Glycyrrhizin, an active component of liquorice roots, and replication of SARS-associated coronavirus (original) (raw)
Summary
The outbreak of SARS warrants the search for antiviral compounds to treat the disease. At present, no specific treatment has been identified for SARS-associated coronavirus infection. We assessed the antiviral potential of ribavirin, 6-azauridine, pyrazofurin, mycophenolic acid, and glycyrrhizin against two clinical isolates of coronavirus (FFM-1 and FFM-2) from patients with SARS admitted to the clinical centre of Frankfurt University, Germany. Of all the compounds, glycyrrhizin was the most active in inhibiting replication of the SARS-associated virus. Our findings suggest that glycyrrhizin should be assessed for treatment of SARS.
A new coronavirus has been identified in patients with severe acute respiratory syndrome (SARS).1 SARS is an infectious disease with a high potential for transmission to close contacts. The outbreak of SARS in several countries has led to the search for active antiviral compounds to treat this disease.
Here, we assessed the antiviral activities of ribavirin, 6-azauridine, pyrazofurin, mycophenolic acid, and glycyrrhizin against two clinical isolates of coronavirus (FFM-1 and FFM-2) from patients with SARS admitted to the clinical centre of Frankfurt University, Germany. All the compounds are available commercially and have been used in patients for their antiviral, antitumour, and immunosuppressive activity. We visually scored cytopathogenicity induced by the virus 72–96 h after infection in 96-well microplates on confluent layers of Vero cells. The selectivity index was determined as the ratio of the concentration of the compound that reduced cell viability to 50% (CC50) to the concentration of the compound needed to inhibit the cytopathic effect to 50% of the control value (EC50). We determined the cytotoxicity of the drugs with an MMT cell-proliferative Kit I (Roche, Mannheim, Germany).
Ribavirin and mycophenolic acid, inhibitors of inosine monophosphate dehydrogenase, did not affect replication of the SARS-associated coronaviruses (SARS-CV) (table). The inhibitors of orotidine monophosphate decarboxylase, 6-azauridine and pyrazofurin, inhibited replication of SARS-CV at non-toxic doses with selectivity indices of 5 and 12, respectively. The most potent inhibitor of SARS-CV replication in Vero cells was glycyrrhizin, which had a selectivity index of 67.
Table.
Activity of compounds against SARS-associated coronavirus in Vero cell cultures
| EC50*(mg/L) | CC50*(mg/L) | Selectivity index | |
|---|---|---|---|
| Compound | |||
| 6-azauridine | 16·8 (2·9) | 104 (18) | 6 |
| Pyrazofurin | 4·2 (0·57) | 52 (9·6) | 12 |
| Mycophenolic acid | >50 | >50 | NC |
| Ribavirin | >1000 | >1000 | NC |
| Glycyrrhizin | |||
| After virus adsorption | 600 (72) | >20000† | >33 |
| During and after virus adsorption | 300 (51) | >20000 | >67 |
| During virus adsorption | 2400 (410) | >20000 | >8·3 |
In addition to inhibition of virus replication, glycyrrhizin inhibits adsorption and penetration of the virus—early steps of the replicative cycle. Glycyrrhizin was less effective when added during the adsorption period than when added after virus adsorption (EC50 600 mg/L vs 2400 mg/L, respectively). Glycyrrhizin was most effective when given both during and after the adsorption period (EC50 300 mg/L).
The figureshows the effect of glycyrrhizin on replication of SARS-CV in Vero cells. We detected replication of SARS-CV with serum samples from patients with SARS. Expression of viral antigens was much lower in cultures treated with 1000 mg/L of glycyrrhizin than in any other culture; high concentrations of glycyrrhizin (4000 mg/L) completely blocked replication of the virus (figure).
Figure.
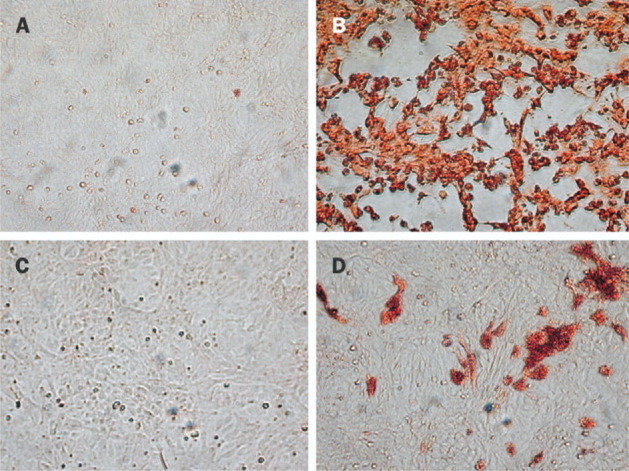
Effect of glycyrrhizin on replication of SARS-associated coronavirus in Vero cells
Cells were fixed with 60 parts methanol to 40 parts acetone 72 h after infection. Virus was detected in serum from the patient with SARS by peroxidase staining. (A) mock infected cells. (B) infected cells without treatment. (C) infected cells treated with 4000 mg/L glycyrrhizin. (D) infected cells treated with 1000 mg/L glycyrrhizin.
In a comparison of the antiviral potential of 6-azauridine, ribavirin, and glycyrrhizin against several pathogenic flaviviruses, Crance and collegues2 showed that ribavirin and 6-azauridine were active but not selective inhibitors when assessed with regard to inhibition of cell growth. Glycyrrhizin had a low selectivity index, but was a significantly potent inhibitor of replication of all the viruses tested. The EC50 reported by these authors for glycyrrhizin was 316–625 mg/L (added twice during the incubation period of 7 days). Taking into consideration that the compounds were added twice during the total period of incubation, the EC50 for glycyrrhizin we recorded (table) indicates a higher sensitivity of SARS-CV to this drug than that recorded by Crance and colleagues.
The mechanism of glycyrrhizin's activity against SARS-CV is unclear. Glycyrrhizin affects cellular signalling pathways such as protein kinase C; casein kinase II; and transcription factors such as activator protein 1 and nuclear factor κB. Furthermore, glycyrrhizin and its aglycone metabolite 18β glycyrrhetinic acid upregulate expression of inducible nitrous oxide synthase and production of nitrous oxide in macrophages.3 Nitrous oxide inhibits replication of several viruses—eg, Japanese encephalitis virus4 (a member of the Flaviviridae family), which can also be inhibited by glycyrrhizin.2 Our preliminary results show that glycyrrhizin induces nitrous oxide synthase in Vero cells and that virus replication is inhibited when the nitrous oxide donor (BETA NONOate) is added to the culture medium.
Glycyrrhizin has previously been used to treat patients with HIV-1 and chronic hepatitis C virus. The resulting low concentrations of P24 antigen in patients with HIV-1 who were given this compound has been attributed to upregulation of chemokines. Infrequent side-effects such as raised blood pressure and hypokalaemia were reported in some patients after several months of glycyrrhizin treatment. Treatment of SARS should only be needed for a short time. Since the side-effects of this compound are known and can be controlled for, proper monitoring could lead to effective use of glycyrrhizin as a treatment for SARS. Booth and colleagues5 reported that ribavirin had many toxic effects when given to patients with SARS, including haemolysis (76% of patients) and a drastic reduction of haemoglobin (49% of patients). However, although high doses of glycyrrhizin have been used in clinical trials, this compound had few toxic effects compared with the other regimens, and the drug was reported to be clinically effective.
Future search for compounds of therapeutic interest against SARS will be greatly facilitated by establishing growth of SARS-CV in human cells.
References
- 1.Drosten C, Gunther S, Preiser W. Identification of a novel coronavirus in patients with severe acute respiratory syndrome. N Engl J Med. 2003;348:1967–1976. doi: 10.1056/NEJMoa030747. [DOI] [PubMed] [Google Scholar]
- 2.Crance JM, Scaramozzino N, Jouan A, Garin D. Interferon, ribavirin, 6-azauridine, and glycyrrhizin: antiviral compounds active against pathogenic flaviviruses. Antiviral Res. 2003;58:73–79. doi: 10.1016/s0166-3542(02)00185-7. [DOI] [PubMed] [Google Scholar]
- 3.Jeong HG, Kim JY. Induction of inducible nitric oxide synthase expression by 18β-glycyrrhetinic acid in macrophages. FEBS Lett. 2002;513:208–212. doi: 10.1016/s0014-5793(02)02311-6. [DOI] [PubMed] [Google Scholar]
- 4.Lin YL, Huang YL, Ma SH. Inhibition of Japanese encephalitis virus infection by nitric oxide: antiviral effect of nitric oxide on RNA virus replication. J Virol. 1997;71:5227–5235. doi: 10.1128/jvi.71.7.5227-5235.1997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Booth CM, Matukas LM, Tomlinson GA. Clinical features and short-term outcomes of 144 patients with SARS in the greater Toronto area. JAMA. 2003;289:1–9. doi: 10.1001/jama.289.21.JOC30885. [DOI] [PubMed] [Google Scholar]