Failure to Acquire New Semantic Knowledge in Patients With Large Medial Temporal Lobe Lesions (original) (raw)
. Author manuscript; available in PMC: 2009 Nov 3.
Published in final edited form as: Hippocampus. 2005;15(2):273–280. doi: 10.1002/hipo.20057
Abstract
We examined new semantic learning in two profoundly amnesic patients (E.P. and G.P.) whose lesions involve virtually the entire medial temporal lobe (MTL) bilaterally. The patients were given five tests of semantic knowledge for information that could only have been acquired after the onset of their amnesia in 1992 and 1987, respectively. Age-matched and education-matched controls (n = 8) were also tested. On tests of recall, E.P. and G.P. each scored 10% correct on a test of 20 easy factual questions (controls = 90%), 2% and 4% correct on 55 questions about news events (controls = 85%), and 0% and 4% correct on a test of 24 famous faces. On three tests of recognition memory for this same material, the patients scored at chance levels. Similarly, the patients were unable to judge whether persons who had been famous for many decades were still living or had died during the past 10 years (E.P. = 53%; G.P. = 50%; controls = 73%; chance = 50%). Lastly, neither patient E.P. nor patient G.P. could draw an accurate floor plan of his current residence, despite having lived there for 10 years and 1 year, respectively. The results demonstrate that the capacity for new semantic learning can be absent, or nearly absent, when there is virtually complete damage to the MTL bilaterally. Accordingly, the results raise the possibility that the acquisition of conscious (declarative) knowledge about the world cannot be supported by structures outside the MTL, even with extended exposure.
Keywords: memory, semantic learning, amnesia
INTRODUCTION
Semantic memory refers to the capacity for acquiring and recollecting facts and other general knowledge about the world (Eichenbaum and Cohen, 2001; Squire, 1992; Tulving, 1983). It has often been observed that the ability to acquire new semantic knowledge is impaired following damage to the medial temporal lobe (MTL), which includes the hippocampal region (CA fields, dentate gyrus, and the subicular complex), as well as the adjacent entorhinal, perirhinal, and parahippocampal cortices. Patients with damage limited to the hippocampus have moderate difficulty in acquiring semantic knowledge (Reed and Squire, 1998; Manns et al., 2003; Verfaeillie et al., 2000); patients with damage extending beyond the hippocampus have more severe impairment (Kitchener et al., 1998; Verfaeillie et al., 2000; Westmacott and Moscovitch, 2001). The new semantic knowledge acquired by amnesic patients typically has the characteristics of declarative memory. That is, it is flexible, consciously accessible, and it is integrated into a broad fund of stored knowledge (Shimamura and Squire, 1988; Tulving et al., 1991; Hamann and Squire, 1995; Westmacott and Moscovitch, 2001).
It has been unclear as to which brain structures are responsible for the residual ability of amnesic patients to acquire conscious semantic knowledge. One possibility is that new semantic knowledge is entirely dependent on the MTL and that sufficiently large lesions of the MTL would disable new semantic learning quite completely. An alternative possibility is that semantic learning can be successful even following extensive (or complete) damage to the MTL. For example, it has been suggested that semantic memory might be acquired gradually as conscious declarative knowledge directly in the neocortex (Tulving, 1991; Kitchener et al., 1998; McClelland et al., 1995; Holdstock et al., 2002).
It is of interest that the well-known patient H.M. has acquired significant semantic knowledge about people who became famous after he became amnesic (O’Kane et al., 2004). H.M. underwent an MTL resection in 1953, which included the entorhinal cortex, amygdala, and anterior hippocampus but spared the parahippocampal cortex and ventrocaudal perirhinal cortex (Corkin et al., 1997). Because H.M.’s hippocampus is thought to be nonfunctional (the entorhinal cortex was entirely removed), his success at learning new facts demonstrates that such learning can be supported by structures other than the hippocampus. The question remains, however, whether H.M.’s capacity for new semantic learning depends on intact MTL structures (parahippocampal cortex and dorsal perirhinal cortex) or on structures outside the MTL. We have addressed this question by examining new semantic learning in two severely amnesic patients (E.P. and G.P.) who have nearly complete MTL lesions bilaterally (and more complete MTL lesions than H.M.). It follows that if the capacity for new semantic learning is dependent on intact MTL tissue, patients E.P. and G.P. should not have been able to acquire new factual information since they became amnesic. Alternatively, if new semantic learning is supported by neocortical structures outside the MTL, patients E.P. and G.P. should have been able to acquire a substantial amount of postmorbid semantic knowledge.
METHODS
Participants
We studied two male patients (Fig. 1), who developed severe amnesia after herpes simplex encephalitis. Despite their profound memory impairment, both patients scored in the normal range on tests of general intelligence and also performed normally on seven different tests of visual perceptual discrimination, including a test of the ability to discriminate among faces (Stark and Squire, 2000). E.P. was born in 1922, had 12 years of education, and developed amnesia in 1992. G.P. was born in 1946, had 16 years of education, and developed amnesia in 1987. Estimates of MTL damage were based on quantitative analysis of magnetic resonance images from the patients and four controls for each patient (see Gold and Squire, 2004), following published procedures for segmenting the MTL (Insausti et al., 1998; Amaral and Insausti, 1990). Volume estimates for lateral temporal structures and for the frontal, parietal, and occipital lobes were based on the same controls as were used for the MTL measurements. The measurements presented here are based on improved techniques and on more controls than were available previously. Accordingly, the estimates of damage are largely similar, but not identical, to what has been reported previously for these patients (Stefanacci et al., 2000; Bayley et al., 2003; Schmolck et al., 2002; Levy et al., 2004).
FIGURE 1.
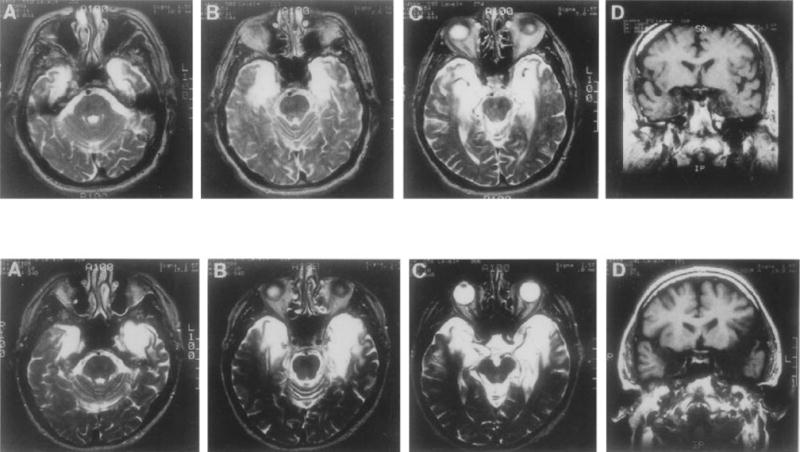
Magnetic resonance images showing the extent of temporal lobe damage in patients E.P. (top row) and G.P. (bottom row). A–C in each row are T2-weighted axial images through the temporal lobe. The images are continuous 5-mm sections (with 2.5-mm gaps) and are arranged from ventral (A) to dorsal (C). Damaged tissue is indicated by bright signal. D in each row is a coronal T1-weighted image at the level of the amygdala. Damaged tissue is indicated by dark signal. See text for description of the lesions.
E.P.’s lesion extends 7 cm caudally from the temporal lobe bilaterally and includes all of the amygdala and all of the hippocampal region (dentate gyrus, cell fields of the hippocampus proper, and subicular complex, except for a small tag of abnormally appearing vestigial tissue that comprises approximately 3% of hippocampal volume). In addition, the damage includes all of the entorhinal cortex, all of the perirhinal cortex, and much of the parahippocampal cortex (about 70% on the left and 76% on the right). The lesion also extends laterally to include the rostral portion of the fusiform gyrus (about 46% on the left and 71% on the right). The volumes for parahippocampal cortex and fusiform gyrus are more than two standard deviations below the control values. The insula is also reduced in size (about 38% on the left and 36% on the right). Lastly, the lateral temporal lobe (inferior, middle, and superior temporal gyri) is of normal size bilaterally (within 7% of the mean control volume), as are the frontal, parietal, and occipital lobes (all ± 9% of the mean control volumes).
Like E.P., G.P.’s lesion is primarily medial temporal, but his lesion extends farther laterally. The damage extends through the anterior 7 cm of the left temporal lobe and the anterior 6 cm of the right temporal lobe. The damage includes bilaterally all of the amygdala, all of the hippocampal region (except for 7% on the right), all of the entorhinal and perirhinal cortices, and much of the parahippocampal cortex (about 87% on the left and 55% on the right). The damage also includes the anterior 1cm of the temporal lobe and extends into the fusiform gyrus (about 29% on the left and 48% on the right). The insula is also reduced in volume by about 76% on the left and 39% on the right. The volumes for parahippocampal cortex, fusiform gyrus, and insula are >2 standard deviations (SD) below the control mean. Lastly, the lateral temporal lobe (inferior, middle, and superior temporal gyri) is within 13% of the mean control volume. The volumes of the frontal, parietal, and occipital cortices are all within ± 10% of the mean control volumes.
A group of eight healthy participants (2 female) served as a control group for the “easy” current events test (mean age = 79 years, mean education = 14.8 years). A second group of eight healthy participants served as a control group for the current events test, the famous faces test and the living-nonliving test (5 female, mean age = 65 years, mean education = 14.0 years). One individual served in both control groups.
Materials and Procedures
Five tests were used to assess the amount of new semantic knowledge that the patients had acquired since the onset of their amnesia. Three of the tests were given in both a free-recall version and a recognition version. On the occasions when a correct answer was given, on either a recall test or a recognition test, we also asked the patients in a later testing session to elaborate on their correct answers. If the information they provided were part of an integrated fund of knowledge, which is a hallmark of semantic memory (Tulving and Markowitsch, 1998), we expected them to be able to provide additional information. Alternatively, if the correct answers were achieved by guessing, additional information should be unavailable.
1. Twenty easy facts (recall and recognition)
Participants were asked 20 questions about information that could only have been acquired after 1988. Questions were constructed to be so easy that controls would achieve near-perfect performance. Some of the questions related to specific events (e.g., “What crime was O.J. Simpson charged with?,” “What building was destroyed on September 11, 2001?”). Other questions related to broader semantic knowledge (e.g., “What is the Internet?” and “What is the new European currency called?”). Testing occurred first in a free-recall format and then in a three-alternative, multiple-choice format. For each correct answer, patients were later asked follow-up questions to assess their knowledge of the subject more completely.
2. News events (recall and recognition)
This test was adapted from the test of news events developed by Manns et al. (2003). Participants were told that they would be asked about events that had occurred relatively recently, within the last 15 years. They were then asked 55 questions about notable news events that had occurred from 1990 to 2000 (e.g., “What is the name of the Russian leader who succeeded Boris Yeltsin?” and “Which tire manufacturer recalled thousands of tires?”). Testing was given first in a free-recall format and then in a four-alternative, multiple-choice format. For each correct answer, patients were later asked follow-up questions, as in test 1.
3. Famous faces (recall and recognition)
This test was adapted from an earlier famous faces test (Reed and Squire, 1998). The test consisted of 24 photographs of famous people who came into the news in the 1990s. The test was given first in a free-recall format (“Who is this famous person?” e.g., Tiger Woods, Bob Dole). After the recall test, participants were shown each photograph that they could not identify and asked (orally by the tester) either a yes-no question (e.g., “Is this person’s name Tiger Woods?” The name that was presented was correct half the time) or a three-alternative, multiple-choice question (e.g., “Which of the following is the correct name?” Bob Dole, Newt Gingrich, Ross Perot). Follow-up questions were asked later in the case of correct answers, as in the other tests.
4. Living or nonliving famous person
For this test (see Manns et al., 2003), participants were read aloud the names of famous (n = 126) and fictitious (n = 126) persons, one at a time (e.g., Rosemary Clooney, Frank Dixon, Doris Day). All the famous people had become famous by 1970, and about one-half (56%) of these individuals had died between 1990 and 2001. Participants first decided whether each name was or was not the name of a famous person. Then, for each person correctly judged to be famous, participants decided whether the person was still living or was deceased. To eliminate the use of age as a cue, the average age of the famous people who were living was the same as the age that the deceased people would have reached had they been still living.
5. Home floor plan
Both patients had moved into their current residences (relatively simple, single-floor dwellings) after the onset of their amnesia (E.P. in 1993, G.P. in March, 2003). In early 2004, while away from their homes, the patients were asked to draw a floor plan of their home from memory.
RESULTS
1. Twenty easy facts (recall and recognition)
Controls scored nearly perfectly on the twenty easy facts test (mean = 90 ± 3% correct, range = 75–100%; Fig. 2A). Each patient answered only two questions correctly. Specifically, both patients stated correctly that O. J. Simpson was charged with murder (“What crime was O.J. Simpson charged with?”). When E.P. was asked for more information, he stated “No, I’m blank.” G.P. stated that O.J. Simpson was associated with “murder, his wife,” then incorrectly added “I think he is in jail” and “I think she was shot. She was not strangled or stabbed.” Similarly, although E.P. correctly stated that a riot occurred following the Rodney King trial in Los Angeles (“What happened in Los Angeles following the Rodney King trial?”), he was unable to provide any other information regarding the incident. Finally, although G.P. correctly recalled that Germany was reunified (“Which previously divided European country was reunited within the last 15 years?”), on follow-up he said that this occurred in “the mid-80s” and that the new capital, “wasn’t Berlin. I want to say Bonn.” The controls again performed well on the multiple-choice test (97 ± 2% correct; Fig. 2B). In contrast, each patient scored 55% correct, not reliably above the chance score of 33% (binomial test, P = 0.18). It is possible that the score they obtained (55% correct) reflects what can be achieved by guessing on an imperfect test where the three choices are not equally plausible to an intelligent adult and where the patients might be able to make use of semantic knowledge acquired early in life. Thus, both E.P. and G.P. correctly selected Afghanistan as the country that was invaded in an effort to capture Osama Bin Laden (alternatives, Algeria and Colombia). However, neither patient was able to explain who this person was or why he was well-known. E.P. correctly selected Clinton as the Democratic president who won two terms of office during the 1990s (alternatives, Carter and Ford). However, when asked to guess his first name, he answered “Ralph” and described him as a Republican. Notably, E.P. selected the World Trade Center as the building destroyed on September 11, 2001 (G.P. answered this question incorrectly; alternatives, White House and Independence Hall). However, E.P. was unable to provide any other information. He was asked “Have you ever heard of an airplane running into a building” and he replied “seems like somebody ran into one in New York or someplace,” and added “a big building. Just crashed into it. It didn’t blow down. It burned but that’s all.” He then described the airplane as a “biplane” and estimated the event to have occurred during the 1940s. (A military plane did strike the Empire State Building in 1945, and an incident involving a biplane and the Empire State Building occurred in the 1933 film, King Kong). In any case, neither patient scored above chance levels on this multiple-choice test, so that it is difficult to attach much significance to the occasional correct answers.
FIGURE 2.
Twenty easy facts. Performance of patients E.P., G.P., and controls (CON) in response to 20 questions about information that could only have been acquired after 1988. A: Percentage correct recall. B: Percentage correct responses on a three-alternative, forced-choice recognition test. Brackets show standard error of the mean, and the dashed line indicates chance performance (33%).
2. News events (recall and recognition)
Controls scored 51 ± 6% (range = 31–76%) on the news events recall test (Fig. 3A). In contrast, patients E.P. and G.P. performed very poorly (1.8% and 3.6% correct, respectively). The single correct answer given by E.P. may have been based on knowledge about geopolitics acquired before he became amnesic. When he was asked which country invaded Kuwait, he replied “Iraq and Iran.” When asked to choose, he said “Iraq” and expressed surprise when told that his answer was correct. Patient G.P. answered only two questions correctly and knew little if anything about the relevant topics. For example, when asked to recall the name of the agreement that eases trade restrictions between the United States, Mexico, and Canada (North American Free Trade Agreement), he replied “some global name trade agreement. North American Trade Agreement. North American continental trade agreement.” When encouraged to provide further details, he replied “It unified the continent,” “It was welcome,” and stated that the agreement had been in place “about 20 years” (it had been in place 10 years). Similarly, in response to the question “Which company recalled thousands of tires due to accidents attributed to their failure?,” he correctly replied “Fire-stone.” However, he incorrectly stated that the recalled tires were on “Pontiac or Chevrolet cars” (in fact, the recall mostly concerned Ford trucks). Controls scored 85 ± 3% on the recognition test, whereas both patients performed near the chance score of 25% (E.P., 32% correct; G.P., 26% correct, P > 0.10; Fig. 3B). The patients knew little if anything about the material when their answers were correct. For example, in response to the question “What is the name of the tunnel between Britain and France running beneath the English Channel?” patient E.P. correctly selected “Eurotunnel.” However, when asked to elaborate, he replied “It was made years ago. Mid-1800s.” When asked if he was aware that a tunnel was made more recently, he stated “I don’t recall it. You mean in the last 50 years?” G.P. correctly selected “sheep” as the first animal to be cloned. However, he described cloning as “Controlling its ability to move about. Controlling its mobility,” and stated incorrectly that it happened “Here in America.”
FIGURE 3.
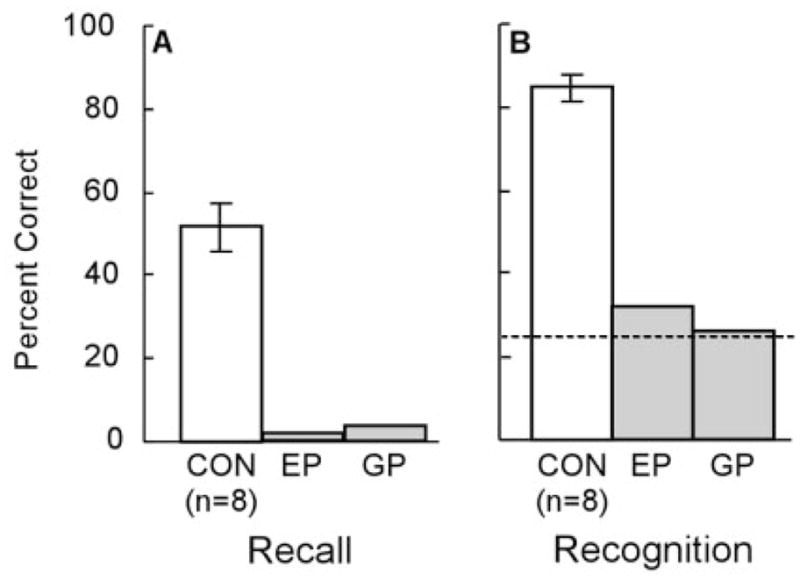
News events. Performance of patients E.P., G.P., and controls (CON) in response to 55 questions about news events that occurred from 1990 to 2000. A: Percentage correct recall. B: Percentage correct responses on a four-alternative, forced-choice recognition test. Brackets show standard error of the mean, and the dashed line indicates chance performance (25%).
3. Famous faces (recall and recognition)
Controls scored 58 ± 8% correct (range = 25–96%) on the famous faces recall test (Fig. 4A). In contrast, E.P. failed to recall a single name, and G.P. identified only one face correctly out of 24 (Colin Powell). On the recognition test (Fig. 4B), the controls scored 91 ± 2% correct (range = 83–100%). In contrast, both patients performed near the chance score of 42% (E.P., 33% correct, P > 0.10; G.P., 54% correct, P > 0.10). The patients could provide no accurate information about their few correct answers. For example, E.P. described Bob Dole as a “football player,” and Anita Hill as an “actress.” Similarly, patient G.P. could provide no additional information about the twelve famous people that he correctly recognized.
FIGURE 4.
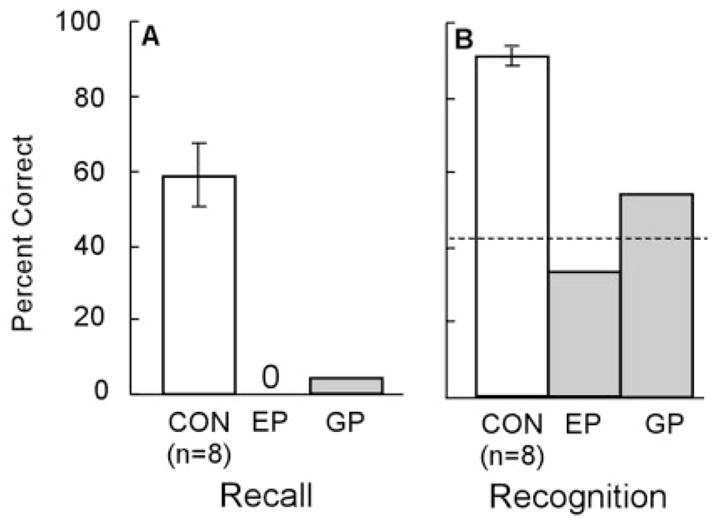
Famous faces. Performance of patients E.P., G.P., and controls (CON) in response to photographs of 24 persons who had become famous during the 1990s. A: Percentage correct recall of the name of the person. B: Percentage correct responses for recognition (both three-alternative, forced-choice recognition and yes/no recognition). Brackets show standard error of the mean, and the dashed line indicates chance performance (42%).
4. Living or nonliving famous persons
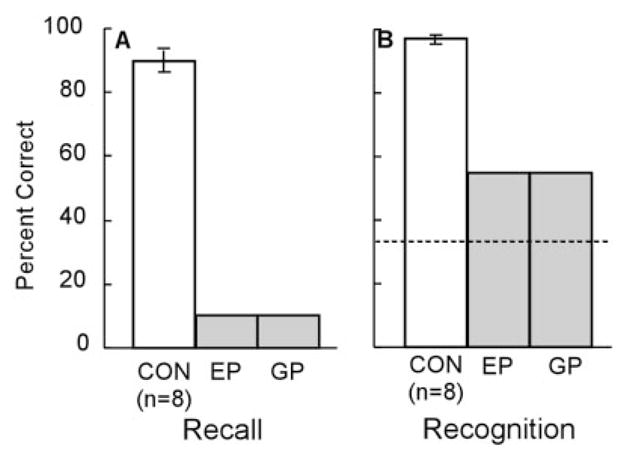
Participants were first asked to identify persons who became famous before 1970. Controls scored 96 ± 1% correct (range = 92–99%), and patients E.P. and G.P. scored 73% and 78% correct, respectively (d′ discriminability score = 3.8 ± 0.6 for controls, 1.2 for E.P., 1.5 for G.P.). Figure 5 shows performance when participants were asked to decide whether the persons they had correctly judged to be famous were living or deceased. Controls scored 73 ± 3% correct (range = 64–87%). In contrast, patients E.P. and G.P. scored near chance, 53% and 50% correct, respectively. d′ scores were also calculated: a hit was defined as a correct judgment of nonliving when the person was deceased, and a false alarm was defined as an incorrect judgment of nonliving when the person was in fact living (d′ = 1.3 ± 0.5 for controls; 0.1 for E.P.; 0.5 for G.P.). Thus, the patients had virtually no knowledge of which famous persons were living and which famous persons had died during the past 10 years.
FIGURE 5.
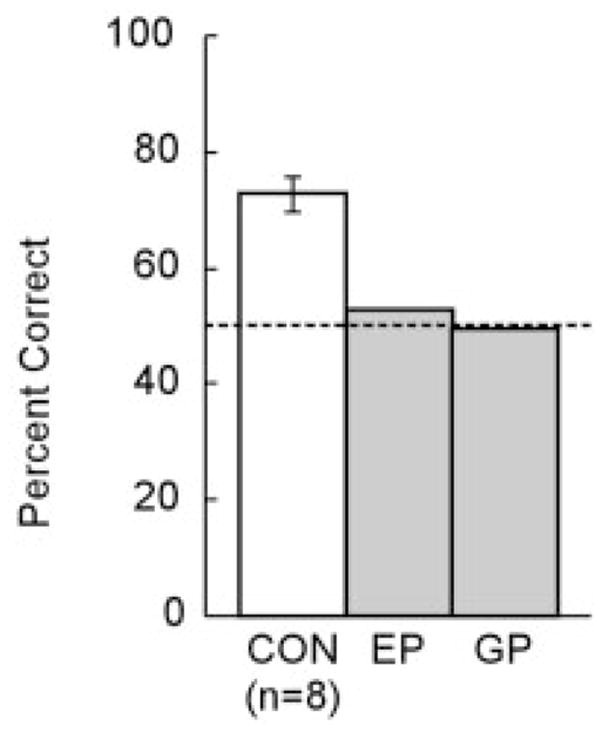
Living or nonliving famous persons. Patients E.P., G.P., and controls (CON) were first asked to identify famous persons from among 126 nonfamous names and 126 persons who had become famous before 1970. For each person correctly identified as famous, participants were then asked whether that person was still living (44% of the famous persons were still living, and 56% had died between 1990 and 2001). Brackets show standard error of the mean, and the dashed line indicates chance performance (50%).
5. Home floor plan
Figure 6 shows the floor plans of their current residences, as drawn by E.P. and G.P. E.P.’s drawing correctly indicated the overall orientation of the house relative to the front door and that the house was divided by a central corridor. However, location of individual rooms was highly inaccurate. For instance, both the bathroom and the kitchen were positioned on the wrong side of the house. G.P.’s drawing appeared even less accurate. The overall shape of the floor plan was incorrect relative to the front door. The location of rooms was highly inaccurate, and the locations of the living room and kitchen were inverted.
FIGURE 6.
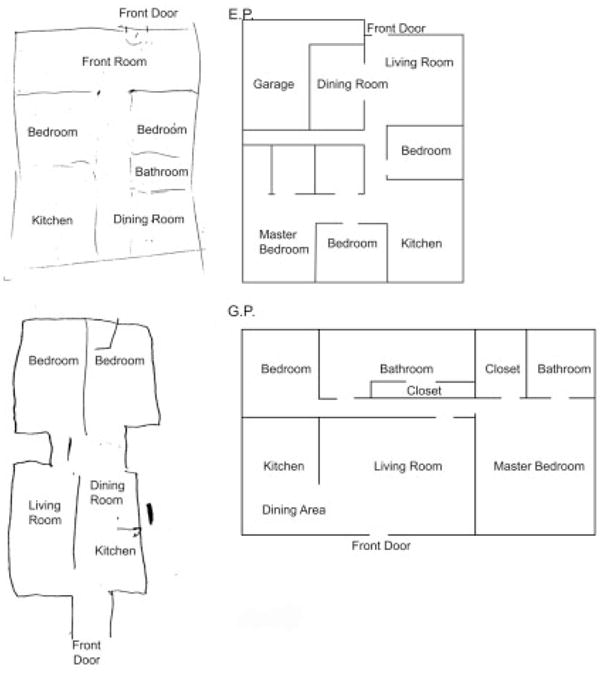
Home floor plan. Patients E.P. (top) and G.P. (bottom) were asked to draw a floor plan of their current home from memory. Both patients had moved to their current home after the onset of their amnesia. An accurate floor plan is shown alongside each patient’s drawing.
DISCUSSION
Two patients (E.P. and G.P.) with profound amnesia and large MTL lesions were given five tests of semantic knowledge for information that could only have been acquired after the onset of their amnesia in 1992 and 1987, respectively. The tests assessed knowledge about well-known facts, news events, famous faces, famous persons, and the layouts of their current homes. On the recall tests, E.P. and G.P. answered only an occasional question correctly (2 each on the 20 easy facts test; 1/55 and 2/55, respectively, on the news events test; and 0/24 and 1/24, respectively, on the famous faces test. On the recognition tests, neither patient scored above chance on any test. Lastly, neither patient could draw a creditable floor plan of his current residence.
It is of interest that the patients did produce an occasional correct answer on the recall tests (E.P.: 3/99 questions; G.P.: 5/99 questions). Yet, neither patient was able to score above chance on the three corresponding recognition tests. It is possible that some of the correct answers on the recall tests were what one might expect from a reasonably intelligent adult who was trying to guess correctly and who could draw on semantic knowledge acquired early in life. In addition, some of the correct answers may have been high-probability associations to cue words, based on long-established knowledge (e.g., the response “murder” to the cue word “crime” in the 20 easy facts test). In any case, the findings indicate that patients E.P. and G.P. have acquired little, if any, new semantic knowledge about the world since the onset of their amnesia. This conclusion fully conforms to our impressions based on hundreds of hours of contact with patients E.P. and G.P. during the past several years. E.P. and G.P. do not speak about general knowledge or factual information that was available only after they became amnesic.
The question arises as to why their intact nondeclarative memory did not support the learning of some new factual information. In a previous study, E.P. demonstrated nondeclarative (nonconscious and inflexible) learning of fact-like knowledge (three-word sentences) across 24 study sessions distributed across 12 weeks (Bayley and Squire, 2002). However, in that case, the learning depended on exact repetitions of the material to be learned, and successful retrieval depended on presenting the first two words of each three-word sentence just as they had been presented during learning. Some acquisition of nondeclarative memory in severe amnesia has also been observed with similar materials, even when the wording of the sentences was varied during learning and during retrieval (Stark et al., 2005). However, these are rather artificial conditions. Indeed, the available data suggest that nondeclarative memory is simply unsuited for supporting the acquisition and retrieval of factual knowledge under the highly variable conditions that obtain outside the laboratory. Thus, nondeclarative memory can sometimes result in the production of correct answers in highly structured settings (albeit without access to awareness that one is expressing factual knowledge). However, the ability to acquire conscious knowledge across widely varying learning conditions is the province of declarative memory.
The performance of E.P. and G.P. can be usefully compared to the performance of the noted patient H.M., who was also tested for information that he could only have acquired after he became amnesic (O’Kane et al., 2004). Whereas E.P. and G.P. failed to exhibit significant postmorbid knowledge, even on multiple-choice tests, H.M. exhibited a considerable store of postmorbid knowledge. Thus, following presentation of a first name and a semantic cue, H.M. was able to generate the last names for 66% of 35 persons who had become famous after the onset of his amnesia in 1953. Further, he scored 88% correct on a two-item recognition test for 39 famous names from his postmorbid period (chance = 50%) and was also able to provide uniquely identifying facts for 12 of the names. Lastly, on an earlier occasion, H.M. drew an accurate floor plan of the house where he had lived for 16 years after he became amnesic (Corkin, 2002).
As described by O’Kane et al. (2004), the information available to H.M. is accessible to conscious awareness and can be expressed flexibly, i.e., regardless of what wording is used to frame the question. Accordingly, the information he has acquired is best understood as reflecting a robust capacity to acquire declarative knowledge. To be sure, H.M.’s performance is far from normal. He has consistently exhibited severe deficits in semantic knowledge for postmorbid information (Marslen-Wilson and Teuber, 1975; O’Kane et al., 2004). Nevertheless, in contrast to E.P. and G.P., H.M. has acquired a substantial amount of factual knowledge since he became amnesic.
It is unlikely that H.M.’s better performance is simply due to the fact that H.M. has been amnesic for longer than E.P. or G.P. (50 years vs. 11 and 16 years, as of 2003), and that he has therefore had a greater number of learning opportunities. First, H.M. exhibited knowledge about persons who became famous as recently as the 1980s, who could only have been learned about since that time (O’Kane et al., 2004). He also scored above chance at distinguishing recently adopted English words from nonwords (Gabrieli et al., 1988). Second, neither E.P. nor G.P. could draw an accurate floor plan of his home, despite having lived there for approximately 10 years and 1 year, respectively, and despite having had what must amount to thousands of learning opportunities. It should be noted that E.P. is able to recall accurate and detailed information about the spatial layout of the neighborhood in which he grew up (Teng and Squire, 1999). He is also able to copy a complex figure as accurately as control subjects (Stefanacci et al., 2000). Thus, E.P.’s failure to draw an accurate floor plan of his current residence cannot be due to visuospatial deficits or to particular difficulties in constructing spatial maps.
It seems most likely, as suggested by O’Kane et al. (2004), that H.M. has succeeded at acquiring new factual knowledge after the onset of his amnesia because his damage is less extensive than the damage in E.P. and G.P. H.M.’s MTL damage includes the hippocampus and the entorhinal cortex but spares the parahippocampal cortex and ventrocaudal perirhinal cortex. In contrast, the MTL damage in E.P. and G.P. includes the hippocampus, the entorhinal cortex, as well as all of the perirhinal cortex and most of the parahippocampal cortex (73% bilaterally for E.P. and 71% bilaterally for G.P.).
O’Kane et al. (2004) pointed out that H.M.’s ability to acquire significant postmorbid knowledge, together with the fact that H.M. has no functional hippocampus, indicates that structures beyond the hippocampus itself must be responsible for his successful learning. The present findings with E.P. and G.P. indicate that the ability to acquire semantic knowledge depends on the structures beyond the hippocampus that are damaged in these two patients. These structures are the perirhinal cortex and parahippocampal cortex within the MTL and the fusiform gyrus and insula more laterally.
A number of considerations suggest that the ability to acquire semantic knowledge depends on MTL structures (not the fusiform gyrus or insula). First, patients with extensive lateral temporal damage typically maintain a considerable capacity for new semantic learning. For example, in patients with focal retrograde amnesia (Kapur, 1993), there is bilateral damage to the anterior and inferior temporal lobes. Yet, MTL structures are largely intact, and these structures presumably work in concert with intact areas of neocortex to support new semantic learning. In addition, patients with semantic dementia (Hodges and Graham, 2001) have extensive damage to the anterolateral temporal lobes, including the fusiform gyrus (which is reduced in volume to a similar degree as in E.P. and G.P.; Chan et al., 2001; Galton et al., 2001), as well as deficits in long-established semantic knowledge (Mummery et al., 2000; Levy et al., 2004). Yet, despite their lateral temporal lobe damage, these patients can demonstrate some new semantic learning as well as some knowledge of currently famous personalities (Funnell, 1995; Hodges and Graham, 1998), and they are more successful in this regard than are E.P. or G.P. For example, one patient was able to learn the names of products, magazines, and television programs and to remember some of this information for at least 6 weeks after the completion of training (Graham et al., 1999). Two other patients were able to reacquire the names of simple objects depicted by line drawings and to remember some of the information for a few months (Snowden and Neary, 2002). Patients with semantic dementia do have some atrophy within the MTL (Chan et al., 2001; Galton et al., 2001), and new learning can be impaired (Simons et al., 2002). However, new semantic learning is presumably more successful for these patients than for E.P. and G.P. because patients with semantic dementia have less volume loss within MTL structures than do patients E.P. and G.P. (Levy et al., 2004). In summary, it is clear that structures lateral to the MTL are not as important for new semantic learning as are the structures of the MTL itself. Nonetheless, the damage in E.P. and G.P. does extend laterally a little beyond the MTL, and one cannot exclude the possibility that this damage did contribute to the severity of their impairment.
The present results emphasize the importance of the MTL for the acquisition of factual information. Although most memory-impaired patients have some ability to learn new facts, it is also the case that most patients available for study have significant sparing of structures within the MTL. Patients E.P. and G.P. demonstrate that the capacity for new semantic learning can be absent, or nearly absent. We suggest that this condition occurs when there is nearly complete damage to the MTL bilaterally. These findings raise the possibility that the acquisition of declarative knowledge cannot be supported by structures outside the MTL, even after extended exposure.
Acknowledgments
The authors thank Jennifer Frascino, Leah Swalley, and Jeffery Gold for assistance, and Dr. T. Jernigan for providing magnetic resonance images of control brains.
Grant sponsor: Medical Research of the Department of Veterans Affairs; Grant sponsor: National Institute of Mental Health (NIMH); Grant number: MH24600; Grant sponsor: Metropolitan Life Foundation.
References
- Amaral DG, Insausti R. Hippocampal formation. In: Paxinos G, editor. The human nervous system. San Diego, CA: Academic Press; 1990. [Google Scholar]
- Bayley PJ, Hopkins RO, Squire LR. Successful recollection of remote autobiographical memories by amnesic patients with medial temporal lobe lesions. Neuron. 2003;38:135–144. doi: 10.1016/s0896-6273(03)00156-9. [DOI] [PubMed] [Google Scholar]
- Bayley PJ, Squire LR. Medial temporal lobe amnesia: gradual acquisition of factual information by nondeclarative memory. J Neurosci. 2002;22:5741–5748. doi: 10.1523/JNEUROSCI.22-13-05741.2002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chan D, Fox N, Scahill R, Crum W, Whitwell J, Leschziner M, Rossor A, Steven J, Cipolotti L, Rossor M. Patterns of temporal lobe atrophy in semantic dementia and Alzheimer’s disease. Ann Neurol. 2001;49:433–442. [PubMed] [Google Scholar]
- Corkin S. What’s new with the amnesic patient H.M.? Nat Rev Neurosci. 2002;3:153–160. doi: 10.1038/nrn726. [DOI] [PubMed] [Google Scholar]
- Corkin S, Amaral DG, Gonzalez RG, Johnson KA, Hyman BT. H.M.’s medial temporal lobe lesion: findings from magnetic resonance imaging. J Neurosci. 1997;17:3964–3980. doi: 10.1523/JNEUROSCI.17-10-03964.1997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eichenbaum H, Cohen NJ. From conditioning to conscious recollection: memory systems of the brain. New York: Oxford University Press; 2001. [Google Scholar]
- Funnell E. A case of forgotten knowledge. In: Campbell R, Conway M, editors. Broken memories. Oxford, England: Blackwell; 1995. pp. 225–236. [Google Scholar]
- Gabrieli JD, Cohen NJ, Corkin S. The impaired learning of semantic knowledge following bilateral medial temporal-lobe resection. Brain Cogn. 1988;7:157–177. doi: 10.1016/0278-2626(88)90027-9. [DOI] [PubMed] [Google Scholar]
- Galton CJ, Patterson K, Graham K, Lambon-Ralph MA, Williams G, Antoun N, Sahakian BJ, Hodges JR. Differing patterns of temporal atrophy in Alzheimer’s disease and semantic dementia. Neurology. 2001;57:216–225. doi: 10.1212/wnl.57.2.216. [DOI] [PubMed] [Google Scholar]
- Gold JJ, Squire LR. Quantifying medial temporal lobe damage in memory-impaired patients. Hippocampus. 2004 doi: 10.1002/hipo.20032. (in press) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Graham KS, Patterson K, Pratt K, Hodges JR. Relearning and subsequent forgetting of semantic category exemplars in a case of semantic dementia. Neuropsychology. 1999;13:359–380. doi: 10.1037//0894-4105.13.3.359. [DOI] [PubMed] [Google Scholar]
- Hamann SB, Squire LR. On the acquisition of new declarative knowledge in amnesia. Behav Neurosci. 1995;109:1027–1044. doi: 10.1037//0735-7044.109.6.1027. [DOI] [PubMed] [Google Scholar]
- Hodges JR, Graham KS. A reversal of the temporal gradient for famous person knowledge in semantic dementia: implications for the neural organization of long-term memory. Neuropsychologia. 1998;36:803–825. doi: 10.1016/s0028-3932(97)00126-7. [DOI] [PubMed] [Google Scholar]
- Hodges JR, Graham KS. Episodic memory: insights from semantic dementia. Philos Trans R Soc Lond B Biol Sci. 2001;356:1423–1434. doi: 10.1098/rstb.2001.0943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holdstock JS, Mayes AR, Roberts N, Cezayirli E, Isaac CL, O’Reilly RC, Norman KA. Under what conditions is recognition spared relative to recall after selective hippocampal damage in humans? Hippocampus. 2002;12:341–351. doi: 10.1002/hipo.10011. [DOI] [PubMed] [Google Scholar]
- Insausti R, Juottonen K, Soininen H, Insausti AM, Partanen K, Vainio P, Laakso MP, Pitkanen A. MR volumetric analysis of the human entorhinal, perirhinal, and temporopolar cortices. Am J Neuroradiol. 1998;19:659–671. [PMC free article] [PubMed] [Google Scholar]
- Kapur N. Focal retrograde amnesia in neurological disease: a critical review. Cortex. 1993;29:217–234. doi: 10.1016/s0010-9452(13)80177-3. [DOI] [PubMed] [Google Scholar]
- Kitchener EG, Hodges JR, McCarthy R. Acquisition of post-morbid vocabulary and semantic facts in the absence of episodic memory. Brain. 1998;121:1313–1327. doi: 10.1093/brain/121.7.1313. [DOI] [PubMed] [Google Scholar]
- Levy DA, Bayley PJ, Squire LR. The anatomy of semantic knowledge: medial vs. lateral temporal lobe. Proc Natl Acad Sci USA. 2004;101:6710–6715. doi: 10.1073/pnas.0401679101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manns JR, Hopkins RO, Squire LR. Semantic memory and the human hippocampus. Neuron. 2003;37:127–133. doi: 10.1016/s0896-6273(03)00146-6. [DOI] [PubMed] [Google Scholar]
- Marslen-Wilson WD, Teuber HL. Memory for remote events in anterograde amnesia: recognition of public figures from news photographs. Neuropsychologia. 1975;13:353–364. doi: 10.1016/0028-3932(75)90013-5. [DOI] [PubMed] [Google Scholar]
- McClelland JL, McNaughton BL, O’Reilly RC. Why there are complementary learning systems in the hippocampus and neocortex: insights from the successes and failures of connectionist models of learning and memory. Psychol Rev. 1995;3:419–457. doi: 10.1037/0033-295X.102.3.419. [DOI] [PubMed] [Google Scholar]
- Mummery C, Patterson K, Price C, Ashburner J, Frackowiak R, Hodges JR. A voxel-based morphometry study of semantic dementia: relationship between temporal lobe atrophy and semantic memory. Ann Neurol. 2000;47:36–45. [PubMed] [Google Scholar]
- O’Kane G, Kensinger EH, Corkin S. Evidence for semantic learning in profound amnesia: an investigation with the patient H.M. Hippocampus. 2004;14:417–425. doi: 10.1002/hipo.20005. [DOI] [PubMed] [Google Scholar]
- Reed JM, Squire LR. Retrograde amnesia for facts and events: findings from four new cases. J Neurosci. 1998;18:3943–3954. doi: 10.1523/JNEUROSCI.18-10-03943.1998. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmolck H, Kensinger E, Corkin S, Squire LR. Semantic knowledge in patient H.M. and other patients with bilateral medial and lateral temporal lobe lesions. Hippocampus. 2002;12:520–533. doi: 10.1002/hipo.10039. [DOI] [PubMed] [Google Scholar]
- Shimamura AP, Squire LR. Long-term memory in amnesia: cued recall, recognition memory, and confidence ratings. J Exp Psychol Learn Mem Cogn. 1988;14:763–770. doi: 10.1037//0278-7393.14.4.763. [DOI] [PubMed] [Google Scholar]
- Simons JS, Graham KS, Hodges JR. Perceptual and semantic contributions to episodic memory: evidence from semantic dementia and Alzheimer’s disease. J Mem Lang. 2002;47:197–213. [Google Scholar]
- Snowden JS, Neary D. Relearning of verbal labels in semantic dementia. Neuropsychologia. 2002;40:1715–1728. doi: 10.1016/s0028-3932(02)00031-3. [DOI] [PubMed] [Google Scholar]
- Squire LR. Declarative and nondeclarative memory: multiple brain systems support learning and memory. J Cogn Neurosci. 1992;4:232–243. doi: 10.1162/jocn.1992.4.3.232. [DOI] [PubMed] [Google Scholar]
- Stark CEL, Squire LR. Intact visual perceptual discrimination in humans in the absence of perirhinal cortex. Learn Mem. 2000;7:273–278. doi: 10.1101/lm.35000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stark CEL, Stark S, Gordon B. New semantic learning and generalization in an amnesic patient. Neuropsychology. doi: 10.1037/0894-4105.19.2.139. (in press) [DOI] [PubMed] [Google Scholar]
- Stefanacci L, Buffalo EA, Schmolck H, Squire LR. Profound amnesia following damage to the medial temporal lobe: a neuroanatomical and neuropsychological profile of patient E.P. J Neurosci. 2000;20:7024–7036. doi: 10.1523/JNEUROSCI.20-18-07024.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teng E, Squire LR. Memory for places learned long ago is intact after hippocampal damage. Nature. 1999;400:675–677. doi: 10.1038/23276. [DOI] [PubMed] [Google Scholar]
- Tulving E. Elements of episodic memory. Cambridge: Oxford University Press; 1983. [Google Scholar]
- Tulving E, Squire LR, Weinberger NM, Lynch G, McGaugh JL. Concepts in human memory Memory: organization and locus of change. New York: Oxford University Press; 1991. pp. 3–32. [Google Scholar]
- Tulving E, Hayman G, Macdonald CA. Long-lasting perceptual priming and semantic learning in amnesia: a case experiment. J Exp Psychol Mem Cogn. 1991;17:595–617. doi: 10.1037//0278-7393.17.4.595. [DOI] [PubMed] [Google Scholar]
- Tulving E, Markowitsch HJ. Episodic and declarative memory: role of the hippocampus. Hippocampus. 1998;8:198–204. doi: 10.1002/(SICI)1098-1063(1998)8:3<198::AID-HIPO2>3.0.CO;2-G. [DOI] [PubMed] [Google Scholar]
- Verfaellie M, Koseff P, Alexander MP. Acquisition of novel semantic information in amnesia: effects of lesion location. Neuropsychologia. 2000;38:484–492. doi: 10.1016/s0028-3932(99)00089-5. [DOI] [PubMed] [Google Scholar]
- Westmacott R, Moscovitch M. Names and words without meaning: incidental postmorbid semantic learning in a person with extensive bilateral medial temporal lobe damage. Neuropsychology. 2001;15:586–596. doi: 10.1037//0894-4105.15.4.586. [DOI] [PubMed] [Google Scholar]