoiditis are displayed in the images below.)

Postoperative anteroposterior (AP) myelogram reveals thickened, clumped nerve roots in arachnoiditis.

Sagittal T1-weighted MRI of the lumbar spine in a patient with adhesive arachnoiditis who received epidural steroid injections. Image shows thickened and clumped nerve roots, which give the appearance of a tethered spinal cord.
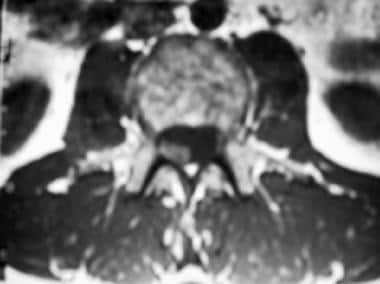
Axial T1-weighted MRI of the lumbar spine shows that the nerve roots adhere to one another and the dural sac.
A retrospective study of 28 patients with lumbar arachnoiditis found limited association between MRI findings and clinical findings, with the exception of confounding lumbar pathology (which was associated with symptom dynamics) and nerve root contour (which was associated with motor and sensory symptoms). [17]
![]()
Radiography
The spinal cord and nerve roots cannot be evaluated with routine plain radiographs. However, myelography with the intrathecal administration of iodinated contrast material is useful in evaluating the contents of the thecal sac. In adults, the conus medullaris normally terminates between the T12-L1 and L1-L2 levels. Below these levels, the nerve roots normally float freely within the thecal sac. Meningeal inflammation leads to thickened or clumped nerve roots (as in the images below), blockage of CSF flow, and the formation of CSF loculations. With radiographic findings, the degree of confidence is high.
Postoperative anteroposterior (AP) myelogram reveals thickened, clumped nerve roots in arachnoiditis.

Postoperative lateral myelographic image reveals clumped and matted nerve roots that simulate a tethered spinal cord in arachnoiditis.
![]()
Computed Tomography
MRI is far superior to conventional CT scanning in the evaluation of arachnoiditis because of the poor contrast resolution in CT scans between the spinal cord and nerve roots and CSF. However, CT myelography is effective in demonstrating the classic imaging findings of arachnoiditis. These include narrowing or blockage of the subarachnoid space, irregular collections of contrast material, thickened or matted nerve roots, and absent filling of nerve root sleeves. [16] With conventional CT scanning, the degree of confidence in findings is low. With myelography, the degree of confidence is high.
(See the image below.)

Postoperative CT myelogram obtained at the level of a laminectomy defect shows an empty sac due to adherence of the nerve roots to the thecal sac.
![]()
Magnetic Resonance Imaging
MRI is the study of choice for the diagnostic evaluation of arachnoiditis. [18, 19, 20, 21] T1-weighted MRI scans, as demonstrated in the images below, may reveal an indistinct or absent cord outline due to the increase in the signal intensity of the surrounding CSF. This may be the result of an elevation in CSF protein content, the presence of inflammatory exudate, or the formation of adhesions along the surface of the spinal cord.

T1-weighted nonenhanced sagittal MRI of the lumbar spine reveals indistinct, poorly defined nerve roots of the cauda equina in tuberculous arachnoiditis and meningitis.

T1-weighted sagittal nonenhanced MRI of the cervical spine shows abnormally increased signal intensity in the subarachnoid space, which is isointense relative to the spinal cord, in a patient with tuberculous arachnoiditis.

T1-weighted sagittal nonenhanced MRI of the lumbar spine shows signal intensity throughout the subarachnoid space that is diffusely increased, compared with that of the spinal cord (arrow), in tuberculous arachnoiditis.
T2-weighted MRI scans may demonstrate CSF loculation and obliteration of the subarachnoid space or irregularly thickened, clumped nerve roots (as shown in the first 2 images below), which occasionally may be misinterpreted as a tethered cord or a thickened filum terminale. With more severe arachnoiditis, progression of nerve root clumping and leptomeningeal adhesions may lead to angular defects in the dural sac. Peripheral adherence of the nerve roots to the walls of the thecal sac produces the so-called featureless, or empty, sac, as seen in the third image below.

Sagittal T2-weighted MRI of the lumbar spine after laminectomy for arachnoiditis shows thickened, clumped nerve roots.
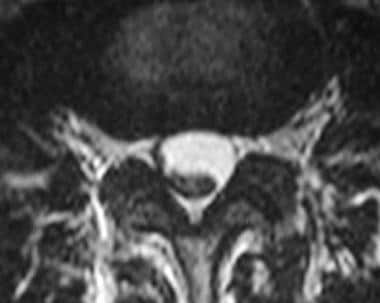
Axial T2-weighted MRI of the lumbar spine in arachnoiditis shows that the nerve roots do not float freely in the thecal sac; instead, they adhere to one another.

Axial T2-weighted MRI of the lumbar spine obtained at the level of laminectomy for arachnoiditis. Peripheral adherence of the nerve roots to the dural sac causes the empty-sac appearance.
Contrast enhancement is an inconstant finding. When it does occur, enhancement may be the result of a vascular network within the fibrous stroma that develops in the subarachnoid space. Three patterns of enhancement have been described, as follows:
- The most common pattern of enhancement (seen in the image below) is a smooth, linear layer of enhancement outlining the surface of the cord and nerve roots.

T1-weighted sagittal fat-suppressed contrast-enhanced MRI of the lumbar spine in tuberculous arachnoiditis and meningitis shows thin, linear leptomeningeal enhancement of the conus medullaris and cauda equina. - The second-most common pattern is a nodular pattern (seen in the image below) with discrete foci of enhancement seen along the surface of the cord and nerve roots.

T1-weighted sagittal MRI of the cervical spine in tuberculous arachnoiditis shows nodular pockets of enhancement in the subarachnoid space after the administration of contrast material. - The least common pattern consists of diffuse intradural enhancement that completely fills the subarachnoid space (as shown in the images below).
T1-weighted sagittal nonenhanced MRI of the lumbar spine shows signal intensity throughout the subarachnoid space that is diffusely increased, compared with that of the spinal cord (arrow), in tuberculous arachnoiditis.
T1-weighted sagittal contrast-enhanced MRI of a lumbar-spine tuberculous arachnoiditis reveals diffuse enhancement that fills the entire subarachnoid space. Tuberculosis (TB) bacilli were isolated from the CSF.
No pattern of enhancement has been found to be characteristic of any specific infectious agent or pathologic process. In general, benign arachnoiditis enhances less avidly than does carcinomatous meningitis; however, MRI findings alone cannot be used to differentiate infection from neoplasm. [22]
MRI after the administration of intrathecal gadopentate dimeglumine (Gd-DTPA) has been described as a safe, effective technique to diagnose or exclude the diagnosis of arachnoiditis. [23, 14, 15]
In one report, arachnoiditis could not be excluded on routine postoperative intravenous-enhanced MRI in a patient with progressive paraparesis and sphincter incontinence. Arachnoiditis was differentiated from postoperative changes with intrathecal-enhanced MRI. Doses ranging from 0.8 to 2 ml of gadolinium mixed with 3 to 5 ml of the patients' CSF under sterile conditions have been injected into the subarachnoid space. MRI was performed utilizing T1-weighted, fat-suppressed sequences in 2-3 orthogonal planes.
Purported advantages of gadolinium-enhanced intrathecal MR imaging include an absence of ionizing radiation, the capability of direct multiplanar imaging, an absence of bony artifact, and high spatial and contrast resolution. It should be noted that although a cooperative multicenter study of 95 patients failed to demonstrate behavioral changes, neurologic alteration, or seizure activity with intrathecal gadolinium, the administration of intrathecal gadolinium is not approved for use by the FDA and has been used off-label.
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). The disease has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or MRA scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness.
With MRI findings, the degree of confidence is high. Sarcoidosis and spinal anesthesia may cause false results.
![]()
- Peng H, Conermann T. Arachnoiditis. 2022 Jan. [QxMD MEDLINE Link]. [Full Text].
- Khan MU, Devlin JA, Fraser A. Adhesive arachnoiditis in mixed connective tissue disease: a rare neurological manifestation. BMJ Case Rep. 2016 Dec 16. 2016:[QxMD MEDLINE Link].
- Panackal AA, Komori M, Kosa P, Khan O, Hammoud DA, Rosen LB, et al. Spinal Arachnoiditis as a Complication of Cryptococcal Meningoencephalitis in Non-HIV Previously Healthy Adults. Clin Infect Dis. 2017 Feb 1. 64 (3):275-283. [QxMD MEDLINE Link].
- Kondety SK, Chatterjee S. Acquired Chiari malformation secondary to tuberculous arachnoiditis of the lumbar spine. Neurol India. 2016 Sep-Oct. 64 (5):1066-8. [QxMD MEDLINE Link].
- Chattopadhyay I, Jha AK, Banerjee SS, Basu S. Post-procedure adhesive arachnoiditis following obstetric spinal anaesthesia. Indian J Anaesth. 2016 May. 60 (5):372-4. [QxMD MEDLINE Link].
- Steel CJ, Abrames EL, O'Brien WT. Arachnoiditis Ossificans - A Rare Cause of Progressive Myelopathy. Open Neuroimag J. 2015. 9:13-20. [QxMD MEDLINE Link].
- Anderson TL, Morris JM, Wald JT, Kotsenas AL. Imaging Appearance of Advanced Chronic Adhesive Arachnoiditis: A Retrospective Review. AJR Am J Roentgenol. 2017 Sep. 209 (3):648-655. [QxMD MEDLINE Link].
- Urits I, Chesteen G, Viswanath O. Arachnoiditis Ossificans of the Lumbosacral Spine. Turk J Anaesthesiol Reanim. 2019 Oct. 47 (5):427-428. [QxMD MEDLINE Link].
- Brou C, Labaisse MA, Tchofo PJ. Arachnoiditis Ossificans. J Belg Soc Radiol. 2021 Jun 17. 105 (1):37. [QxMD MEDLINE Link].
- Domenicucci M, Ramieri A, Passacantilli E, Russo N, Trasimeni G, Delfini R. Spinal arachnoiditis ossificans: report of three cases. Neurosurgery. 2004 Oct. 55 (4):985. [QxMD MEDLINE Link].
- Maulucci CM, Ghobrial GM, Oppenlander ME, Flanders AE, Vaccaro AR, Harrop JS. Arachnoiditis ossificans: clinical series and review of the literature. Clin Neurol Neurosurg. 2014 Sep. 124:16-20. [QxMD MEDLINE Link].
- Malani AN, Vandenberg DM, Singal B, Kasotakis M, Koch S, Moudgal V, et al. Magnetic resonance imaging screening to identify spinal and paraspinal infections associated with injections of contaminated methylprednisolone acetate. JAMA. 2013 Jun 19. 309(23):2465-72. [QxMD MEDLINE Link].
- Lammering JC, Iv M, Gupta N, Pandit R, Patel MR. Imaging spectrum of CNS coccidioidomycosis: prevalence and significance of concurrent brain and spinal disease. AJR Am J Roentgenol. 2013 Jun. 200(6):1334-46. [QxMD MEDLINE Link].
- Munoz A., Hinojosa J., Esparza J. Cisternography and Ventriculography Gadopentate Dimeglumine-Enhanced MR Imaging in Pediatric Patients: Preliminary Report. AJNR. May 2007. 28:889-894.
- Tali ET, Ercan N, Krumina G, et. al. Intrathecal gadolinium (gadopentate dimeglumine) enhanced magnetic resonance myelography and cisternography: results of a multicenter study. Invest Radiol. March 2002. 37(3):152-9.
- Dong A, Zuo C, Zhang P, Lu J, Bai Y. MRI and FDG PET/CT findings in 3 cases of spinal infectious arachnoiditis. Clin Nucl Med. 2014 Oct. 39 (10):900-3. [QxMD MEDLINE Link].
- Parenti V, Huda F, Richardson PK, Brown D, Aulakh M, Taheri MR. Lumbar arachnoiditis: Does imaging associate with clinical features?. Clin Neurol Neurosurg. 2020 May. 192:105717. [QxMD MEDLINE Link].
- Georgy BA, Snow RD, Hesselink JR. MR imaging of spinal nerve roots: techniques, enhancement patterns, and imaging findings. AJR Am J Roentgenol. 1996 Jan. 166(1):173-9. [QxMD MEDLINE Link].
- Gero B, Sze G, Sharif H. MR imaging of intradural inflammatory diseases of the spine. AJNR Am J Neuroradiol. 1991 Sep-Oct. 12(5):1009-19. [QxMD MEDLINE Link].
- Gupta RK, Gupta S, Kumar S. MRI in intraspinal tuberculosis. Neuroradiology. 1994. 36(1):39-43. [QxMD MEDLINE Link].
- Sharma A, Goyal M, Mishra NK. MR imaging of tubercular spinal arachnoiditis. AJR Am J Roentgenol. 1997 Mar. 168(3):807-12. [QxMD MEDLINE Link].
- Chamberlain MC, Glantz M, Groves MD, Wilson WH. Diagnostic tools for neoplastic meningitis: detecting disease, identifying patient risk, and determining benefit of treatment. Semin Oncol. 2009 Aug. 36(4 Suppl 2):S35-45. [QxMD MEDLINE Link].
- Johnson CE, Sze G. Benign lumbar arachnoiditis: MR imaging with gadopentetate dimeglumine. AJNR Am J Neuroradiol. 1990 Jul-Aug. 11(4):763-70. [QxMD MEDLINE Link].
- Postoperative anteroposterior (AP) myelogram reveals thickened, clumped nerve roots in arachnoiditis.
- Postoperative lateral myelographic image reveals clumped and matted nerve roots that simulate a tethered spinal cord in arachnoiditis.
- Postoperative CT myelogram obtained at the level of a laminectomy defect shows an empty sac due to adherence of the nerve roots to the thecal sac.
- Sagittal T1-weighted MRI of the lumbar spine in a patient with adhesive arachnoiditis who received epidural steroid injections. Image shows thickened and clumped nerve roots, which give the appearance of a tethered spinal cord.
- Axial T1-weighted MRI of the lumbar spine shows that the nerve roots adhere to one another and the dural sac.
- Sagittal T2-weighted MRI of the lumbar spine after laminectomy for arachnoiditis shows thickened, clumped nerve roots.
- Axial T2-weighted MRI of the lumbar spine in arachnoiditis shows that the nerve roots do not float freely in the thecal sac; instead, they adhere to one another.
- Axial T2-weighted MRI of the lumbar spine obtained at the level of laminectomy for arachnoiditis. Peripheral adherence of the nerve roots to the dural sac causes the empty-sac appearance.
- T1-weighted nonenhanced sagittal MRI of the lumbar spine reveals indistinct, poorly defined nerve roots of the cauda equina in tuberculous arachnoiditis and meningitis.
- T1-weighted sagittal fat-suppressed contrast-enhanced MRI of the lumbar spine in tuberculous arachnoiditis and meningitis shows thin, linear leptomeningeal enhancement of the conus medullaris and cauda equina.
- Contrast-enhanced T1-weighted axial MRI of the brain shows thick nodular enhancement of the basal cisterns.
- T1-weighted sagittal nonenhanced MRI of the cervical spine shows abnormally increased signal intensity in the subarachnoid space, which is isointense relative to the spinal cord, in a patient with tuberculous arachnoiditis.
- T1-weighted sagittal MRI of the cervical spine in tuberculous arachnoiditis shows nodular pockets of enhancement in the subarachnoid space after the administration of contrast material.
- T1-weighted sagittal nonenhanced MRI of the lumbar spine shows signal intensity throughout the subarachnoid space that is diffusely increased, compared with that of the spinal cord (arrow), in tuberculous arachnoiditis.
- T1-weighted sagittal contrast-enhanced MRI of a lumbar-spine tuberculous arachnoiditis reveals diffuse enhancement that fills the entire subarachnoid space. Tuberculosis (TB) bacilli were isolated from the CSF.
- Sagittal T1-weighted precontrast and postcontrast MRIs. The postcontrast image reveals diffuse leptomeningeal enhancement along the surface of the brainstem and cervical cord.

Author
Specialty Editor Board
Bernard D Coombs, MB, ChB, PhD Consulting Staff, Department of Specialist Rehabilitation Services, Hutt Valley District Health Board, New Zealand
Disclosure: Nothing to disclose.
Chief Editor
Additional Contributors
Lucien M Levy, MD, PhD
Lucien M Levy, MD, PhD is a member of the following medical societies: American Cancer Society, American College of Radiology, American Heart Association, American Medical Association, American Roentgen Ray Society, American Society of Neuroradiology, Radiological Society of North America
Disclosure: Nothing to disclose.