Clinical value of serum CA19-9 levels in evaluating resectability of pancreatic carcinoma (original) (raw)
Abstract
AIM: To evaluate the clinical value of serum CA19-9 levels in predicting the respectability of pancreatic carcinoma according to receiver operating characteristic (ROC) curve analysis.
METHODS: Serum CA19-9 levels were measured in 104 patients with pancreatic cancer which were possible to be resected according to the imaging. ROC curve was plotted for the CA19-9 levels. The point closest to the upper left-hand corner of the graph were chosen as the cut-off point. The sensitivity, specificity, positive and negative predictive values of CA19-9 at this cut-off point were calculated.
RESULTS: Resectable pancreatic cancer was detected in 58 (55.77%) patients and unresectable pancreatic cancer was detected in 46 (44.23%) patients. The area under the ROC curve was 0.918 and 95% CI was 0.843-0.992. The CA19-9 level was 353.15 U/mL, and the sensitivity and specificity of CA19-9 at this cut-off point were 93.1% and 78.3%, respectively. The positive and negative predictive value was 84.38% and 90%, respectively.
CONCLUSION: Preoperative serum CA19-9 level is a useful marker for further evaluating the resectability of pancreatic cancer. Obviously increased serum levels of CA19-9 (> 353.15 U/mL) can be regarded as an ancillary parameter for unresectable pancreatic cancer.
Keywords: Pancreatic carcinoma, Resection, Tumor markers, CA19-9, Receiver operating characteristic curve
INTRODUCTION
The prognosis of pancreatic cancer is extremely poor and its early diagnosis is difficult[1,2]. Surgical resection offers the best chance of cure. However, local vascular involvement, nodal and distant metastases are frequently found at the time of diagnosis, thus losing the opportunity of operation[3]. At present, the best way for preoperative staging of pancreatic cancer is bolus-contrast, and triple-phase helical computed tomography, which has been shown to be almost 100% accurate in predicting unresectable disease[4–6]. However, approximately 25%-50% of patients with resectable disease on computed tomography are found to have unresectable lesions at laparotomy[7].
CA19-9 is the most widely used pancreatic cancer serum marker. Serum CA19-9 level has been shown to correlate with the thyroid node metastasis (TNM) staging, and tumor size in patients with pancreatic cancer[8]. However, little is known about the value of serum CA19-9 level in evaluating the resectability of pancreatic carcinoma.
Receiver operating characteristic (ROC) curve has been widely accepted as the standard method for dscribing and comparing the accuracy of medical diagnostic tests[9,10]. ROC curve is an efficient way to display and assess the predictive value of cut-off points.
In this study, we evaluated the clinical value of serum CA19-9 level in predicting the resectability of pancreatic carcinoma according to ROC curve analysis.
MATERIALS AND METHODS
We retrospectively reviewed the clinical and imaging data including preoperative CA19-9 level in 104 patients with pancreatic cancer who underwent surgical resection at the Affiliated Hospital of Qingdao University Medical College from January 2001 to July 2007. Pancreatic adenocarcinoma was histologically confirmed. Resectability of pancreatic cancer was evaluated at least by preoperative bolus-contrast, triple-phase helical computer tomography (CT) scan.
Resectability was defined as a tumour limited to the pancreas with no invasion of the superior mesenteric artery and vein, portal vein and metastases (celiac lymph, peritoneum or liver).
Serum levels of CA19-9 and total serum bilirubin levels were measured before surgery (normal 0-39.0 U/mL for CA19-9, 3.4-17.1 μmol/L for total serum bilirubin).
The data were described using Q1-3. Differences between groups were detected using the Wilcoxon 2-sample test. Serum CA19-9 levels were used to plot the ROC curve, and calculate the area under the curve (AUC). We chose the point closest to the upper left-hand corner of the graph as the cut-off point. The sensitivity, specificity, positive and negative predictive values of CA19-9 at this cut-off point were calculated. P < 0.05 was considered statistically significant.
RESULTS
Of the 104 patients, 72 were males and 32 were females with a mean age of 59 years (range 41-75 years). The pancreatic tumor was confined to the head, body and tail of the pancreas in 86, 8, and 10 patients, respectively. Forty-eight patients underwent pancreatic- coduodenectomy, 10 patients distal pancreatectomy, and 46 only exploratory laparotomy and biopsy. The general characteristics of the patients are listed in Table 1.
Table 1.
Characteristics of patients (n = 104)
| Characteristics | Data, n (%) |
|---|---|
| Age (yr) | 59 ± 9 (mean ± SD) |
| Sex | |
| Male | 72 (69.2) |
| Female | 32 (30.8) |
| Location of tumors | |
| Head | 86 (82.7) |
| Body | 8 (7.7) |
| Body and tail | 10 (9.6) |
| Type of operation | |
| Pancreaticoduodenectomy | 48 (46.2) |
| Distal pancreatectomy | 10 (9.6) |
| Exploratory laparotomy and biopsy | 46 (44.2) |
The distribution of preoperative serum CA19-9 levels is shown in Figure 1. The Q2 (median) preoperative serum CA19-9 level in patients with unresectable tumor was 5-fold higher than that in patients with resectable tumor (Table 2). The difference between two groups was significant (P < 0.01). The mean total serum bilirubin level in patients with resectable and unresectable tumor was 28.6 μmol/L and 34.4 μmol/L, respectively (_P_ > 0.05). Therefore, the CA19-9 levels were not adjusted.
Figure 1.
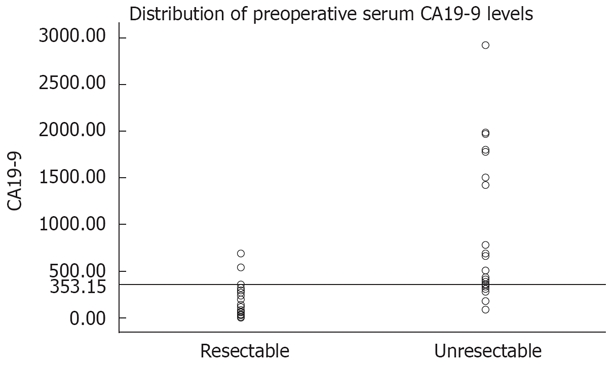
Distribution of preoperative serum CA19-9 levels. The horizon marker is set according to the cut-off point of CA19-9 (353.15 U/mL).
Table 2.
CA19-9 levels in patients with resectable and unresectable pancreatic cancer
| Group | n | CA19-9 (U/mL) | Wilcoxon | |||
|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Z | P | ||
| Resectable | 58 | 15.57 | 130.10 | 270.25 | -5.132 | 0.000 |
| Unresectable | 46 | 361.30 | 656.20 | 1780.00 |
Figure 2 shows the ROC curve. The AUC was 0.918 and 95% CI was 0.843-0.992, suggesting that changes in serum CA19-9 levels may have a direct relation to resectability[11,12]. When the cut-off value of CA19-9 was 353.15 U/mL according to the point closest to the upper left-hand corner of the graph, the sensitivity and specificity were 93.1% and 78.3%, respectively. The preoperative resectability according to the cut-off point was compared with the actual operation, and the positive and negative predictive value of CA19-9 was 84.38% and 90.00%, respectively (Table 3).
Figure 2.
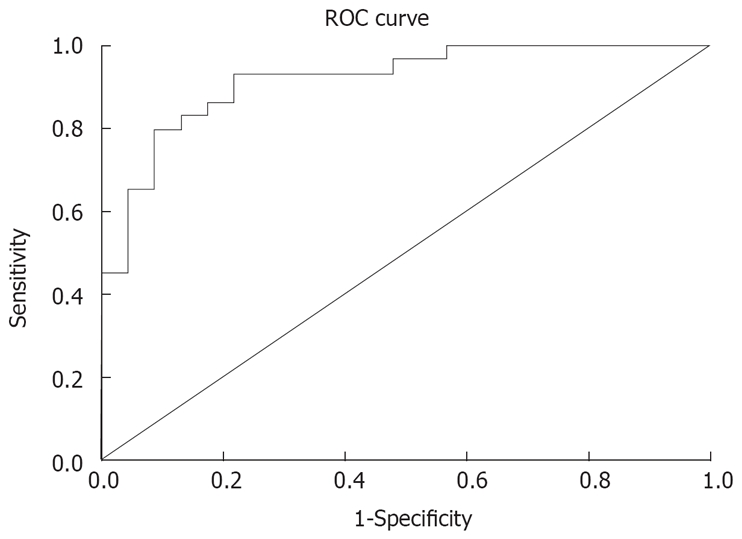
ROC analysis of CA19-9. Perfect discrimination has a ROC plot passing through the upper left corner (100% sensitivity, 100% specificity). The closer the ROC plot to the upper left corner, the higher the overall accuracy of the test (AUC: 0.9-1 indicating excellent; 0.8-0.9 indicating very good; 0.7-0.8 indicating good; 0.6-0.7 indicating average; 0.5-0.6 indicating poor). The AUC of CA19-9 was 0.918.
Table 3.
Positive and negative predictive values of CA19-9 at the cut-off point
| Resection | Total | Predictive value | |||
|---|---|---|---|---|---|
| Yes | No | ||||
| CA19-9 (U/mL) | ≤ 353.15 | 54 | 10 | 64 | 84.38% (+) |
| > 353.15 | 4 | 36 | 40 | 90.00% (-) | |
| Total | 58 | 46 | 104 |
DISCUSSION
Pancreatic cancer is one of the most common causes for cancer-related death. The overall five-year survival rate ranges from 0.4% to 4%, the lowest for any cancer[1,13]. Early diagnosis of pancreatic cancer is difficult because its early symptoms are usually non-specific. Local vascular involvement, nodal and distant metastases are frequently found at the time of diagnosis[14].
Recently, considerable improvements in radiological imaging make it possible to limit surgery for patients who will benefit[15,16]. The current methods of choice for diagnosing and staging pancreatic cancer are thin section, contrast-enhanced, and triple-phase helical computed tomography[17,18]. However, approximately 25%-50% of patients with resectable disease on computed tomography are found to have unresectable lesions at laparotomy[7,19]. Although magnetic resonance imaging is increasingly used in the evaluation of pancreatic tumor, it was reported that it offers no significant diagnostic advantage over computed tomography[20]. Endoscopic retrograde cholangio pancreatography (ERCP) is more controversial for patients with a mass on CT[21]. B-mode ultrasonography is operator-dependent and may be inaccurate due to factors such as large body habitus, presence of ascites, or overlying bowel gas. Therefore we should find other ways to further evaluate the resectability of pancreatic cancer.
CA19-9 is a tumor-associated antigen, initially described by Koprowski et al[22]. The sensitivity and specificity of CA19-9 for the diagnosis of pancreatic cancer are higher than than those of CEA, CA50 and CA242[23–25]. CA19-9 has become a predominant tumor marker for the diagnosis of pancreatic adenocarcinoma. It was reported that CA19-9 level is useful in diagnosis and prognosis of pancreatic cancer[26,27]. However, little is known about the value of serum CA19-9 levels in evaluating the resectability of pancreatic carcinoma[28]. This study was to find whether preoperative serum CA19-9 is a useful marker for evaluating the resectability of pancreatic cancer.
In the present study, the differences between patients with resectable and unresectable pancreatic cancer were significant (P < 0.01). The AUC was 0.918 and 95% CI was 0.843-0.992, suggesting that the preoperative serum CA19-9 level is an efficient marker for evaluating the resectability of pancreatic carcinoma. When the cut-off value of CA19-9 was 353.15 U/mL according to the point closest to the upper left-hand corner of the graph, the sensitivity, specificity, positive and negative predictive value was 93.1%, 78.3%, 84.38% and 90%, respectively, indicating that increased serum levels of CA19-9 (> 353.15 U/mL) can be regarded as an ancillary parameter for the unresectable pancreatic cancer[29]. Pancreatic cancer was resectable only in 4 patients whose preoperative serum CA19-9 level was over 353.15 U/mL (Table 3 and Figure 1).
Kilic et al[30] reported that the sensitivity, specificity, positive and negative predictive value are 82.4%, 92.3%, 91.4% and 83.9%, respectively, in 51 patients, and the cut-off value of CA19-9 is 256.4 U/mL. Their results are similar to our data, but the cut-off value was lower than that in our study (256.4 U/mL vs 353.15 U/mL). The discrepancy may be due the sample size, and the unadjusted CA19-9 level according to the bilirubin level.
In conclusion, a preoperative serum CA19-9 level is a useful marker for evaluating the resectability of pancreatic cancer. Increased serum levels of CA19-9 (> 353.15 U/mL) can be regarded as an ancillary parameter for unresectable pancreatic cancer.
COMMENTS
Background
At present, the best way of preoperative staging of pancreatic cancer is bolus-contrast and triple-phase helical computed tomography. However, approximately 25%-50% of patients with resectable disease on computed tomography are found to have unresectable lesions at laparotomy.
Research frontiers
CA19-9 is the most widely used serum marker of pancreatic cancer. CA19-9 has been shown to correlate with the thyroid node metastasis (TNM) staging and tumor size in patients with pancreatic cancer. However, little is known about the value of serum CA19-9 levels in evaluating the resectability of pancreatic carcinoma.
Innovations and breakthroughs
Receiver operating characteristic (ROC) curve analysis was used to evaluate the clinical value of serum CA19-9 levels in predicting the resectability of pancreatic carcinoma.
Applications
Preoperative serum CA19-9 level may be a useful marker for evaluating the resectability of pancreatic cancer. Increased serum level of CA19-9 (> 353.15 U/mL) may be regarded as an ancillary parameter for unresectable pancreatic cancer.
Terminology
CA19-9 is a tumor-associated antigen initially described by Koprowski et al and has been widely used as a serum marker of pancreatic cancer. ROC curve has been widely accepted as the standard method for describing and comparing the accuracy of medical diagnostic tests. ROC curve is an efficient way to display and assess the predictive value of cut-off points.
Peer review
This is a very interesting study. The authors used ROC analysis as an appropriate statistical method for defining the cut-off value of serum CA19-9 to discriminate between resectable and unresectable pancreatic cancer.
Peer reviewers: Dr. Bernd Sido, Department of General and Abdominal Surgery, Teaching Hospital of the University of Regensburg, Hospital Barmherzige Brüder, Prüfeninger Strasse 86, Regensburg D-93049, Germany; Giuseppe Tisone, Professor, Department of Surgery, University of Rome Tor Vergata, Ospedale S.Eugenio, Piazzale dell’Umanesimo 10, Rome 00144, Italy
S- Editor Li DL L- Editor Wang XL E- Editor Liu Y
References
- 1.Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, Thun MJ. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71–96. doi: 10.3322/CA.2007.0010. [DOI] [PubMed] [Google Scholar]
- 2.Wang L, Yang GH, Lu XH, Huang ZJ, Li H. Pancreatic cancer mortality in China (1991-2000) World J Gastroenterol. 2003;9:1819–1823. doi: 10.3748/wjg.v9.i8.1819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Warshaw AL, Fernandez-del Castillo C. Pancreatic carcinoma. N Engl J Med. 1992;326:455–465. doi: 10.1056/NEJM199202133260706. [DOI] [PubMed] [Google Scholar]
- 4.Tamm EP, Silverman PM, Charnsangavej C, Evans DB. Diagnosis, staging, and surveillance of pancreatic cancer. AJR Am J Roentgenol. 2003;180:1311–1323. doi: 10.2214/ajr.180.5.1801311. [DOI] [PubMed] [Google Scholar]
- 5.Vargas R, Nino-Murcia M, Trueblood W, Jeffrey RB Jr. MDCT in Pancreatic adenocarcinoma: prediction of vascular invasion and resectability using a multiphasic technique with curved planar reformations. AJR Am J Roentgenol. 2004;182:419–425. doi: 10.2214/ajr.182.2.1820419. [DOI] [PubMed] [Google Scholar]
- 6.Wakabayashi H, Nishiyama Y, Otani T, Sano T, Yachida S, Okano K, Izuishi K, Suzuki Y. Role of 18F-fluorodeoxyglucose positron emission tomography imaging in surgery for pancreatic cancer. World J Gastroenterol. 2008;14:64–69. doi: 10.3748/wjg.14.64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Pisters PW, Lee JE, Vauthey JN, Charnsangavej C, Evans DB. Laparoscopy in the staging of pancreatic cancer. Br J Surg. 2001;88:325–337. doi: 10.1046/j.1365-2168.2001.01695.x. [DOI] [PubMed] [Google Scholar]
- 8.Koopmann J, Rosenzweig CN, Zhang Z, Canto MI, Brown DA, Hunter M, Yeo C, Chan DW, Breit SN, Goggins M. Serum markers in patients with resectable pancreatic adenocarcinoma: macrophage inhibitory cytokine 1 versus CA19-9. Clin Cancer Res. 2006;12:442–446. doi: 10.1158/1078-0432.CCR-05-0564. [DOI] [PubMed] [Google Scholar]
- 9.Zou KH, O'Malley AJ, Mauri L. Receiver-operating characteristic analysis for evaluating diagnostic tests and predictive models. Circulation. 2007;115:654–657. doi: 10.1161/CIRCULATIONAHA.105.594929. [DOI] [PubMed] [Google Scholar]
- 10.Walter SD, Sinuff T. Studies reporting ROC curves of diagnostic and prediction data can be incorporated into meta-analyses using corresponding odds ratios. J Clin Epidemiol. 2007;60:530–534. doi: 10.1016/j.jclinepi.2006.09.002. [DOI] [PubMed] [Google Scholar]
- 11.Altman DG, Bland JM. Diagnostic tests 2: Predictive values. BMJ. 1994;309:102. doi: 10.1136/bmj.309.6947.102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Altman DG, Bland JM. Diagnostic tests 3: receiver operating characteristic plots. BMJ. 1994;309:188. doi: 10.1136/bmj.309.6948.188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Jemal A, Murray T, Samuels A, Ghafoor A, Ward E, Thun MJ. Cancer statistics, 2003. CA Cancer J Clin. 2003;53:5–26. doi: 10.3322/canjclin.53.1.5. [DOI] [PubMed] [Google Scholar]
- 14.Pappas S, Federle MP, Lokshin AE, Zeh HJ 3rd. Early detection and staging of adenocarcinoma of the pancreas. Gastroenterol Clin North Am. 2007;36:413–429, x. doi: 10.1016/j.gtc.2007.03.013. [DOI] [PubMed] [Google Scholar]
- 15.Takhar AS, Palaniappan P, Dhingsa R, Lobo DN. Recent developments in diagnosis of pancreatic cancer. BMJ. 2004;329:668–673. doi: 10.1136/bmj.329.7467.668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Misek DE, Patwa TH, Lubman DM, Simeone DM. Early detection and biomarkers in pancreatic cancer. J Natl Compr Canc Netw. 2007;5:1034–1041. doi: 10.6004/jnccn.2007.0086. [DOI] [PubMed] [Google Scholar]
- 17.Delbeke D, Pinson CW. Pancreatic tumors: role of imaging in the diagnosis, staging, and treatment. J Hepatobiliary Pancreat Surg. 2004;11:4–10. doi: 10.1007/s00534-002-0775-x. [DOI] [PubMed] [Google Scholar]
- 18.Sahani DV, Shah ZK, Catalano OA, Boland GW, Brugge WR. Radiology of pancreatic adenocarcinoma: current status of imaging. J Gastroenterol Hepatol. 2008;23:23–33. doi: 10.1111/j.1440-1746.2007.05117.x. [DOI] [PubMed] [Google Scholar]
- 19.Karmazanovsky G, Fedorov V, Kubyshkin V, Kotchatkov A. Pancreatic head cancer: accuracy of CT in determination of resectability. Abdom Imaging. 2005;30:488–500. doi: 10.1007/s00261-004-0279-z. [DOI] [PubMed] [Google Scholar]
- 20.Hanbidge AE. Cancer of the pancreas: the best image for early detection--CT, MRI, PET or US? Can J Gastroenterol. 2002;16:101–105. doi: 10.1155/2002/184370. [DOI] [PubMed] [Google Scholar]
- 21.Andersson R, Vagianos C, Williamson R. Preoperative staging and evaluation of resectability in pancreatic ductal adenocarcinoma. HPB (Oxford) 2004;6:5–12. doi: 10.1080/13651820310017093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Koprowski H, Steplewski Z, Mitchell K, Herlyn M, Herlyn D, Fuhrer P. Colorectal carcinoma antigens detected by hybridoma antibodies. Somatic Cell Genet. 1979;5:957–971. doi: 10.1007/BF01542654. [DOI] [PubMed] [Google Scholar]
- 23.Wu X, Lu XH, Xu T, Qian JM, Zhao P, Guo XZ, Yang XO, Jiang WJ. [The diagnostic value of serum carcinoma markers, fecal K-ras and p53 gene mutation in pancreatic cancers] Zhonghua Neike Zazhi. 2005;44:741–744. [PubMed] [Google Scholar]
- 24.Okusaka T, Okada S, Sato T, Wakasugi H, Saisho H, Furuse J, Ishikawa O, Matsuno S, Yokoyama S. Tumor markers in evaluating the response to radiotherapy in unresectable pancreatic cancer. Hepatogastroenterology. 1998;45:867–872. [PubMed] [Google Scholar]
- 25.Liao Q, Zhao YP, Yang YC, Li LJ, Long X, Han SM. Combined detection of serum tumor markers for differential diagnosis of solid lesions located at the pancreatic head. Hepatobiliary Pancreat Dis Int. 2007;6:641–645. [PubMed] [Google Scholar]
- 26.Kang CM, Kim JY, Choi GH, Kim KS, Choi JS, Lee WJ, Kim BR. The use of adjusted preoperative CA 19-9 to predict the recurrence of resectable pancreatic cancer. J Surg Res. 2007;140:31–35. doi: 10.1016/j.jss.2006.10.007. [DOI] [PubMed] [Google Scholar]
- 27.Zhao JZ, Wu BH. Clinical significance of CA19-9 in diagnosis of digestive tract tumors. China Nati J New Gastroenterol. 1997;3:253–254. doi: 10.3748/wjg.v3.i4.253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Schlieman MG, Ho HS, Bold RJ. Utility of tumor markers in determining resectability of pancreatic cancer. Arch Surg. 2003;138:951–955; discussion 955-956. doi: 10.1001/archsurg.138.9.951. [DOI] [PubMed] [Google Scholar]
- 29.Zakowski L, Seibert C, VanEyck S. Evidence-based medicine: answering questions of diagnosis. Clin Med Res. 2004;2:63–69. doi: 10.3121/cmr.2.1.63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Kilic M, Gocmen E, Tez M, Ertan T, Keskek M, Koc M. Value of preoperative serum CA 19-9 levels in predicting resectability for pancreatic cancer. Can J Surg. 2006;49:241–244. [PMC free article] [PubMed] [Google Scholar]