Invasive Fungal Diseases in Adult Patients in Intensive Care Unit (FUNDICU): 2024 consensus definitions from ESGCIP, EFISG, ESICM, ECMM, MSGERC, ISAC, and ISHAM (original) (raw)
Abstract
Purpose
The aim of this document was to develop standardized research definitions of invasive fungal diseases (IFD) in non-neutropenic, adult patients without classical host factors for IFD, admitted to intensive care units (ICUs).
Methods
After a systematic assessment of the diagnostic performance for IFD in the target population of already existing definitions and laboratory tests, consensus definitions were developed by a panel of experts using the RAND/UCLA appropriateness method.
Results
Standardized research definitions were developed for proven invasive candidiasis, probable deep-seated candidiasis, proven invasive aspergillosis, probable invasive pulmonary aspergillosis, and probable tracheobronchial aspergillosis. The limited evidence on the performance of existing definitions and laboratory tests for the diagnosis of IFD other than candidiasis and aspergillosis precluded the development of dedicated definitions, at least pending further data. The standardized definitions provided in the present document are aimed to speed-up the design, and increase the feasibility, of future comparative research studies.
Introduction
Invasive fungal diseases (IFD) are widely recognized as a cause of morbidity and mortality in immunocompromised patients, but can also occur in non-neutropenic, adult patients admitted to intensive care unit (ICU), without classical host factors for IFD [[1](#ref-CR1 "Bassetti M, Bouza E (2017) Invasive mould infections in the ICU setting: complexities and solutions. J Antimicrob Chemother 72(supp_l 1):39–47. https://doi.org/10.1093/jac/dkx032
"),[2](#ref-CR2 "Bassetti M, Giacobbe DR, Vena A et al (2019) Incidence and outcome of invasive candidiasis in intensive care units (ICUs) in Europe: results of the EUCANDICU project. Crit Care 23(1):219.
https://doi.org/10.1186/s13054-019-2497-3
"),[3](#ref-CR3 "Delaloye J, Calandra T (2014) Invasive candidiasis as a cause of sepsis in the critically ill patient. Virulence 5(1):161–169.
https://doi.org/10.4161/viru.26187
"),[4](#ref-CR4 "Ostrosky-Zeichner L, Al-Obaidi M (2017) Invasive fungal infections in the intensive care unit. Infect Dis Clin N Am 31(3):475–487.
https://doi.org/10.1016/j.idc.2017.05.005
"),[5](/article/10.1007/s00134-024-07341-7#ref-CR5 "Taccone FS, Van den Abeele AM, Bulpa P et al (2015) Epidemiology of invasive aspergillosis in critically ill patients: clinical presentation, underlying conditions, and outcomes. Crit Care 19:7.
https://doi.org/10.1186/s13054-014-0722-7
")\].The population of non-neutropenic, critically ill adult patients is highly heterogenous, including medical and surgical patients, with a wide range of baseline comorbidities and predisposing conditions for IFD [[6](#ref-CR6 "Bassetti M, Righi E, Ansaldi F et al (2015) A multicenter multinational study of abdominal candidiasis: epidemiology, outcomes and predictors of mortality. Intensive Care Med 41(9):1601–1610. https://doi.org/10.1007/s00134-015-3866-2
"),[7](#ref-CR7 "Kluge S, Strauss R, Kochanek M, Weigand MA, Rohde H, Lahmer T (2021) Aspergillosis: emerging risk groups in critically ill patients. Med Mycol.
https://doi.org/10.1093/mmy/myab064
"),[8](#ref-CR8 "Leroy O, Gangneux JP, Montravers P et al (2009) Epidemiology, management, and risk factors for death of invasive Candida infections in critical care: a multicenter, prospective, observational study in France (2005–2006). Crit Care Med 37(5):1612–1618.
https://doi.org/10.1097/CCM.0b013e31819efac0
"),[9](#ref-CR9 "Prattes J, Wauters J, Giacobbe DR et al (2022) Risk factors and outcome of pulmonary aspergillosis in critically ill coronavirus disease 2019 patients-a multinational observational study by the European Confederation of Medical Mycology. Clin Microbiol Infect 28(4):580–587.
https://doi.org/10.1016/j.cmi.2021.08.014
"),[10](#ref-CR10 "Salmanton-Garcia J, Sprute R, Stemler J et al (2021) COVID-19-associated pulmonary aspergillosis, March–August 2020. Emerg Infect Dis 27(4):1077–1086.
https://doi.org/10.3201/eid2704.204895
"),[11](#ref-CR11 "Schauwvlieghe A, Rijnders BJA, Philips N et al (2018) Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: a retrospective cohort study. Lancet Respir Med 6(10):782–792.
https://doi.org/10.1016/S2213-2600(18)30274-1
"),[12](/article/10.1007/s00134-024-07341-7#ref-CR12 "Janssen NAF, Nyga R, Vanderbeke L et al (2021) Multinational observational cohort study of COVID-19-associated pulmonary aspergillosis (1). Emerg Infect Dis 27(11):2892–2898.
https://doi.org/10.3201/eid2711.211174
")\]. Together with the frequent absence of classical host factors predisposing to IFD, such as neutropenia, hematological malignancies, or solid organ transplantation (SOT), this wide heterogeneity has led to the development of different definitions of IFD in this patient population, each with different denominators (i.e., different subgroups of critically ill patients by predisposing factors/conditions) \[[13](#ref-CR13 "Bassetti M, Marchetti M, Chakrabarti A et al (2013) A research agenda on the management of intra-abdominal candidiasis: results from a consensus of multinational experts. Intensive Care Med 39(12):2092–2106.
https://doi.org/10.1007/s00134-013-3109-3
"),[14](#ref-CR14 "Blot SI, Taccone FS, Van den Abeele AM et al (2012) A clinical algorithm to diagnose invasive pulmonary aspergillosis in critically ill patients. Am J Respir Crit Care Med 186(1):56–64.
https://doi.org/10.1164/rccm.201111-1978OC
"),[15](#ref-CR15 "Bulpa P, Dive A, Sibille Y (2007) Invasive pulmonary aspergillosis in patients with chronic obstructive pulmonary disease. Eur Respir J 30(4):782–800.
https://doi.org/10.1183/09031936.00062206
"),[16](#ref-CR16 "Koehler P, Bassetti M, Chakrabarti A et al (2021) Defining and managing COVID-19-associated pulmonary Aspergillosis: the 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect Dis 21(6):e149–e162.
https://doi.org/10.1016/S1473-3099(20)30847-1
"),[17](#ref-CR17 "Vandewoude KH, Blot SI, Depuydt P et al (2006) Clinical relevance of Aspergillus isolation from respiratory tract samples in critically ill patients. Crit Care 10(1):R31.
https://doi.org/10.1186/cc4823
"),[18](#ref-CR18 "Verweij PE, Bruggemann RJM, Azoulay E et al (2021) Taskforce report on the diagnosis and clinical management of COVID-19 associated pulmonary aspergillosis. Intensive Care Med 47(8):819–834.
https://doi.org/10.1007/s00134-021-06449-4
"),[19](/article/10.1007/s00134-024-07341-7#ref-CR19 "Verweij PE, Rijnders BJA, Bruggemann RJM et al (2020) Review of influenza-associated pulmonary aspergillosis in ICU patients and proposal for a case definition: an expert opinion. Intensive Care Med 46(8):1524–1535.
https://doi.org/10.1007/s00134-020-06091-6
")\]. While certainly useful for providing information on the burden of IFD and for increasing awareness and recognition of IFD in specific categories of critically ill patients (e.g., patients with chronic obstructive pulmonary disease \[COPD\], influenza, or coronavirus disease 2019 \[COVID-19\]), these definitions remain of limited generalizability outside the specific populations for which they were developed.The Invasive Fungal Diseases in Adult Patients in ICU (FUNDICU) project was conceived with the aim of developing a standard set of definitions for IFD in non-neutropenic, ICU patients outside the classical immunocompromised patient populations, which could improve the generalizability and comparability of research results. The FUNDICU definitions have been developed for clinical research, and not for clinical practice. Furthermore, they are not meant to replace but rather to complement the definitions of IFD provided by the European Organization for Research and Treatment of Cancer (EORTC) and the Mycoses Study Group Education and Research Consortium (MSGERC) [[20](/article/10.1007/s00134-024-07341-7#ref-CR20 "Donnelly JP, Chen SC, Kauffman CA et al (2020) Revision and update of the consensus definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis 71(6):1367–1376. https://doi.org/10.1093/cid/ciz1008
")\]. The EORTC/MSGERC consensus document remains the reference for standardized IFD definitions in patients with classical host factors, even when they are admitted to the ICU. More in detail, the definitions of IFD included in the present document do not apply to those ICU patients who fulfill the EORTC/MSGERC host factors: (i) hematology and SOT patients; (ii) prolonged use of corticosteroids; (iii) treatment with other recognized T-cell immunosuppressants; (iv) treatment with recognized B-cell immunosuppressants; (v) inherited severe immunodeficiency; (vi) acute graft-versus-host disease grade III or IV involving the gut, lung, or liver and refractory to first-line treatment with steroids \[[20](/article/10.1007/s00134-024-07341-7#ref-CR20 "Donnelly JP, Chen SC, Kauffman CA et al (2020) Revision and update of the consensus definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis 71(6):1367–1376.
https://doi.org/10.1093/cid/ciz1008
")\].Methods
The detailed protocol of the FUNDICU project has been published previously [[21](/article/10.1007/s00134-024-07341-7#ref-CR21 "Bassetti M, Scudeller L, Giacobbe DR et al (2019) Developing definitions for invasive fungal diseases in critically ill adult patients in intensive care units. Protocol of the FUNgal infections Definitions in ICU patients (FUNDICU) project. Mycoses 62(4):310–319. https://doi.org/10.1111/myc.12869
")\]. A multidisciplinary panel of experts was selected by the chairs of the Critically Ill Patients Study Group (ESGCIP) and the Fungal Infections Study Group (EFISG) of the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) \[[21](/article/10.1007/s00134-024-07341-7#ref-CR21 "Bassetti M, Scudeller L, Giacobbe DR et al (2019) Developing definitions for invasive fungal diseases in critically ill adult patients in intensive care units. Protocol of the FUNgal infections Definitions in ICU patients (FUNDICU) project. Mycoses 62(4):310–319.
https://doi.org/10.1111/myc.12869
")\]. The panel was approved by the Executive Committees of ESGCIP and EFISG, and then by the relevant bodies/committees of the European Society of Intensive Care Medicine (ESICM), the European Confederation of Medical Mycology (ECMM), and the MSGERC \[[21](/article/10.1007/s00134-024-07341-7#ref-CR21 "Bassetti M, Scudeller L, Giacobbe DR et al (2019) Developing definitions for invasive fungal diseases in critically ill adult patients in intensive care units. Protocol of the FUNgal infections Definitions in ICU patients (FUNDICU) project. Mycoses 62(4):310–319.
https://doi.org/10.1111/myc.12869
")\]. The second step was to identify the existing relevant literature on the performance of existing definitions and tests for the diagnosis of different IFDs in the target population. Four different systematic reviews were conducted, with subsequent updates of the literature searches up to 31 March 2022\. Their results were published and used to develop the initial definitions, which were discussed and approved by the expert panel \[[22](#ref-CR22 "Bassetti M, Giacobbe DR, Grecchi C et al (2020) Performance of existing definitions and tests for the diagnosis of invasive aspergillosis in critically ill, adult patients: a systematic review with qualitative evidence synthesis. J Infect 81(1):131–146.
https://doi.org/10.1016/j.jinf.2020.03.065
"),[23](#ref-CR23 "Giacobbe DR, Cortegiani A, Karaiskos I et al (2021) Performance of existing definitions and tests for the diagnosis of invasive fungal diseases other than invasive candidiasis and invasive aspergillosis in critically ill, adult patients: a systematic review with qualitative evidence synthesis. J Fungi (Basel, Switzerland) 7(3):176.
https://doi.org/10.3390/jof7030176
"),[24](#ref-CR24 "Giacobbe DR, Asperges E, Cortegiani A et al (2022) Performance of existing clinical scores and laboratory tests for the diagnosis of invasive candidiasis in critically ill, nonneutropenic, adult patients: a systematic review with qualitative evidence synthesis. Mycoses 65(12):1073–1111.
https://doi.org/10.1111/myc.13515
"),[25](/article/10.1007/s00134-024-07341-7#ref-CR25 "Bassetti M, Zuccaro V, Asperges E, Scudeller L, Giacobbe DR, Investigators F (2022) Performance of existing definitions and tests for the diagnosis of invasive aspergillosis in critically ill, non-neutropenic, adult patients: an update including COVID-19 data. J Infect 85(5):573–607.
https://doi.org/10.1016/j.jinf.2022.08.003
")\]. The definitions were then evaluated by the expert panel using the RAND/UCLA appropriateness method \[[26](/article/10.1007/s00134-024-07341-7#ref-CR26 "Brook RH, Chassin MR, Fink A, Solomon DH, Kosecoff J, Park RE (1986) A method for the detailed assessment of the appropriateness of medical technologies. Int J Technol Assess Health Care 2(1):53–63.
https://doi.org/10.1017/s0266462300002774
")\]. Briefly, each member of the expert panel rated each of the proposed definitions from 1 to 9 using the REDCap electronic data capture software (with 1 and 9 indicating “inappropriate” and “fully appropriate” definitions, respectively) \[[27](/article/10.1007/s00134-024-07341-7#ref-CR27 "Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG (2009) Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 42(2):377–381.
https://doi.org/10.1016/j.jbi.2008.08.010
")\]. After all experts had voted, the median score was used to classify each of the rated definitions as follows: (i) inappropriate (score 1–3); (ii) possibly considered (score 4–6); (iii) appropriate (score 7–9). During the rating process, experts were also given the opportunity to provide alternative definitions \[[21](/article/10.1007/s00134-024-07341-7#ref-CR21 "Bassetti M, Scudeller L, Giacobbe DR et al (2019) Developing definitions for invasive fungal diseases in critically ill adult patients in intensive care units. Protocol of the FUNgal infections Definitions in ICU patients (FUNDICU) project. Mycoses 62(4):310–319.
https://doi.org/10.1111/myc.12869
")\]. A total of two voting rounds were necessary to rate initial and alternative definitions. Finally, definitions ranked as “appropriate” or “possibly considered” were discussed by the panel during an online meeting with an anonymized vote for acceptance or rejection. Participants were also offered the possibility to select no preference over agreement or rejection (neutral votes). Consensus was defined as a ≥ 70% agreement towards acceptance with < 15% disagreement (with the denominator also including neutral votes) \[[28](/article/10.1007/s00134-024-07341-7#ref-CR28 "Williamson PR, Altman DG, Blazeby JM et al (2012) Developing core outcome sets for clinical trials: issues to consider. Trials 13:132.
https://doi.org/10.1186/1745-6215-13-132
")\]. A total of three voting rounds preceded by dedicated discussions and modifications were necessary during the online meeting to achieve provisional consensus on all proposed definitions. Then, a fourth round of remote voting of definitions was conducted after peer review to discuss and evaluate reviewers’ comments, even for minor text changes for fluency. The voting round after peer review was performed to consider suggestions provided by referees during the peer-review process without losing the rigorous methodological approach for consensus achievement adopted in the previous phases. Changes were implemented only in case of ≥ 70% agreement towards acceptance with < 15% disagreement. Deviations from the original protocol are reported and justified in the supplementary material.Invasive candidiasis
Background
Invasive candidiasis (IC) is the most common IFD in non-neutropenic, critically ill adult patients in the ICU, and is associated with high mortality that may exceed 50% in patients presenting with septic shock [[2](/article/10.1007/s00134-024-07341-7#ref-CR2 "Bassetti M, Giacobbe DR, Vena A et al (2019) Incidence and outcome of invasive candidiasis in intensive care units (ICUs) in Europe: results of the EUCANDICU project. Crit Care 23(1):219. https://doi.org/10.1186/s13054-019-2497-3
"), [6](/article/10.1007/s00134-024-07341-7#ref-CR6 "Bassetti M, Righi E, Ansaldi F et al (2015) A multicenter multinational study of abdominal candidiasis: epidemiology, outcomes and predictors of mortality. Intensive Care Med 41(9):1601–1610.
https://doi.org/10.1007/s00134-015-3866-2
"), [29](#ref-CR29 "Baldesi O, Bailly S, Ruckly S et al (2017) ICU-acquired candidaemia in France: epidemiology and temporal trends, 2004–2013—a study from the REA-RAISIN network. J Infect 75(1):59–67.
https://doi.org/10.1016/j.jinf.2017.03.011
"),[30](#ref-CR30 "Bassetti M, Righi E, Ansaldi F et al (2014) A multicenter study of septic shock due to candidemia: outcomes and predictors of mortality. Intensive Care Med 40(6):839–845.
https://doi.org/10.1007/s00134-014-3310-z
"),[31](#ref-CR31 "Bassetti M, Vena A, Giacobbe DR et al (2022) Risk factors for intra-abdominal candidiasis in intensive care units: results from EUCANDICU study. Infect Dis Ther 11(2):827–840.
https://doi.org/10.1007/s40121-021-00585-6
"),[32](#ref-CR32 "Bassetti M, Vena A, Meroi M et al (2020) Factors associated with the development of septic shock in patients with candidemia: a post hoc analysis from two prospective cohorts. Crit Care 24(1):117.
https://doi.org/10.1186/s13054-020-2793-y
"),[33](#ref-CR33 "Kett DH, Azoulay E, Echeverria PM, Vincent JL, Extended Prevalence of Infection in ICUSGoI (2011) Candida bloodstream infections in intensive care units: analysis of the extended prevalence of infection in intensive care unit study. Crit Care Med 39(4):665–670.
https://doi.org/10.1097/CCM.0b013e318206c1ca
"),[34](#ref-CR34 "Paiva JA, Pereira JM, Tabah A et al (2016) Characteristics and risk factors for 28-day mortality of hospital acquired fungemias in ICUs: data from the EUROBACT study. Crit Care 20:53.
https://doi.org/10.1186/s13054-016-1229-1
"),[35](#ref-CR35 "Tortorano AM, Dho G, Prigitano A et al (2012) Invasive fungal infections in the intensive care unit: a multicentre, prospective, observational study in Italy (2006–2008). Mycoses 55(1):73–79.
https://doi.org/10.1111/j.1439-0507.2011.02044.x
"),[36](/article/10.1007/s00134-024-07341-7#ref-CR36 "Vincent JL, Rello J, Marshall J et al (2009) International study of the prevalence and outcomes of infection in intensive care units. JAMA 302(21):2323–2329.
https://doi.org/10.1001/jama.2009.1754
")\]. Invasive candidiasis develops when _Candida_ spp., common colonizers of the skin and mucosal surfaces, invade the normally sterile compartments of the body \[[37](/article/10.1007/s00134-024-07341-7#ref-CR37 "Bassetti M, Azoulay E, Kullberg BJ et al (2021) EORTC/MSGERC definitions of invasive fungal diseases: summary of activities of the intensive care unit working group. Clin Infect Dis 72(Suppl 2):S121–S127.
https://doi.org/10.1093/cid/ciaa1751
"), [38](/article/10.1007/s00134-024-07341-7#ref-CR38 "Pappas PG, Lionakis MS, Arendrup MC, Ostrosky-Zeichner L, Kullberg BJ (2018) Invasive candidiasis. Nat Rev Dis Primers 4:18026.
https://doi.org/10.1038/nrdp.2018.26
")\]. IC can be divided into two non-mutually exclusive forms: (_i_) candidemia; (_ii_) deep-seated candidiasis. The most common form of deep-seated candidiasis in non-neutropenic, critically ill patients in the ICU is intra-abdominal candidiasis (IAC) \[[6](/article/10.1007/s00134-024-07341-7#ref-CR6 "Bassetti M, Righi E, Ansaldi F et al (2015) A multicenter multinational study of abdominal candidiasis: epidemiology, outcomes and predictors of mortality. Intensive Care Med 41(9):1601–1610.
https://doi.org/10.1007/s00134-015-3866-2
"), [8](/article/10.1007/s00134-024-07341-7#ref-CR8 "Leroy O, Gangneux JP, Montravers P et al (2009) Epidemiology, management, and risk factors for death of invasive Candida infections in critical care: a multicenter, prospective, observational study in France (2005–2006). Crit Care Med 37(5):1612–1618.
https://doi.org/10.1097/CCM.0b013e31819efac0
"), [31](/article/10.1007/s00134-024-07341-7#ref-CR31 "Bassetti M, Vena A, Giacobbe DR et al (2022) Risk factors for intra-abdominal candidiasis in intensive care units: results from EUCANDICU study. Infect Dis Ther 11(2):827–840.
https://doi.org/10.1007/s40121-021-00585-6
"), [39](/article/10.1007/s00134-024-07341-7#ref-CR39 "Clancy CJ, Nguyen MH (2013) Finding the “missing 50%” of invasive candidiasis: how nonculture diagnostics will improve understanding of disease spectrum and transform patient care. Clin Infect Dis 56(9):1284–1292.
https://doi.org/10.1093/cid/cit006
")\].Development process for invasive candidiasis definitions
Isolation of Candida spp. from at least one blood culture obtained from venipuncture (not from a catheter) is an unequivocal evidence (proven diagnosis) of candidemia, which is the most common form of proven IFD in non-neutropenic, critically ill adult ICU patients [[2](/article/10.1007/s00134-024-07341-7#ref-CR2 "Bassetti M, Giacobbe DR, Vena A et al (2019) Incidence and outcome of invasive candidiasis in intensive care units (ICUs) in Europe: results of the EUCANDICU project. Crit Care 23(1):219. https://doi.org/10.1186/s13054-019-2497-3
"), [8](/article/10.1007/s00134-024-07341-7#ref-CR8 "Leroy O, Gangneux JP, Montravers P et al (2009) Epidemiology, management, and risk factors for death of invasive Candida infections in critical care: a multicenter, prospective, observational study in France (2005–2006). Crit Care Med 37(5):1612–1618.
https://doi.org/10.1097/CCM.0b013e31819efac0
"), [37](/article/10.1007/s00134-024-07341-7#ref-CR37 "Bassetti M, Azoulay E, Kullberg BJ et al (2021) EORTC/MSGERC definitions of invasive fungal diseases: summary of activities of the intensive care unit working group. Clin Infect Dis 72(Suppl 2):S121–S127.
https://doi.org/10.1093/cid/ciaa1751
")\].When a proven diagnosis of IC is not available or difficult to achieve, patients with a high probability of IC can still be included in research studies. To define probable IC for research purposes, the expert panel evaluated (in the presence of consistent clinical criteria) the role of cultures from non-sterile sites and fungal antigen-based biomarkers [[24](/article/10.1007/s00134-024-07341-7#ref-CR24 "Giacobbe DR, Asperges E, Cortegiani A et al (2022) Performance of existing clinical scores and laboratory tests for the diagnosis of invasive candidiasis in critically ill, nonneutropenic, adult patients: a systematic review with qualitative evidence synthesis. Mycoses 65(12):1073–1111. https://doi.org/10.1111/myc.13515
")\]. Regarding fungal antigen-based biomarkers, most of the available evidence in non-neutropenic, critically ill adult patients is limited to the serum biomarker (1,3)-β-D-glucan (BDG). The positive predictive value (PPV) of BDG varies widely between studies, possibly reflecting the prevalence of IC in the study population and its targeted or untargeted use (e.g., the PPV of BDG is expected to be the highest in the subgroup of patients with signs and symptoms of infection and risk factors for IC), but the use of different BDG cut-offs in the different studies \[[24](/article/10.1007/s00134-024-07341-7#ref-CR24 "Giacobbe DR, Asperges E, Cortegiani A et al (2022) Performance of existing clinical scores and laboratory tests for the diagnosis of invasive candidiasis in critically ill, nonneutropenic, adult patients: a systematic review with qualitative evidence synthesis. Mycoses 65(12):1073–1111.
https://doi.org/10.1111/myc.13515
")\] may also influence the results.The panel eventually decided not to develop a “probable” category for research studies on candidemia. This decision was based on the fact that blood cultures are always obtained in patients with suspected candidemia and, if collected properly through venipuncture (two pairs of blood culture bottles of 10 mL each for aerobic and anaerobic culture before initiating any antifungal therapy [[40](/article/10.1007/s00134-024-07341-7#ref-CR40 "Ruhnke M, Bohme A, Buchheidt D et al (2012) Diagnosis of invasive fungal infections in hematology and oncology-guidelines from the Infectious Diseases Working Party in Haematology and Oncology of the German Society for Haematology and Oncology (AGIHO). Ann Oncol 23(4):823–833. https://doi.org/10.1093/annonc/mdr407
")\]), their sensitivity could potentially increase to 70–80% by augmenting the number of blood cultures pairs collected over 24 h \[[39](/article/10.1007/s00134-024-07341-7#ref-CR39 "Clancy CJ, Nguyen MH (2013) Finding the “missing 50%” of invasive candidiasis: how nonculture diagnostics will improve understanding of disease spectrum and transform patient care. Clin Infect Dis 56(9):1284–1292.
https://doi.org/10.1093/cid/cit006
")\]. Therefore, a large number of patients with proven candidemia (or without candidemia if a sufficient number of negative blood cultures have been collected to provide a reliable reference standard) can usually be identified and included in research studies. On the other hand, a plausible argument for developing a definition of probable candidemia is to consider positivity of blood cultures from at least two sites (e.g., from a central venous catheter and from an arterial catheter) when venipuncture is not available. The panel will consider this possibility in future updates of the consensus document, if restriction to proven diagnosis by venipuncture will eventually prove insufficient to achieve adequate sample sizes in research studies.The scenario is different for deep-seated candidiasis, for which a proven diagnosis is usually less frequently obtained than for candidemia, and for which cultures from non-sterile sites and fungal antigen-based biomarkers (in particular serum BDG, to which most of the available evidence refers, see above) could be considered for defining probable IC in research studies. Important limitations to recognize are that the use of fungal antigen-based biomarkers in deep-seated candidiasis is still not standardized and that they could be hampered by low specificity for defining probable IC for research purposes. Furthermore, most evidence on their use in critically ill adult patients comes from studies evaluating candidemia or IC in general (i.e., both candidemia and deep-seated candidiasis) [[24](/article/10.1007/s00134-024-07341-7#ref-CR24 "Giacobbe DR, Asperges E, Cortegiani A et al (2022) Performance of existing clinical scores and laboratory tests for the diagnosis of invasive candidiasis in critically ill, nonneutropenic, adult patients: a systematic review with qualitative evidence synthesis. Mycoses 65(12):1073–1111. https://doi.org/10.1111/myc.13515
")\]. After careful consideration and discussion, the panel ultimately agreed that serum BDG positivity may not achieve sufficient specificity in the target population as a mycological criterion to be used in conjunction with at least one clinical criterion to define “probable” deep-seated candidiasis in research studies. Implementation of serum BDG as a mycological criterion was the most debated topic during consensus development. It was initially included in the provisional definition, although, while the panel almost unanimously agreed on the other mycological criteria, major comments regarding serum BDG inclusion highlighted its possible low specificity for defining probable deep-seated candidiasis for research purposes. Discussions were protracted after peer review, when it was eventually agreed not to include serum BDG as mycological criterion for the current FUNDICU research definition for probable deep-seated candidiasis, at least pending further evidence.An even more difficult task is to define IC when its presence is suspected clinically but the criteria for either proven or probable IC are not fulfilled. The expert panel considered once again (as for the use of antigen-based biomarkers for probable deep-seated candidiasis, see above) that a crucial aspect in developing research definitions is the conceptual distinction between clinical suspicion of IC (which may lead to early therapy in the daily clinical practice) and the definition of IC intended for research purposes. Specifically, a low but non-negligible probability of IC may prompt empirical antifungal therapy in patients with severe clinical presentation (i.e., septic shock) in clinical practice, but may not be sufficient to ensure homogeneity and control for confounding when defining IC for research purposes. For this reason, the panel ultimately decided not to develop a “possible” category for the definition of IC. Indeed, according to the results of the baseline systematic review conducted to support the development of this document [[24](/article/10.1007/s00134-024-07341-7#ref-CR24 "Giacobbe DR, Asperges E, Cortegiani A et al (2022) Performance of existing clinical scores and laboratory tests for the diagnosis of invasive candidiasis in critically ill, nonneutropenic, adult patients: a systematic review with qualitative evidence synthesis. Mycoses 65(12):1073–1111. https://doi.org/10.1111/myc.13515
")\], the definition of a “possible IC” category would have carried an unacceptable risk of including a large proportion of patients without IC, thereby precluding reliable comparison and generalization of research results.Definitions of proven invasive candidiasis and probable deep-seated candidiasis
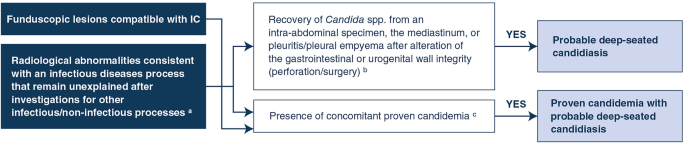
The developed definitions of proven IC and probable deep-seated candidiasis in non-neutropenic, critically ill adult ICU patients without classical host factors for IFD are detailed in Tables 1 and 2, respectively. A flowchart to identify patients fulfilling the definition of probable deep-seated candidiasis is also displayed in Fig. 1.
Table 1 Research definition for proven invasive candidiasis in non-neutropenic, adult patients in ICU
Table 2 Research definition for probable deep-seated candidiasis in non-neutropenic, adult patients in ICU
Fig. 1
The alternative text for this image may have been generated using AI.
Flowchart for probable deep-seated candidiasis research definition in non-neutropenic, adult patients in ICU. The definitions of probable IC provided in the present document do not apply to those ICU patients fulfilling host factors as defined in the European Organization for Research and Treatment of Cancer (EORTC) and the Mycoses Study Group Education and Research Consortium (MSGERC) consensus: (i) hematology and solid organ transplantation patients; (ii) prolonged use of corticosteroids; (iii) treatment with other recognized T-cell immunosuppressants; (iv) treatment with recognized B-cell immunosuppressants; (v) inherited severe immunodeficiency; (vi) acute graft-versus-host disease grade III or IV involving the gut, lungs, or liver that is refractory to first-line treatment with steroids. In these patients, the EORTC/MSGERC definitions should be used for defining IC in research studies (for more details, see the EORTC/MSGERC consensus document [[20](/article/10.1007/s00134-024-07341-7#ref-CR20 "Donnelly JP, Chen SC, Kauffman CA et al (2020) Revision and update of the consensus definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis 71(6):1367–1376. https://doi.org/10.1093/cid/ciz1008
")\]). aSuch abnormalities should be evident in deep sites where invasive candidiasis may develop either because of direct inoculation or because of previous, undetected hematogenous spread (e.g., IAC, endocarditis, osteomyelitis, arthritis, mediastinitis, meningitis; with the exclusion of the lung, for which only a proven diagnosis through histology would be considered as invasive candidiasis). The investigations carried out for excluding alternative diagnoses should be reported in detail. b Specimens should be obtained during surgery, puncture, or obtained from a newly inserted drain as soon as possible (no later than 24 h after placement). This mycological criterion does not apply to the isolation of _Candida_ spp. from peritoneal fluid after gastrointestinal/urogenital perforation if complete source control is rapidly obtained (within 24 h from perforation and after peritoneal fluid collection). This may reflect contamination before development of invasive disease and does not define a mycological criterion for probable deep-seated candidiasis. In case of source control performed > 24 h after perforation or in case of recurrent peritonitis (e.g., anastomosis leakage), isolation of _Candida_ spp. from the peritoneum (from an intra-abdominal specimen during surgery or obtained from an external drainage inserted from < 24 h) does define a mycological criterion for probable deep-seated candidiasis. The same concepts apply to Candida mediastinitis and pleuritis/pleural empyema after esophageal perforation. c The presence of concomitant proven candidemia can be considered as a mycological criterion for probable deep-seated candidiasis. In this case, the disease should be classified as proven IC in research studies (proven candidemia plus probable deep-seated candidiasis). _IC_ invasive candidiasis, _ICU_ intensive care unitProven invasive candidiasis
The expert panel universally agreed that the identification of Candida spp. from normally sterile sites defines IC (either candidemia or deep-seated candidiasis). Identification can be made by direct microscopy, culture, or histology. The histological evidence of budding cells consistent with Candida spp. directly defines proven invasive candidiasis, whereas species identification by polymerase chain reaction (PCR) or culture is required for hyphae or pseudohyphae, which may also be observed with other yeasts [[37](/article/10.1007/s00134-024-07341-7#ref-CR37 "Bassetti M, Azoulay E, Kullberg BJ et al (2021) EORTC/MSGERC definitions of invasive fungal diseases: summary of activities of the intensive care unit working group. Clin Infect Dis 72(Suppl 2):S121–S127. https://doi.org/10.1093/cid/ciaa1751
")\].Probable deep-seated candidiasis
The presence of at least one mycological criterion and at least one clinical criterion is necessary for defining probable deep-seated candidiasis, as agreed upon by the panel. Two mycological criteria were eventually defined. The first one is recovery of Candida spp. from a specimen collected in a sterile manner from an abdominal, mediastinal, or pleural space or abscess/empyema after alteration of the gastrointestinal or urogenital wall integrity (perforation/surgery). Specimens should preferably be obtained during surgery or from a ultrasound (US)-guided or computerized tomography (CT)-guided aspirate or from a newly inserted drain no later than 24 h after placement [[41](/article/10.1007/s00134-024-07341-7#ref-CR41 "De Waele JJ, Boelens J, Van De Putte D, Huis In ’t Veld D, Coenye T (2022) The role of abdominal drain cultures in managing abdominal infections. Antibiotics (Basel). 11(5):97. https://doi.org/10.3390/antibiotics11050697
")\]. However, contamination of specimens obtained from colonized drains should always be considered. In particular, this mycological criterion does not apply to the isolation of _Candida_ spp. from peritoneal fluid after gastrointestinal or urogenital perforation if source control is rapidly achieved (within 24 h from perforation and after peritoneal fluid collection). A similar situation may reflect contamination prior to the development of invasive disease. In the case of source control performed more than 24 h after perforation or in the case of recurrent peritonitis (e.g., anastomotic leakage), isolation of _Candida_ spp. from the peritoneum (from an intra-abdominal specimen during surgery or obtained from an external drainage inserted within 24 h) defines a mycological criterion for probable deep-seated candidiasis. The same concepts apply to _Candida_ mediastinitis and pleuritis/empyema following esophageal perforation. The second mycological criterion is as follows: for other deep sites (and for the mediastinum and the abdomen in the absence of perforation), the presence of concomitant proven candidemia can be considered as a mycological criterion for probable deep-seated candidiasis. In this latter case, the disease should be classified as proven IC in research studies (proven candidemia plus probable deep-seated candidiasis).Regarding clinical criteria, the following were defined: (i) funduscopic lesions compatible with invasive candidiasis or (ii) radiological abnormalities consistent with an infectious disease process that remain unexplained after investigation for other infectious/non-infectious processes; these abnormalities should be present in sites where IC could develop either because of direct inoculation or because of previous unrecognized hematogenous spread (e.g., IAC, endocarditis, osteomyelitis, arthritis, mediastinitis, meningitis); very importantly, the investigations undertaken for excluding alternative diagnoses should be reported in detail in all research studies in which the probable deep-seated candidiasis definition is employed.
Of note, the systematic reviews that underpinned the development of this document highlighted that very few studies investigating the performance of PCR (including assays exploiting miniaturized magnetic resonance technology) for the diagnosis of IC on blood cultures or other deep specimens met the inclusion criteria necessary to reliably assess the role of PCR in defining IC in non-neutropenic, critically ill adult ICU patients without classical host factors for IFD. The same applies to fungal antigen-based biomarkers other than BDG and to combinations of biomarkers. Nevertheless, the panel strongly recognizes that both PCR and fungal antigen-based tests (including further investigation on BDG in the target population) represent an important area of future research in an attempt to improve current IC diagnosis for both research and clinical purposes in the target population.
Invasive aspergillosis
Background
Invasive aspergillosis (IA) has traditionally been reported in classical at-risk populations, such as hematology or SOT patients [[20](/article/10.1007/s00134-024-07341-7#ref-CR20 "Donnelly JP, Chen SC, Kauffman CA et al (2020) Revision and update of the consensus definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis 71(6):1367–1376. https://doi.org/10.1093/cid/ciz1008
"), [42](/article/10.1007/s00134-024-07341-7#ref-CR42 "Husain S, Mooney ML, Danziger-Isakov L et al (2011) A 2010 working formulation for the standardization of definitions of infections in cardiothoracic transplant recipients. J Heart Lung Transplant 30(4):361–374.
https://doi.org/10.1016/j.healun.2011.01.701
"), [43](/article/10.1007/s00134-024-07341-7#ref-CR43 "Maschmeyer G, Haas A, Cornely OA (2007) Invasive aspergillosis: epidemiology, diagnosis and management in immunocompromised patients. Drugs 67(11):1567–1601.
https://doi.org/10.2165/00003495-200767110-00004
")\]. However, IA can also develop outside these classical categories. In non-neutropenic, adult ICU patients, IA usually presents as invasive pulmonary aspergillosis (IPA), which poses particular diagnostic challenges: (i) the classical radiological features of IPA (e.g., halo or air crescent sign) described in immunocompromised patients are often absent; (ii) non-culture-based tests such as galactomannan and DNA amplification may have lower diagnostic accuracy than in classical at-risk populations \[[1](/article/10.1007/s00134-024-07341-7#ref-CR1 "Bassetti M, Bouza E (2017) Invasive mould infections in the ICU setting: complexities and solutions. J Antimicrob Chemother 72(supp_l 1):39–47.
https://doi.org/10.1093/jac/dkx032
"), [22](/article/10.1007/s00134-024-07341-7#ref-CR22 "Bassetti M, Giacobbe DR, Grecchi C et al (2020) Performance of existing definitions and tests for the diagnosis of invasive aspergillosis in critically ill, adult patients: a systematic review with qualitative evidence synthesis. J Infect 81(1):131–146.
https://doi.org/10.1016/j.jinf.2020.03.065
"), [44](#ref-CR44 "Baddley JW, Stephens JM, Ji X, Gao X, Schlamm HT, Tarallo M (2013) Aspergillosis in intensive care unit (ICU) patients: epidemiology and economic outcomes. BMC Infect Dis 13:29.
https://doi.org/10.1186/1471-2334-13-29
"),[45](#ref-CR45 "Meersseman W, Vandecasteele SJ, Wilmer A, Verbeken E, Peetermans WE, Van Wijngaerden E (2004) Invasive aspergillosis in critically ill patients without malignancy. Am J Respir Crit Care Med 170(6):621–625.
https://doi.org/10.1164/rccm.200401-093OC
"),[46](#ref-CR46 "Prattes J, Wauters J, Giacobbe DR, Lagrou K, Hoenigl M, Group E-CS (2021) Diagnosis and treatment of COVID-19 associated pulmonary apergillosis in critically ill patients: results from a European confederation of medical mycology registry. Intensive Care Med 47(10):1158–1160.
https://doi.org/10.1007/s00134-021-06471-6
"),[47](#ref-CR47 "van de Veerdonk FL, Kolwijck E, Lestrade PP et al (2017) Influenza-associated aspergillosis in critically ill patients. Am J Respir Crit Care Med 196(4):524–527.
https://doi.org/10.1164/rccm.201612-2540LE
"),[48](#ref-CR48 "Bartoletti M, Pascale R, Cricca M et al (2021) Epidemiology of invasive pulmonary aspergillosis among intubated patients with COVID-19: a prospective study. Clin Infect Dis 73(11):e3606–e3614.
https://doi.org/10.1093/cid/ciaa1065
"),[49](#ref-CR49 "Borman AM, Palmer MD, Fraser M et al (2020) COVID-19-associated invasive aspergillosis: data from the UK National Mycology Reference Laboratory. J Clin Microbiol.
https://doi.org/10.1128/JCM.02136-20
"),[50](#ref-CR50 "Lahmer T, Kriescher S, Herner A et al (2021) Invasive pulmonary aspergillosis in critically ill patients with severe COVID-19 pneumonia: results from the prospective AspCOVID-19 study. PLoS ONE 16(3):e0238825.
https://doi.org/10.1371/journal.pone.0238825
"),[51](#ref-CR51 "Nyga R, Maizel J, Nseir S et al (2020) Invasive tracheobronchial aspergillosis in critically ill patients with severe influenza. A clinical trial. Am J Respir Crit Care Med 202(5):708–716.
https://doi.org/10.1164/rccm.201910-1931OC
"),[52](#ref-CR52 "Permpalung N, Chiang TP, Massie AB et al (2022) Coronavirus disease 2019-associated pulmonary aspergillosis in mechanically ventilated patients. Clin Infect Dis 74(1):83–91.
https://doi.org/10.1093/cid/ciab223
"),[53](/article/10.1007/s00134-024-07341-7#ref-CR53 "van de Veerdonk FL, Wauters J, Verweij PE (2020) Invasive aspergillus tracheobronchitis emerging as a highly lethal complication of severe influenza. Am J Respir Crit Care Med 202(5):646–648.
https://doi.org/10.1164/rccm.202005-1883ED
")\]. These problems could be overcome by proven diagnosis requiring histology. However, obtaining samples for histology by biopsy of infected tissue is often not feasible, e.g., due to hemodynamic instability, mechanical ventilation, or coagulopathy. For this reason, various definitions of probable IA for use in critically ill ICU patients have been proposed over the years \[[14](#ref-CR14 "Blot SI, Taccone FS, Van den Abeele AM et al (2012) A clinical algorithm to diagnose invasive pulmonary aspergillosis in critically ill patients. Am J Respir Crit Care Med 186(1):56–64.
https://doi.org/10.1164/rccm.201111-1978OC
"),[15](#ref-CR15 "Bulpa P, Dive A, Sibille Y (2007) Invasive pulmonary aspergillosis in patients with chronic obstructive pulmonary disease. Eur Respir J 30(4):782–800.
https://doi.org/10.1183/09031936.00062206
"),[16](#ref-CR16 "Koehler P, Bassetti M, Chakrabarti A et al (2021) Defining and managing COVID-19-associated pulmonary Aspergillosis: the 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect Dis 21(6):e149–e162.
https://doi.org/10.1016/S1473-3099(20)30847-1
"),[17](#ref-CR17 "Vandewoude KH, Blot SI, Depuydt P et al (2006) Clinical relevance of Aspergillus isolation from respiratory tract samples in critically ill patients. Crit Care 10(1):R31.
https://doi.org/10.1186/cc4823
"),[18](#ref-CR18 "Verweij PE, Bruggemann RJM, Azoulay E et al (2021) Taskforce report on the diagnosis and clinical management of COVID-19 associated pulmonary aspergillosis. Intensive Care Med 47(8):819–834.
https://doi.org/10.1007/s00134-021-06449-4
"),[19](/article/10.1007/s00134-024-07341-7#ref-CR19 "Verweij PE, Rijnders BJA, Bruggemann RJM et al (2020) Review of influenza-associated pulmonary aspergillosis in ICU patients and proposal for a case definition: an expert opinion. Intensive Care Med 46(8):1524–1535.
https://doi.org/10.1007/s00134-020-06091-6
")\]. However, although they are certainly useful, they are not based on a broad consensus and/or are limited to very specific categories of ICU patients, which precludes their generalization. Another diagnostic challenge is that distinguishing _Aspergillus_ colonization from IA in non-neutropenic, adult patients in ICU may be more difficult in the absence of classical host factors.Development process for invasive aspergillosis definitions
The non-specific clinical/radiological presentation and the wide heterogeneity of predisposing conditions remain important issues when attempting to develop a universal definition of IA in non-neutropenic adult ICU patients without classical host factors. The results of the systematic review conducted to support the development of the present document resulted in the identification of common features in the performance of existing definitions and laboratory tests, which ultimately helped to achieve consensus [[22](/article/10.1007/s00134-024-07341-7#ref-CR22 "Bassetti M, Giacobbe DR, Grecchi C et al (2020) Performance of existing definitions and tests for the diagnosis of invasive aspergillosis in critically ill, adult patients: a systematic review with qualitative evidence synthesis. J Infect 81(1):131–146. https://doi.org/10.1016/j.jinf.2020.03.065
"), [25](/article/10.1007/s00134-024-07341-7#ref-CR25 "Bassetti M, Zuccaro V, Asperges E, Scudeller L, Giacobbe DR, Investigators F (2022) Performance of existing definitions and tests for the diagnosis of invasive aspergillosis in critically ill, non-neutropenic, adult patients: an update including COVID-19 data. J Infect 85(5):573–607.
https://doi.org/10.1016/j.jinf.2022.08.003
")\]. Specifically, (i) although based on small samples, the existing AspICU definition of putative IPA showed a good ability to discriminate between colonization and infection in critically ill patients with positive respiratory cultures, when tested against the proper diagnostic reference (autopsy/histology); (ii) the diagnostic performance of bronchoalveolar lavage fluid (BALF) galactomannan was better than that of serum galactomannan in the target population; (iii) BALF and serum BDG consistently showed suboptimal specificity for the diagnosis of IPA in non-neutropenic, adult ICU patients \[[22](/article/10.1007/s00134-024-07341-7#ref-CR22 "Bassetti M, Giacobbe DR, Grecchi C et al (2020) Performance of existing definitions and tests for the diagnosis of invasive aspergillosis in critically ill, adult patients: a systematic review with qualitative evidence synthesis. J Infect 81(1):131–146.
https://doi.org/10.1016/j.jinf.2020.03.065
"), [25](/article/10.1007/s00134-024-07341-7#ref-CR25 "Bassetti M, Zuccaro V, Asperges E, Scudeller L, Giacobbe DR, Investigators F (2022) Performance of existing definitions and tests for the diagnosis of invasive aspergillosis in critically ill, non-neutropenic, adult patients: an update including COVID-19 data. J Infect 85(5):573–607.
https://doi.org/10.1016/j.jinf.2022.08.003
")\]. With this baseline information, and after sharing opinions and experiences related to the application of concepts developed for other patient populations, the expert panel was finally able to reach a consensus on the definitions of proven IA and probable IPA/tracheobronchial aspergillosis (TBA) in non-neutropenic, critically ill adult ICU patients without classical host factors. The panel decided against developing a “possible” category of IA for research purposes. Yet, it did not discourage the use of the possible definition developed elsewhere for specific ICU populations (e.g., patients with COVID-19-associated pulmonary aspergillosis \[CAPA\]) to target early antifungal treatment in selected situations in clinical practice \[[16](/article/10.1007/s00134-024-07341-7#ref-CR16 "Koehler P, Bassetti M, Chakrabarti A et al (2021) Defining and managing COVID-19-associated pulmonary Aspergillosis: the 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect Dis 21(6):e149–e162.
https://doi.org/10.1016/S1473-3099(20)30847-1
"), [18](/article/10.1007/s00134-024-07341-7#ref-CR18 "Verweij PE, Bruggemann RJM, Azoulay E et al (2021) Taskforce report on the diagnosis and clinical management of COVID-19 associated pulmonary aspergillosis. Intensive Care Med 47(8):819–834.
https://doi.org/10.1007/s00134-021-06449-4
")\].Three important points need to be discussed more in detail. First, while the definition of proven IA is inherently applicable to all forms of IA (not only pulmonary), the evidence that led to the development of the definition of probable IA in the current document was limited to IPA and TBA. Therefore, the panel did not consider it feasible to define probable IA for forms other than IPA and TBA, pending further evidence. Second, as anticipated above, the panel did not support to develop a definition of possible IPA/TBA for research purposes. In clinical practice, physicians may decide to administer antifungals in selected cases of suspected IPA/TBA that do not meet the definition for probable disease (e.g., critically ill patients with influenza or COVID-19 who have no alternative diagnoses, have positive mycological tests from non-bronchoscopic lavage, and do not respond to antibacterial therapy for pulmonary infiltrates) [[19](/article/10.1007/s00134-024-07341-7#ref-CR19 "Verweij PE, Rijnders BJA, Bruggemann RJM et al (2020) Review of influenza-associated pulmonary aspergillosis in ICU patients and proposal for a case definition: an expert opinion. Intensive Care Med 46(8):1524–1535. https://doi.org/10.1007/s00134-020-06091-6
"), [54](/article/10.1007/s00134-024-07341-7#ref-CR54 "Ergun M, Bruggemann RJM, Alanio A et al (2021) Aspergillus test profiles and mortality in critically ill COVID-19 patients. J Clin Microbiol 59(12):e0122921.
https://doi.org/10.1128/JCM.01229-21
"), [55](/article/10.1007/s00134-024-07341-7#ref-CR55 "Giacobbe DR, Prattes J, Wauters J et al (2022) Prognostic impact of bronchoalveolar lavage fluid galactomannan and aspergillus culture results on survival in COVID-19 intensive care unit patients: a post hoc analysis from the European Confederation of Medical Mycology (ECMM) COVID-19-associated pulmonary aspergillosis study. J Clin Microbiol 60(4):e0229821.
https://doi.org/10.1128/jcm.02298-21
")\]. However, the number of false-positive tests in a possible category would be too high to avoid confounding the results of research studies, thereby compromising comparability and generalizability. Third, the presence of signs and symptoms defined in the AspICU criteria was considered by the panel as a necessary condition to evaluate patients for probable IPA/TBA (with very few exceptions, see below), to improve the chance of distinguishing true infection from colonization \[[14](/article/10.1007/s00134-024-07341-7#ref-CR14 "Blot SI, Taccone FS, Van den Abeele AM et al (2012) A clinical algorithm to diagnose invasive pulmonary aspergillosis in critically ill patients. Am J Respir Crit Care Med 186(1):56–64.
https://doi.org/10.1164/rccm.201111-1978OC
")\].The definitions of probable IPA and probable TBA required prolonged discussions. While generic risk factors (e.g., short courses of corticosteroids) may prompt clinicians to consider antifungal therapy in selected cases, they are too vague to contribute defining probable IPA and probable TBA for research purposes. Rather than risk factors, the panel decided to define precise predisposing conditions, i.e., baseline conditions that carry a substantial risk of IA (eventually defined as ICU host factors). Surely, this could be seen as a conservative approach. However, it makes it possible to preserve comparability and generalization of research results without necessarily impacting on clinical practice (since physicians should follow guidelines for patient management rather than research definitions for early treatment decisions).
Definitions of proven invasive aspergillosis and probable invasive pulmonary aspergillosis/probable tracheobronchial aspergillosis
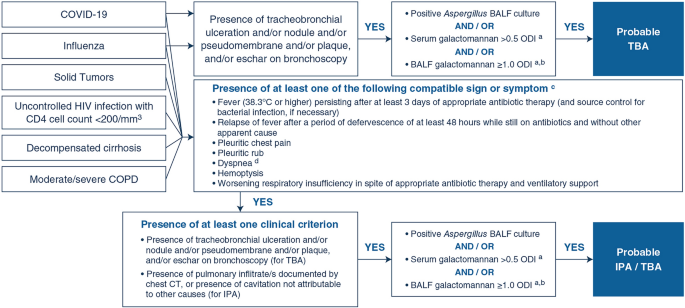
The definitions of proven IA and of probable IPA and probable TBA in non-neutropenic, critically ill adult ICU patients without classical host factors for IFD are detailed in Table 3 and Table 4, respectively. A flowchart to identify patients fulfilling the definition of probable IPA/probable TBA is also displayed in Fig. 2.
Table 3 Research definition for proven invasive aspergillosis in non-neutropenic, adult patients in ICU
Table 4 Research definitions for probable invasive pulmonary aspergillosis and tracheobronchial aspergillosis in non-neutropenic, adult patients in ICU
Fig. 2
The alternative text for this image may have been generated using AI.
Flowchart for probable IPA and probable TBA research definitions in non-neutropenic, adult patients in ICU*. BALF bronchoalveolar lavage fluid, COPD chronic obstructive pulmonary disease, COVID-19 coronavirus disease 2019, CT computerized tomography, GM galactomannan, HIV human immunodeficiency virus, ICU intensive care unit, IPA invasive pulmonary aspergillosis, ODI optical density index, TBA tracheobronchial aspergillosis. *The definitions of probable IPA/TBA for research studies provided in the present document do not apply to those ICU patients fulfilling host factors as defined in the EORTC/MSGERC consensus: (i) hematology and solid organ transplant patients; (ii) prolonged use of corticosteroids; (iii) treatment with other recognized T-cell immunosuppressants; (iv) treatment with recognized B-cell immunosuppressants; (v) inherited severe immunodeficiency; (vi) acute graft-versus-host disease grade III or IV involving the gut, lungs, or liver that is refractory to first-line treatment with steroids. In these patients, the EORTC/MSGERC definitions should be used for defining IPA/TBA in research studies (for more details, see the EORTC/MSGERC consensus document [[20](/article/10.1007/s00134-024-07341-7#ref-CR20 "Donnelly JP, Chen SC, Kauffman CA et al (2020) Revision and update of the consensus definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis 71(6):1367–1376. https://doi.org/10.1093/cid/ciz1008
")\]). aPlatelia _Aspergillus_ Ag Kit. bWhen the Platelia test is unavailable, another GM test can be used when this test was compared with the Platelia test in a well-designed study and shown to have comparable specificity to the 1.0 Platelia cut-off. cCompatible with the site/progression of IPA or TBA. dNot applicable for patients ventilated patients from more than 48 h at the time of assessment for probable IPA/TBA. TBA; applicable in the first 48 h if dyspneic at the time of initiation of ventilationProven invasive aspergillosis
The expert panel agreed to define proven IA in non-neutropenic, critically ill adult ICU patients without classical host factors as the combination of Aspergillus detection and tissue invasion. More in detail, proven IA is defined by the presence of tissue invasion demonstrated by histological or cytopathological evidence in a specimen obtained from a normally sterile site or the lung by biopsy or needle aspiration, combined with detection of hyphae compatible with Aspergillus spp. (confirmed by culture or PCR). Alternatively, the recovery from culture of Aspergillus spp. from a specimen obtained by biopsy or needle aspiration from a lesion consistent with an infectious process and obtained from a normally sterile site is also defined as proven IA.
Probable invasive pulmonary aspergillosis and probable tracheobronchial aspergillosis
To define probable IPA/TBA, the following should be present: (i) at least one compatible sign or symptom; (ii) at least one ICU host factor; (iii) at least one clinical criterion; (iv) at least one mycological criterion. The only allowed exception is probable TBA in patients with COVID-19 or influenza that can be defined also in the absence of compatible signs and symptoms (see Table 4 and Fig. 2).
Regarding compatible signs and symptoms, at least one of the following signs or symptoms should be present (and compatible with the site/progression of IPA or TBA) to proceed with the evaluation of the patients who may meet the definitions of probable IPA or probable TBA for research studies: (i) fever persisting after at least 3 days of appropriate antibiotic therapy (and source control for bacterial infection, if necessary); (ii) relapse of fever after a period of at least 48 h of defervescence while still on antibiotics and without other apparent causes; (iii) pleuritic chest pain; (iv) pleuritic rubbing of the lungs on examination; (v) dyspnea (not applicable for patients ventilated from more than 48 h at the time of assessment for probable IPA/TBA, and applicable in the first 48 h if dyspneic at the time of initiation of ventilation); (vi) hemoptysis; (vii) worsening respiratory insufficiency despite appropriate antibiotic therapy and ventilatory support [[14](/article/10.1007/s00134-024-07341-7#ref-CR14 "Blot SI, Taccone FS, Van den Abeele AM et al (2012) A clinical algorithm to diagnose invasive pulmonary aspergillosis in critically ill patients. Am J Respir Crit Care Med 186(1):56–64. https://doi.org/10.1164/rccm.201111-1978OC
")\].ICU host factors include the following: (i) influenza; (ii) COVID-19; (iii) moderate/severe COPD; (iv) decompensated liver cirrhosis; (v) Uncontrolled infection by human immunodeficiency virus (HIV) with CD4 cell count < 200/mm3; (vi) solid tumors. The expert panel recognize the usefulness of existing consensus definitions for specific categories of ICU patients (i.e., patients with influenza or with COVID-19) as valuable baseline information for development of this document [[16](/article/10.1007/s00134-024-07341-7#ref-CR16 "Koehler P, Bassetti M, Chakrabarti A et al (2021) Defining and managing COVID-19-associated pulmonary Aspergillosis: the 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect Dis 21(6):e149–e162. https://doi.org/10.1016/S1473-3099(20)30847-1
"), [19](/article/10.1007/s00134-024-07341-7#ref-CR19 "Verweij PE, Rijnders BJA, Bruggemann RJM et al (2020) Review of influenza-associated pulmonary aspergillosis in ICU patients and proposal for a case definition: an expert opinion. Intensive Care Med 46(8):1524–1535.
https://doi.org/10.1007/s00134-020-06091-6
")\].Clinical criteria include the following: (i) presence of tracheobronchial ulceration and/or nodules and/or pseudomembrane and/or plaque, and/or eschar on bronchoscopy (to define probable TBA); (ii) presence of pulmonary infiltrate(s) by chest CT, or presence of cavitation not attributable to other causes (to define probable IPA).
With regard to the mycological criteria, the panel agreed on the following: (i) detection of mold elements in BALF by microscopy; (ii) positive Aspergillus BALF culture; (iii) serum galactomannan > 0.5 optical density index (ODI); (iv) BALF galactomannan ≥ 1.0 ODI. With regard to Aspergillus PCR, while its use in BALF, serum, plasma, and/or whole blood could be useful in clinical practice to identify patients with suspected IPA/TBA and could prompt early treatment (as such it is included in the clinical consensus definition for probable CAPA developed by the ECMM and the International Society for Human and Animal Mycology [ISHAM] [[16](/article/10.1007/s00134-024-07341-7#ref-CR16 "Koehler P, Bassetti M, Chakrabarti A et al (2021) Defining and managing COVID-19-associated pulmonary Aspergillosis: the 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect Dis 21(6):e149–e162. https://doi.org/10.1016/S1473-3099(20)30847-1
")\]), the overall evidence regarding its general performance in non-neutropenic, critically ill ICU patients is still limited \[[22](/article/10.1007/s00134-024-07341-7#ref-CR22 "Bassetti M, Giacobbe DR, Grecchi C et al (2020) Performance of existing definitions and tests for the diagnosis of invasive aspergillosis in critically ill, adult patients: a systematic review with qualitative evidence synthesis. J Infect 81(1):131–146.
https://doi.org/10.1016/j.jinf.2020.03.065
"), [25](/article/10.1007/s00134-024-07341-7#ref-CR25 "Bassetti M, Zuccaro V, Asperges E, Scudeller L, Giacobbe DR, Investigators F (2022) Performance of existing definitions and tests for the diagnosis of invasive aspergillosis in critically ill, non-neutropenic, adult patients: an update including COVID-19 data. J Infect 85(5):573–607.
https://doi.org/10.1016/j.jinf.2022.08.003
")\]. Therefore, additional studies conducted in the target population may lead to the inclusion of PCR for the diagnosis of IA in future updates of the current definitions. In particular, this should not discourage the use of PCR as a mycological criterion in research studies conducted in patients with COVID-19 using the ECMM/ISHAM definition of probable CAPA as a reference standard, as this may provide indirect evidence of the suitability of PCR as a useful mycological criterion (e.g., indirect evidence arising from prognostic considerations). The same considerations generally apply to the _Aspergillus_ lateral flow device (AspLFD) and the GM lateral flow assay galactomannan lateral flow assay (GM-LFA) \[[16](/article/10.1007/s00134-024-07341-7#ref-CR16 "Koehler P, Bassetti M, Chakrabarti A et al (2021) Defining and managing COVID-19-associated pulmonary Aspergillosis: the 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect Dis 21(6):e149–e162.
https://doi.org/10.1016/S1473-3099(20)30847-1
")\]. The latest update of the systematic review on the diagnostic performance of laboratory tests for IPA provided some evidence on the use of BALF GM-LFA in the population of interest \[[25](/article/10.1007/s00134-024-07341-7#ref-CR25 "Bassetti M, Zuccaro V, Asperges E, Scudeller L, Giacobbe DR, Investigators F (2022) Performance of existing definitions and tests for the diagnosis of invasive aspergillosis in critically ill, non-neutropenic, adult patients: an update including COVID-19 data. J Infect 85(5):573–607.
https://doi.org/10.1016/j.jinf.2022.08.003
")\]. Although the sensitivity and specificity varied between studies, the panel eventually deemed it appropriate, when the Platelia test is unavailable, to suggest using other GM tests for defining probable IPA/TBA in research studies, provided they were compared with the Platelia test in well-designed studies and shown to have comparable specificity to the 1.0 Platelia cut-off. Overall, whenever available, the use of GM remains preferable for defining probable IPA/TBA in research studies in the population of interest, pending further evidence.Other invasive fungal diseases
Definition development process
For IFD other than IC and IA, such as Pneumocystis jirovecii pneumonia (PJP), the systematic reviews supporting the development of this document highlighted the lack of sufficient evidence on the diagnostic performance of existing definitions and laboratory tests for their diagnosis in non-neutropenic, critically ill adult patients in the ICU [[23](/article/10.1007/s00134-024-07341-7#ref-CR23 "Giacobbe DR, Cortegiani A, Karaiskos I et al (2021) Performance of existing definitions and tests for the diagnosis of invasive fungal diseases other than invasive candidiasis and invasive aspergillosis in critically ill, adult patients: a systematic review with qualitative evidence synthesis. J Fungi (Basel, Switzerland) 7(3):176. https://doi.org/10.3390/jof7030176
")\]. While for proven IFD other than IA and IC, the expert panel suggested adhering to the definitions already provided in the EORTC/MSGERC consensus document \[[20](/article/10.1007/s00134-024-07341-7#ref-CR20 "Donnelly JP, Chen SC, Kauffman CA et al (2020) Revision and update of the consensus definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis 71(6):1367–1376.
https://doi.org/10.1093/cid/ciz1008
")\], defining a probable category for these IFD was considered unfeasible in the population of interest. For this reason, dedicated initiatives have been started to assess the use and performance of diagnostic tests for IFD other than IC and IA in ICU patients \[[56](/article/10.1007/s00134-024-07341-7#ref-CR56 "Di Meco G, Mora S, Giacobbe DR et al (2022) A wide database for a multicenter study on Pneumocystis jirovecii pneumonia in intensive care units. Stud Health Technol Inform 294:557–558.
https://doi.org/10.3233/SHTI220521
"), [57](/article/10.1007/s00134-024-07341-7#ref-CR57 "Giacobbe DR, Dettori S, Di Pilato V et al (2023) Pneumocystis jirovecii pneumonia in intensive care units: a multicenter study by ESGCIP and EFISG. Crit Care 27(1):323.
https://doi.org/10.1186/s13054-023-04608-1
")\], aimed to support the development of definitions of probable disease in future updates of this document.Conclusions
The FUNDICU consensus document provides definitions for IC and IA in non-neutropenic, adult patients in the ICU who do not fulfil the host factors included in the recent EORTC/MSGERC consensus document [[20](/article/10.1007/s00134-024-07341-7#ref-CR20 "Donnelly JP, Chen SC, Kauffman CA et al (2020) Revision and update of the consensus definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis 71(6):1367–1376. https://doi.org/10.1093/cid/ciz1008
")\], for use in clinical research. Although many gaps remain, we hope that, if widely adopted, the standardized definitions provided in this document will facilitate the design of future research studies and increase the comparability of their results. The ultimate goal is to standardize the diagnosis of IFD and optimize the management and outcomes of critically ill patients with IFD.Data availability
Not applicable.
References
- Bassetti M, Bouza E (2017) Invasive mould infections in the ICU setting: complexities and solutions. J Antimicrob Chemother 72(supp_l 1):39–47. https://doi.org/10.1093/jac/dkx032
Article CAS Google Scholar - Bassetti M, Giacobbe DR, Vena A et al (2019) Incidence and outcome of invasive candidiasis in intensive care units (ICUs) in Europe: results of the EUCANDICU project. Crit Care 23(1):219. https://doi.org/10.1186/s13054-019-2497-3
Article PubMed PubMed Central Google Scholar - Delaloye J, Calandra T (2014) Invasive candidiasis as a cause of sepsis in the critically ill patient. Virulence 5(1):161–169. https://doi.org/10.4161/viru.26187
Article PubMed Google Scholar - Ostrosky-Zeichner L, Al-Obaidi M (2017) Invasive fungal infections in the intensive care unit. Infect Dis Clin N Am 31(3):475–487. https://doi.org/10.1016/j.idc.2017.05.005
Article Google Scholar - Taccone FS, Van den Abeele AM, Bulpa P et al (2015) Epidemiology of invasive aspergillosis in critically ill patients: clinical presentation, underlying conditions, and outcomes. Crit Care 19:7. https://doi.org/10.1186/s13054-014-0722-7
Article PubMed PubMed Central Google Scholar - Bassetti M, Righi E, Ansaldi F et al (2015) A multicenter multinational study of abdominal candidiasis: epidemiology, outcomes and predictors of mortality. Intensive Care Med 41(9):1601–1610. https://doi.org/10.1007/s00134-015-3866-2
Article PubMed Google Scholar - Kluge S, Strauss R, Kochanek M, Weigand MA, Rohde H, Lahmer T (2021) Aspergillosis: emerging risk groups in critically ill patients. Med Mycol. https://doi.org/10.1093/mmy/myab064
Article PubMed Google Scholar - Leroy O, Gangneux JP, Montravers P et al (2009) Epidemiology, management, and risk factors for death of invasive Candida infections in critical care: a multicenter, prospective, observational study in France (2005–2006). Crit Care Med 37(5):1612–1618. https://doi.org/10.1097/CCM.0b013e31819efac0
Article PubMed Google Scholar - Prattes J, Wauters J, Giacobbe DR et al (2022) Risk factors and outcome of pulmonary aspergillosis in critically ill coronavirus disease 2019 patients-a multinational observational study by the European Confederation of Medical Mycology. Clin Microbiol Infect 28(4):580–587. https://doi.org/10.1016/j.cmi.2021.08.014
Article CAS PubMed Google Scholar - Salmanton-Garcia J, Sprute R, Stemler J et al (2021) COVID-19-associated pulmonary aspergillosis, March–August 2020. Emerg Infect Dis 27(4):1077–1086. https://doi.org/10.3201/eid2704.204895
Article CAS PubMed PubMed Central Google Scholar - Schauwvlieghe A, Rijnders BJA, Philips N et al (2018) Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: a retrospective cohort study. Lancet Respir Med 6(10):782–792. https://doi.org/10.1016/S2213-2600(18)30274-1
Article PubMed Google Scholar - Janssen NAF, Nyga R, Vanderbeke L et al (2021) Multinational observational cohort study of COVID-19-associated pulmonary aspergillosis (1). Emerg Infect Dis 27(11):2892–2898. https://doi.org/10.3201/eid2711.211174
Article CAS PubMed PubMed Central Google Scholar - Bassetti M, Marchetti M, Chakrabarti A et al (2013) A research agenda on the management of intra-abdominal candidiasis: results from a consensus of multinational experts. Intensive Care Med 39(12):2092–2106. https://doi.org/10.1007/s00134-013-3109-3
Article PubMed Google Scholar - Blot SI, Taccone FS, Van den Abeele AM et al (2012) A clinical algorithm to diagnose invasive pulmonary aspergillosis in critically ill patients. Am J Respir Crit Care Med 186(1):56–64. https://doi.org/10.1164/rccm.201111-1978OC
Article PubMed Google Scholar - Bulpa P, Dive A, Sibille Y (2007) Invasive pulmonary aspergillosis in patients with chronic obstructive pulmonary disease. Eur Respir J 30(4):782–800. https://doi.org/10.1183/09031936.00062206
Article CAS PubMed Google Scholar - Koehler P, Bassetti M, Chakrabarti A et al (2021) Defining and managing COVID-19-associated pulmonary Aspergillosis: the 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect Dis 21(6):e149–e162. https://doi.org/10.1016/S1473-3099(20)30847-1
Article CAS PubMed Google Scholar - Vandewoude KH, Blot SI, Depuydt P et al (2006) Clinical relevance of Aspergillus isolation from respiratory tract samples in critically ill patients. Crit Care 10(1):R31. https://doi.org/10.1186/cc4823
Article PubMed PubMed Central Google Scholar - Verweij PE, Bruggemann RJM, Azoulay E et al (2021) Taskforce report on the diagnosis and clinical management of COVID-19 associated pulmonary aspergillosis. Intensive Care Med 47(8):819–834. https://doi.org/10.1007/s00134-021-06449-4
Article CAS PubMed PubMed Central Google Scholar - Verweij PE, Rijnders BJA, Bruggemann RJM et al (2020) Review of influenza-associated pulmonary aspergillosis in ICU patients and proposal for a case definition: an expert opinion. Intensive Care Med 46(8):1524–1535. https://doi.org/10.1007/s00134-020-06091-6
Article CAS PubMed PubMed Central Google Scholar - Donnelly JP, Chen SC, Kauffman CA et al (2020) Revision and update of the consensus definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis 71(6):1367–1376. https://doi.org/10.1093/cid/ciz1008
Article PubMed Google Scholar - Bassetti M, Scudeller L, Giacobbe DR et al (2019) Developing definitions for invasive fungal diseases in critically ill adult patients in intensive care units. Protocol of the FUNgal infections Definitions in ICU patients (FUNDICU) project. Mycoses 62(4):310–319. https://doi.org/10.1111/myc.12869
Article PubMed Google Scholar - Bassetti M, Giacobbe DR, Grecchi C et al (2020) Performance of existing definitions and tests for the diagnosis of invasive aspergillosis in critically ill, adult patients: a systematic review with qualitative evidence synthesis. J Infect 81(1):131–146. https://doi.org/10.1016/j.jinf.2020.03.065
Article CAS PubMed Google Scholar - Giacobbe DR, Cortegiani A, Karaiskos I et al (2021) Performance of existing definitions and tests for the diagnosis of invasive fungal diseases other than invasive candidiasis and invasive aspergillosis in critically ill, adult patients: a systematic review with qualitative evidence synthesis. J Fungi (Basel, Switzerland) 7(3):176. https://doi.org/10.3390/jof7030176
Article Google Scholar - Giacobbe DR, Asperges E, Cortegiani A et al (2022) Performance of existing clinical scores and laboratory tests for the diagnosis of invasive candidiasis in critically ill, nonneutropenic, adult patients: a systematic review with qualitative evidence synthesis. Mycoses 65(12):1073–1111. https://doi.org/10.1111/myc.13515
Article PubMed Google Scholar - Bassetti M, Zuccaro V, Asperges E, Scudeller L, Giacobbe DR, Investigators F (2022) Performance of existing definitions and tests for the diagnosis of invasive aspergillosis in critically ill, non-neutropenic, adult patients: an update including COVID-19 data. J Infect 85(5):573–607. https://doi.org/10.1016/j.jinf.2022.08.003
Article PubMed PubMed Central Google Scholar - Brook RH, Chassin MR, Fink A, Solomon DH, Kosecoff J, Park RE (1986) A method for the detailed assessment of the appropriateness of medical technologies. Int J Technol Assess Health Care 2(1):53–63. https://doi.org/10.1017/s0266462300002774
Article CAS PubMed Google Scholar - Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG (2009) Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 42(2):377–381. https://doi.org/10.1016/j.jbi.2008.08.010
Article PubMed Google Scholar - Williamson PR, Altman DG, Blazeby JM et al (2012) Developing core outcome sets for clinical trials: issues to consider. Trials 13:132. https://doi.org/10.1186/1745-6215-13-132
Article PubMed PubMed Central Google Scholar - Baldesi O, Bailly S, Ruckly S et al (2017) ICU-acquired candidaemia in France: epidemiology and temporal trends, 2004–2013—a study from the REA-RAISIN network. J Infect 75(1):59–67. https://doi.org/10.1016/j.jinf.2017.03.011
Article PubMed Google Scholar - Bassetti M, Righi E, Ansaldi F et al (2014) A multicenter study of septic shock due to candidemia: outcomes and predictors of mortality. Intensive Care Med 40(6):839–845. https://doi.org/10.1007/s00134-014-3310-z
Article CAS PubMed Google Scholar - Bassetti M, Vena A, Giacobbe DR et al (2022) Risk factors for intra-abdominal candidiasis in intensive care units: results from EUCANDICU study. Infect Dis Ther 11(2):827–840. https://doi.org/10.1007/s40121-021-00585-6
Article PubMed PubMed Central Google Scholar - Bassetti M, Vena A, Meroi M et al (2020) Factors associated with the development of septic shock in patients with candidemia: a post hoc analysis from two prospective cohorts. Crit Care 24(1):117. https://doi.org/10.1186/s13054-020-2793-y
Article PubMed PubMed Central Google Scholar - Kett DH, Azoulay E, Echeverria PM, Vincent JL, Extended Prevalence of Infection in ICUSGoI (2011) Candida bloodstream infections in intensive care units: analysis of the extended prevalence of infection in intensive care unit study. Crit Care Med 39(4):665–670. https://doi.org/10.1097/CCM.0b013e318206c1ca
Article PubMed Google Scholar - Paiva JA, Pereira JM, Tabah A et al (2016) Characteristics and risk factors for 28-day mortality of hospital acquired fungemias in ICUs: data from the EUROBACT study. Crit Care 20:53. https://doi.org/10.1186/s13054-016-1229-1
Article PubMed PubMed Central Google Scholar - Tortorano AM, Dho G, Prigitano A et al (2012) Invasive fungal infections in the intensive care unit: a multicentre, prospective, observational study in Italy (2006–2008). Mycoses 55(1):73–79. https://doi.org/10.1111/j.1439-0507.2011.02044.x
Article PubMed Google Scholar - Vincent JL, Rello J, Marshall J et al (2009) International study of the prevalence and outcomes of infection in intensive care units. JAMA 302(21):2323–2329. https://doi.org/10.1001/jama.2009.1754
Article CAS PubMed Google Scholar - Bassetti M, Azoulay E, Kullberg BJ et al (2021) EORTC/MSGERC definitions of invasive fungal diseases: summary of activities of the intensive care unit working group. Clin Infect Dis 72(Suppl 2):S121–S127. https://doi.org/10.1093/cid/ciaa1751
Article PubMed Google Scholar - Pappas PG, Lionakis MS, Arendrup MC, Ostrosky-Zeichner L, Kullberg BJ (2018) Invasive candidiasis. Nat Rev Dis Primers 4:18026. https://doi.org/10.1038/nrdp.2018.26
Article PubMed Google Scholar - Clancy CJ, Nguyen MH (2013) Finding the “missing 50%” of invasive candidiasis: how nonculture diagnostics will improve understanding of disease spectrum and transform patient care. Clin Infect Dis 56(9):1284–1292. https://doi.org/10.1093/cid/cit006
Article PubMed Google Scholar - Ruhnke M, Bohme A, Buchheidt D et al (2012) Diagnosis of invasive fungal infections in hematology and oncology-guidelines from the Infectious Diseases Working Party in Haematology and Oncology of the German Society for Haematology and Oncology (AGIHO). Ann Oncol 23(4):823–833. https://doi.org/10.1093/annonc/mdr407
Article CAS PubMed Google Scholar - De Waele JJ, Boelens J, Van De Putte D, Huis In ’t Veld D, Coenye T (2022) The role of abdominal drain cultures in managing abdominal infections. Antibiotics (Basel). 11(5):97. https://doi.org/10.3390/antibiotics11050697
Article CAS Google Scholar - Husain S, Mooney ML, Danziger-Isakov L et al (2011) A 2010 working formulation for the standardization of definitions of infections in cardiothoracic transplant recipients. J Heart Lung Transplant 30(4):361–374. https://doi.org/10.1016/j.healun.2011.01.701
Article PubMed PubMed Central Google Scholar - Maschmeyer G, Haas A, Cornely OA (2007) Invasive aspergillosis: epidemiology, diagnosis and management in immunocompromised patients. Drugs 67(11):1567–1601. https://doi.org/10.2165/00003495-200767110-00004
Article CAS PubMed Google Scholar - Baddley JW, Stephens JM, Ji X, Gao X, Schlamm HT, Tarallo M (2013) Aspergillosis in intensive care unit (ICU) patients: epidemiology and economic outcomes. BMC Infect Dis 13:29. https://doi.org/10.1186/1471-2334-13-29
Article PubMed PubMed Central Google Scholar - Meersseman W, Vandecasteele SJ, Wilmer A, Verbeken E, Peetermans WE, Van Wijngaerden E (2004) Invasive aspergillosis in critically ill patients without malignancy. Am J Respir Crit Care Med 170(6):621–625. https://doi.org/10.1164/rccm.200401-093OC
Article PubMed Google Scholar - Prattes J, Wauters J, Giacobbe DR, Lagrou K, Hoenigl M, Group E-CS (2021) Diagnosis and treatment of COVID-19 associated pulmonary apergillosis in critically ill patients: results from a European confederation of medical mycology registry. Intensive Care Med 47(10):1158–1160. https://doi.org/10.1007/s00134-021-06471-6
Article CAS PubMed PubMed Central Google Scholar - van de Veerdonk FL, Kolwijck E, Lestrade PP et al (2017) Influenza-associated aspergillosis in critically ill patients. Am J Respir Crit Care Med 196(4):524–527. https://doi.org/10.1164/rccm.201612-2540LE
Article PubMed Google Scholar - Bartoletti M, Pascale R, Cricca M et al (2021) Epidemiology of invasive pulmonary aspergillosis among intubated patients with COVID-19: a prospective study. Clin Infect Dis 73(11):e3606–e3614. https://doi.org/10.1093/cid/ciaa1065
Article CAS PubMed Google Scholar - Borman AM, Palmer MD, Fraser M et al (2020) COVID-19-associated invasive aspergillosis: data from the UK National Mycology Reference Laboratory. J Clin Microbiol. https://doi.org/10.1128/JCM.02136-20
Article PubMed PubMed Central Google Scholar - Lahmer T, Kriescher S, Herner A et al (2021) Invasive pulmonary aspergillosis in critically ill patients with severe COVID-19 pneumonia: results from the prospective AspCOVID-19 study. PLoS ONE 16(3):e0238825. https://doi.org/10.1371/journal.pone.0238825
Article CAS PubMed PubMed Central Google Scholar - Nyga R, Maizel J, Nseir S et al (2020) Invasive tracheobronchial aspergillosis in critically ill patients with severe influenza. A clinical trial. Am J Respir Crit Care Med 202(5):708–716. https://doi.org/10.1164/rccm.201910-1931OC
Article PubMed Google Scholar - Permpalung N, Chiang TP, Massie AB et al (2022) Coronavirus disease 2019-associated pulmonary aspergillosis in mechanically ventilated patients. Clin Infect Dis 74(1):83–91. https://doi.org/10.1093/cid/ciab223
Article CAS PubMed Google Scholar - van de Veerdonk FL, Wauters J, Verweij PE (2020) Invasive aspergillus tracheobronchitis emerging as a highly lethal complication of severe influenza. Am J Respir Crit Care Med 202(5):646–648. https://doi.org/10.1164/rccm.202005-1883ED
Article PubMed PubMed Central Google Scholar - Ergun M, Bruggemann RJM, Alanio A et al (2021) Aspergillus test profiles and mortality in critically ill COVID-19 patients. J Clin Microbiol 59(12):e0122921. https://doi.org/10.1128/JCM.01229-21
Article PubMed Google Scholar - Giacobbe DR, Prattes J, Wauters J et al (2022) Prognostic impact of bronchoalveolar lavage fluid galactomannan and aspergillus culture results on survival in COVID-19 intensive care unit patients: a post hoc analysis from the European Confederation of Medical Mycology (ECMM) COVID-19-associated pulmonary aspergillosis study. J Clin Microbiol 60(4):e0229821. https://doi.org/10.1128/jcm.02298-21
Article CAS PubMed Google Scholar - Di Meco G, Mora S, Giacobbe DR et al (2022) A wide database for a multicenter study on Pneumocystis jirovecii pneumonia in intensive care units. Stud Health Technol Inform 294:557–558. https://doi.org/10.3233/SHTI220521
Article PubMed Google Scholar - Giacobbe DR, Dettori S, Di Pilato V et al (2023) Pneumocystis jirovecii pneumonia in intensive care units: a multicenter study by ESGCIP and EFISG. Crit Care 27(1):323. https://doi.org/10.1186/s13054-023-04608-1
Article PubMed PubMed Central Google Scholar
Acknowledgements
We would like to thank Intensive Care Medicine editors and reviewers for the insightful comments provided during the review process, and Giulia Viglietti and Helena Policardi for their assistance and technical support during voting rounds. FUNDICU collaborators Claire Roger (Department of Anesthesiology, Critical Care, Pain and Emergency Medicine, Nimes University Hospital, Place du Professeur Robert Debré, Nîmes Cedex, France; UR UM103 IMAGINE, Univ Montpellier, Montpellier, France), Christian Eckmann (Academic Hospital of Goettingen University, Department of General, Visceral and Thoracic Surgery, Klinikum Hannoversch-Muenden, Hannoversch-Muenden), Jean-Pierre Gangneux (Université Rennes, CHU de Rennes, Inserm, Irset (Institut de Recherche en Santé, Environnement et Travail) UMR_S 1085, Rennes, France), Esther Segal (Department of Clinical Microbiology and Immunology, Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel), Geoffrey Coombs (Antimicrobial Resistance and Infectious Diseases Research Laboratory, Murdoch University, Perth, WA, Australia), Andreas Voss (Department of Medical Microbiology and Infectious Diseases, Canisius Wilhelmina Hospital, Nijmegen, The Netherlands; Radboud Center for Infectious Diseases, Radboud University Medical Center, Nijmegen, The Netherlands)
Funding
The present project did not require additional funding from routine research activities. Open access cost for this publication was covered by ESGCIP funds. JDW is supported by a Sr Clinical Research Grant from the Research Foundation Flanders (FWO, Ref. 1881020N).
Author information
Authors and Affiliations
- Department of Health Sciences (DISSAL), University of Genoa, Genoa, Italy
Matteo Bassetti, Daniele R. Giacobbe & Antonio Vena - Infectious Diseases Unit, IRCCS Ospedale Policlinico San Martino, L.go R. Benzi 10, 16132, Genoa, Italy
Matteo Bassetti, Daniele R. Giacobbe & Antonio Vena - Anaesthesiology and Intensive Care, Karolinska University Hospital Huddinge, Stockholm, Sweden
Christina Agvald-Ohman - Department of Infectious Diseases and Clinical Microbiology, Faculty of Medicine, Hacettepe University, Ankara, Turkey
Murat Akova - Mycology Reference Laboratory, National Centre for Microbiology, Instituto de Salud Carlos III, Majadahonda, Madrid, Spain
Ana Alastruey-Izquierdo & Manuel Cuenca-Estrella - Centro de Investigación Biomédica en Red (CIBER) de Enfermedades Infecciosas-CIBERINFEC, Madrid, Spain
Ana Alastruey-Izquierdo - Department of Medical Microbiology, Faculty of Medicine, Hacettepe University, Ankara, Turkey
Sevtap Arikan-Akdagli - Université de Paris, Paris, France
Elie Azoulay - Service de Médecine Intensive Et Réanimation, Hôpital Saint-Louis, AP-HP, Paris, France
Elie Azoulay - Department of Internal Medicine and Pediatrics, Faculty of Medicine and Health Sciences, Ghent University, Ghent, Belgium
Stijn Blot - UQ Centre for Clinical Research, Faculty of Medicine, The University of Queensland, Brisbane, Australia
Stijn Blot - Department I of Internal Medicine, Center for Integrated Oncology Aachen Bonn Cologne Duesseldorf (CIO ABCD) and Excellence Center for Medical Mycology (ECMM), Faculty of Medicine and University Hospital Cologne, University of Cologne, Cologne, Germany
Oliver A. Cornely & Philipp Koehler - Faculty of Medicine and University Hospital Cologne, Institute of Translational Research, Cologne Excellence Cluster On Cellular Stress Responses in Aging-Associated Diseases (CECAD), University of Cologne, Cologne, Germany
Oliver A. Cornely - Faculty of Medicine and University Hospital Cologne, Clinical Trials Centre Cologne (ZKS Köln), University of Cologne, Cologne, Germany
Oliver A. Cornely - German Centre for Infection Research (DZIF), Partner Site Bonn-Cologne, Cologne, Germany
Oliver A. Cornely - Department of Intensive Care Medicine, University Medical Center, University Utrecht, Utrecht, The Netherlands
Dylan W. de Lange - Department of Medical Sciences, Infectious Diseases, University of Turin, Turin, Italy
Francesco G. De Rosa - Department of Critical Care Medicine, Ghent University Hospital, Ghent, Belgium
Jan J. De Waele - Department of Critical Care, University Hospital Attikon, Attikon Medical School, National and Kapodistrian University of Athens, Athens, Greece
George Dimopoulos - Intensive Care Unit, Virgen del Rocío University Hospital, Seville, Spain
Jose Garnacho-Montero - Division of Infectious Diseases, Department of Internal Medicine, Medical University of Graz, Graz, Austria
Martin Hoenigl - BioTechMed, Graz, Austria
Martin Hoenigl - Translational Mycology Working Group, ECMM Excellence Center for Clinical Mycology, Medical University of Graz, Graz, Austria
Martin Hoenigl - Division of Infectious Diseases, and Center for Infectious Diseases Research, American University of Beirut Medical Center, Beirut, Lebanon
Souha S. Kanj - Medical Faculty and University Hospital Cologne, Cologne Excellence Cluster on Cellular Stress Responses in Aging-Associated Diseases (CECAD), University of Cologne, Cologne, Germany
Philipp Koehler - Department of Medicine and Radboud Center for Infectious Diseases, Radboud University Medical Center, Nijmegen, The Netherlands
Bart J. Kullberg - Institute of Microbiology, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland
Frédéric Lamoth - Service of Immunology and Allergy and Center of Human Immunology Lausanne, Department of Medicine, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland
Frédéric Lamoth & Thierry Calandra - Department of Laboratory Medicine and Pathology, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland
Frédéric Lamoth & Thierry Calandra - Institute of Hygiene and Medical Microbiology, Medical University of Innsbruck, Innsbruck, Austria
Cornelia Lass-Flörl - Universitair Ziekenhuis Leuven, Louvain, Belgium
Johan Maertens - Department of Intensive Care Medicine, Multidisciplinary Intensive Care Research Organization (MICRO), St James’ Hospital, Dublin, Ireland
Ignacio Martin-Loeches - Clinical Microbiology and Infectious Diseases, Hospital General Universitario Gregorio Marañón, Madrid, Spain
Patricia Muñoz - Instituto de Investigación Sanitaria Gregorio Marañón, Madrid, Spain
Patricia Muñoz - Centro de Investigación Biomédica en Red (CIBER) de Enfermedades Respiratorias-CIBERES (CB06/06/0058), Madrid, Spain
Patricia Muñoz - Medicine Department, Faculty of Medicine, Universidad Complutense de Madrid, Madrid, Spain
Patricia Muñoz - Third Department of Internal Medicine, School of Medicine, Sotiria General Hospital, National and Kapodistrian University, Athens, Greece
Garyphallia Poulakou - Clinical Research/Epidemiology in Pneumonia and Sepsis (CRIPS), Vall d’Hebron Institut of Research (VHIR), Barcelona, Spain
Jordi Rello & Sofia Tejada - Clinical Research in the ICU, CHU Nimes, Universite de Nimes-Montpellier, Nimes, France
Jordi Rello - Medicine Department, Universitat Internacional de Catalunya (UIC), Sant Cugat, Spain
Jordi Rello - Centro de Investigación Biomédica en Red de Enfermedades Respiratorias (CIBERES), Instituto de Salud Carlos III, Madrid, Spain
Jordi Rello & Sofia Tejada - Dipartimento di Scienze di Laboratorio E Infettivologiche, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy
Maurizio Sanguinetti - Dipartimento di Scienze Biotecnologiche di Base, Cliniche Intensivologiche e Perioperatorie, Università Cattolica del Sacro Cuore, Rome, Italy
Maurizio Sanguinetti - Department of Intensive Care, Hôpital Universitaire de Bruxelles (HUB), Université Libre de Bruxelles (ULB), Brussels, Belgium
Fabio S. Taccone - Medical and Infectious Diseases Intensive Care Unit, AP-HP, Bichat Claude Bernard University Hospital, Paris, France
Jean-François Timsit - IAME UMR 1137, Université Paris-Cité, Paris, France
Jean-François Timsit - Department of Pneumology, Hospital Clinic of Barcelona, Barcelona, Spain
Antoni Torres - August Pi i Sunyer Biomedical Research Institute (IDIBAPS), University of Barcelona, Barcelona, Spain
Antoni Torres - Biomedical Research Networking Centres in Respiratory Diseases (CIBERES), Barcelona, Spain
Antoni Torres - Catalan Institution for Research and Advanced Studies (ICREA), Barcelona, Spain
Antoni Torres - Department of Medicine/Division of Infectious Disease, Medical College of Georgia/Augusta University, Augusta, GA, USA
Jose A. Vazquez - Medical Intensive Care Unit, University Hospitals Leuven, Louvain, Belgium
Joost Wauters - Infectious Diseases Unit, IRCCS San Matteo, Pavia, Italy
Erika Asperges & Valentina Zuccaro - Department of Precision Medicine in Medical, Surgical and Critical Care (Me.Pre.C.C.), University of Palermo, Palermo, Italy
Andrea Cortegiani - Department of Anesthesia Intensive Care and Emergency, University Hospital Policlinico Paolo Giaccone, Palermo, Italy
Andrea Cortegiani - Malattie Infettive, Azienda Socio Sanitaria Territoriale (ASST) di Lodi, Lodi, Italy
Cecilia Grecchi - 1st Department of Internal Medicine-Infectious Diseases, Hygeia General Hospital, Athens, Greece
Ilias Karaiskos - Saint Eloi Department of Anesthesiology and Critical Care Medicine, Montpellier University Health Care Center, Montpellier, France
Clément Le Bihan - Department of Microbiology, Immunology and Transplantation, KU Leuven, Louvain, Belgium
Toine Mercier - Department of Hematology, University Hospitals Leuven, Louvain, Belgium
Toine Mercier - Department of Medicine, Regional Hospital West Jutland, Herning, Denmark
Klaus L. Mortensen - Infectious and Tropical Diseases Unit, Department of Medicine and Surgery, University of Insubria-ASST-Sette Laghi, Varese, Italy
Maddalena Peghin - Scientific Direction, IRCCS Istituto Giannina Gaslini, Genoa, Italy
Chiara Rebuffi - Research and Innovation Unit, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy
Luigia Scudeller
Authors
- Matteo Bassetti
- Daniele R. Giacobbe
- Christina Agvald-Ohman
- Murat Akova
- Ana Alastruey-Izquierdo
- Sevtap Arikan-Akdagli
- Elie Azoulay
- Stijn Blot
- Oliver A. Cornely
- Manuel Cuenca-Estrella
- Dylan W. de Lange
- Francesco G. De Rosa
- Jan J. De Waele
- George Dimopoulos
- Jose Garnacho-Montero
- Martin Hoenigl
- Souha S. Kanj
- Philipp Koehler
- Bart J. Kullberg
- Frédéric Lamoth
- Cornelia Lass-Flörl
- Johan Maertens
- Ignacio Martin-Loeches
- Patricia Muñoz
- Garyphallia Poulakou
- Jordi Rello
- Maurizio Sanguinetti
- Fabio S. Taccone
- Jean-François Timsit
- Antoni Torres
- Jose A. Vazquez
- Joost Wauters
- Erika Asperges
- Andrea Cortegiani
- Cecilia Grecchi
- Ilias Karaiskos
- Clément Le Bihan
- Toine Mercier
- Klaus L. Mortensen
- Maddalena Peghin
- Chiara Rebuffi
- Sofia Tejada
- Antonio Vena
- Valentina Zuccaro
- Luigia Scudeller
- Thierry Calandra
Consortia
the Study Group for Infections in Critically Ill Patients of the European Society of Clinical Microbiology and Infectious Diseases (ESGCIP), the Fungal Infection Study Group of the European Society of Clinical Microbiology and Infectious Diseases (EFISG), the European Society of Intensive Care Medicine (ESICM), the European Confederation of Medical Mycology (ECMM), the Mycoses Study Group Education and Research Consortium (MSGERC), the International Society of Antimicrobial Chemotherapy (ISAC), the International Society for Human and Animal Mycology (ISHAM), the Austrian Society for Medical Mycology (ÖGMM), the Italian Society of Anesthesia, Analgesia, Reanimation, and Intensive Care (SIAARTI), the Italian Society of Anti-Infective Therapy (SITA), and the FUNDICU Collaborators
- Claire Roger
- , Christian Eckmann
- , Jean-Pierre Gangneux
- , Esther Segal
- , Geoffrey Coombs
- & Andreas Voss
Contributions
MB (ESGCIP chair; coordination of the project, first drafting of IFD definitions after systematic review, development of IFD definitions and consensus document); DRG (ESGCIP; coordination of the project, protocol development, systematic review, drafting of consensus document); CA-O (ESICM; development of IFD definitions and consensus document); MA (ESGCIP, EFISG; development of IFD definitions and consensus document); AA-I (EFISG chair, ECMM, ISHAM; development of IFD definitions and consensus document); SAA (EFISG, ECMM; development of IFD definitions and consensus document); EA (ESICM; development of IFD definitions and consensus document); SB (ESICM; development of IFD definitions and consensus document); OAC (past ECMM president, EFISG, MSGERC; development of IFD definitions and consensus document; ISHAM treasurer); MC-E (EFISG; development of IFD definitions and consensus document); DWL (ESICM; development of IFD definitions and consensus document); FGR (ESGCIP; development of IFD definitions and consensus document); JJW (ESICM; development of IFD definitions and consensus document); GD (ESICM, ESGCIP; development of IFD definitions and consensus document); JG-M (ESICM; development of IFD definitions and consensus document); MH (ECMM president, ISHAM, EFISG, MSGERC; development of IFD definitions and consensus document); SSK (development of IFD definitions and consensus document); PK (EFISG, ESGCIP, ISHAM and MSGERC member; development of IFD definitions and consensus document); BJK (MSGERC; development of IFD definitions and consensus document); FL (ECMM, EFISG; development of IFD definitions and consensus document), CL-F (past EFISG chair; first drafting of IFD definitions after systematic review, development of IFD definitions and consensus document); JM (development of IFD definitions and consensus document), IM-L (ESICM; development of IFD definitions and consensus document); PM (ESGCIP, EFISG; development of IFD definitions and consensus document); GP (ESGCIP; development of IFD definitions and consensus document); JR (development of IFD definitions and consensus document); MS (EFISG; development of IFD definitions and consensus document); FST (ESICM; development of IFD definitions and consensus document), J-FT (past ESCGIP chair, ESICM; development of IFD definitions and consensus document); AT (development of IFD definitions and consensus document); JAV (MSGERC; development of IFD definitions and consensus document); JW (EFISG; development of IFD definitions and consensus document); EA (systematic review); AC (systematic review); CG (systematic review); IK (systematic review); CL (systematic review); TM (systematic review); KLM (systematic review); MP (systematic review); CR (systematic review); ST (systematic review); AV (systematic review); VZ (systematic review); LS (protocol development, supervision of systematic review, facilitation of face-to-face meeting/s); TC (coordination, development of IFD definitions and consensus document).
Corresponding author
Correspondence toMatteo Bassetti.
Ethics declarations
Conflicts of interest
Outside the submitted work, MB reports research grants and/or personal fees for advisor/consultant and/or speaker/chairman from BioMérieux, Cidara, Gilead, Menarini, MSD, Pfizer, and Shionogi. Outside the submitted work, DRG reports investigator-initiated grants from Pfizer Inc, Shionogi, BioMérieux, and Gilead Italia, and personal fees for advisor/speaker from Pfizer Inc., Menarini, and Tillotts Pharma. Outside the submitted work, AAI reports fees for educational lectures from Gilead, Pfizer, and MSD; grants from Instituto de Salud Carlos III and ESCMID; advisor for the Joint Program Initiative on Antimicrobial Resistance and the WHO Technical Expert Group for the Development of the Fungal Priority Pathogens List; travel support from Gilead. Outside the submitted work, EA reports grants from Pfizer and MSD, and honoraria for lectures or presentations from Gilead, Pfizer, Alexion, Mindray, and Sanofi. OAC reports grants or contracts from BMBF, Cidara, EU-DG RTD (101037867), F2G, Gilead, MedPace, MSD, Mundipharma, Octapharma, Pfizer, Scynexis; Consulting fees from Abbvie, AiCuris, Biocon, Cidara, Gilead, IQVIA, Janssen, Matinas, MedPace, Menarini, Moderna, Molecular Partners, MSG-ERC, Noxxon, Octapharma, Pfizer, PSI, Scynexis, Seres; honoraria for lectures from Abbot, Abbvie, Al-Jazeera Pharmaceuticals/Hikma Gilead, Grupo Biotascana/United Medical/Knight ISHAM Working group, MedScape, MedUpdate, Merck/MSD, Noscendo, Pfizer,Shionogi, StreamedUp; payment for expert testimony from Cidara; Participation on a Data Safety Monitoring Board or Advisory Board from Boston Strategic Partners, Cidara, IQVIA, Janssen, MedPace, Pulmocide, Shionogi, PSI, The Prime Meridian Group; a pending patent currently reviewed at the German Patent and Trade Mark Office; stoke or stoke options from CoRe Consulting and EasyRadiology; other interests from Wiley, outside the submitted work. Outside the submitted work, FGDR reports consulting fess/honoraria for lectures from MSD, Pfizer, and Gilead Sciences, and travel fees from Pfizer and MSD. JDW reports grants for advisor/consultant or speaker/chairman from for MSD, Pfizer, and ThermoFisher (fees and honoraria paid to institution). GD reports honoraria for lectures/presentations from Gilead, Pfizer, and InfectoPharm. JGM reports personal fees for advisor/consultant and/or speaker/chairman from Gilead and Pfizer. MH received research funding from Gilead Sciences, Astellas, Mundipharma, Euroimmune, MSD, Pulmocide, IMMY, Scynexis, F2G and Pfizer, outside the submitted work. Outside the submitted work, SSK reports fees for lectures/advisory board from Basilea, MSD, Pfizer, and Hikma. PK reports grants or contracts from German Federal Ministry of Research and Education (BMBF) B-FAST (Bundesweites Forschungsnetz Angewandte Surveillance und Testung) and NAPKON (Nationales Pandemie Kohorten Netz, German National Pandemic Cohort Network) of the Network University Medicine (NUM) and the State of North Rhine-Westphalia; consulting fees Ambu GmbH, Gilead Sciences, Mundipharma Resarch Limited, Noxxon N.V. and Pfizer Pharma; honoraria for lectures from Akademie für Infektionsmedizin e.V., Ambu GmbH, Astellas Pharma, BioRad Laboratories Inc., Datamed GmbH, European Confederation of Medical Mycology, Gilead Sciences, GPR Academy Ruesselsheim, HELIOS Kliniken GmbH, Lahn-Dill-Kliniken GmbH, medupdate GmbH, MedMedia GmbH, MSD Sharp & Dohme GmbH, Pfizer Pharma GmbH, Scilink Comunicación Científica SC and University Hospital and LMU Munich; participation on an Advisory Board from Ambu GmbH, Gilead Sciences, Mundipharma Resarch Limited and Pfizer Pharma; a pending patent currently reviewed at the German Patent and Trade Mark Office (DE 10 2021 113 007.7); other non-financial interests from Elsevier, Wiley and Taylor & Francis online outside the submitted work. Outside the submitted work, FL reports grants from Pfizer, Gilead, MSD, Novartis, Swiss National Science Foundation, Santos-Suarez Foundation; and honoraria for lectures/presentation from Gilead, Pfizer, MSD, Mundipharma. Outside the submitted work, CLF reports research grants and/or personal fees for advisor/consultant, travel and/or speaker/chairman from Gilead, MSD, Pfizer, BioMérieux, F2G, IMMY, Shionogi, Astellas Pharma. Outside the submitted work, JM reports research grants and/or personal fees for advisor/consultant, and/or speaker/chairman from Gilead Sciences, F2G, Shionogi, Mundipharma, Mundipharma, Takeda, and Basilea. Outside the submitted work, IML reports grants from Grifols; consulting fees from MSD, Gilead, Mundipharma, fees for lectures/advisory board from Gilead, MSD, and Mundipharma; travel support from the European Respiratory Society (Chair Critical Care Group). Outside the submitted work, PM reports fees for lectures/advisory board from Gilead, MSD, Mundipharma, Pfizer. Outside of the submitted work, GP reports fees for lectures/advisory board from AstraZeneca, Gilead, Glaxo, Menarini, MSD, Pfizer and SOBI; grants from Adagio Therapeutics, AstraZeneca, Bausch, Fabentech, Pfizer, PharmaMar, Roche, Xenothera. Outside the submitted work, JR reports consulting fees from Pfizer; honoraria for lectures/presentations from Pfizer, MSD, and Roche; travel support from Roche. Outside the submitted work, J-FT reports grants from Pfizer and MSD; consulting fees from Gilead; honoraria for lectures/presentations from Mundipharma, Gilead, and Pfizer; Advisor fees from MSD, Pfizer, BD, Aspen, Roche diagnostic, and BioMérieux. Outside the submitted work, AT reports consultant/speaker fees from Pfizer, Poliphor, MSD, Jansen, and OM Pharma. Outside the submitted work, JAV reports consulting fees from F2G and Cidara; honoraria for lectures/presentations from Melinta. Outside the submitted work, JW reports investigator-initiated research grants, speaker honoraria and travel grants from Pfizer and Gilead. Outside the submitted work, AC reports fees for lectures/advisory board from Gilead, MSD, Mundipharma, Pfizer. Outside the submitted work, IK reports grants and honoraria for lectures/presentations from Pfizer and BioMérieux. Outside the submitted work, TM reports consultancy fees from Gilead Sciences, Pfizer and AstraZeneca, unrestricted research grants from Gilead Sciences, and travel support from AstraZeneca. Outside the submitted work, KM reports travel support from Gilead. Outside the submitted work, MP reports honoraria for lectures/presentations from Dia Sorin, MDS, Menarini, Pfizer, and ThermoFisher. Outside the submitted work, LS reports travel support from ESCMID. TC has participated in advisory/safety monitoring boards or consulted for Cidara, Novartis, MSD Merck Sharp & Dohme AG, Shionogi and Gilead and received grant from European Community (Horizon 2020, HDM-FUN Grant; host-directed medicine in invasive fungal infections, co-applicant) for projects unrelated to the submitted work; all contracts were made with and fees paid to his institution (CHUV).
Ethics and consent
The present consensus document does not involve patients’ data and does not require approval by Ethical Review Board.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
FUNDICU Collaborators are listed in acknowledgements section.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article
Cite this article
Bassetti, M., Giacobbe, D.R., Agvald-Ohman, C. et al. Invasive Fungal Diseases in Adult Patients in Intensive Care Unit (FUNDICU): 2024 consensus definitions from ESGCIP, EFISG, ESICM, ECMM, MSGERC, ISAC, and ISHAM.Intensive Care Med 50, 502–515 (2024). https://doi.org/10.1007/s00134-024-07341-7
- Received: 09 October 2023
- Accepted: 31 January 2024
- Published: 21 March 2024
- Version of record: 21 March 2024
- Issue date: April 2024
- DOI: https://doi.org/10.1007/s00134-024-07341-7
Keywords
Profiles
- Daniele R. Giacobbe View author profile
- Oliver A. Cornely View author profile
- Frédéric Lamoth View author profile
- Ignacio Martin-Loeches View author profile