Long-term intubation and high rate of tracheostomy in COVID-19 patients might determine an unprecedented increase of airway stenoses: a call to action from the European Laryngological Society (original) (raw)
Introduction
The novel Coronavirus disease 2019 (COVID-19) is a highly contagious, pandemic zoonosis, caused by an RNA betacoronavirus called severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). In most patients, the disease takes a mild form with symptoms like fever, cough, nausea, vomiting, and diarrhea, but it can also cause massive involvement of the lower respiratory tract with interstitial pneumonia [1]. Despite the low mortality rate (1.4–2.3%) [1,[2](#ref-CR2 "Wu Z, McGoogan JM (2020) Characteristics of and important lessons from the Coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72314 cases from the Chinese Center for Disease Control and Prevention. JAMA. https://doi.org/10.1001/jama.2020.2648
(Published online ahead of print, 2020 Feb 24)"),[3](#ref-CR3 "Huang C, Wang Y, Li X et al (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395:497–506"),[4](/article/10.1007/s00405-020-06112-6#ref-CR4 "Wang D, Hu B, Hu C et al (2020) Clinical characteristics of 138 hospitalized patients with 2019 novel Coronavirus-infected pneumonia in Wuhan. JAMA 323:1061–1069")\] and the relatively, low number of patients needing critical care (in the range between 5 and 12%) \[[1](/article/10.1007/s00405-020-06112-6#ref-CR1 "Guan WJ, Ni ZY, Hu Y et al (2020) Clinical characteristics of Coronavirus disease 2019 in China. N Engl J Med 382:1708–1720"), [5](/article/10.1007/s00405-020-06112-6#ref-CR5 "Kowalski LP, Sanabria A, Ridge JA et al (2020) COVID-19 pandemic: Effects and evidence-based recommendations for otolaryngology and head and neck surgery practice. Head Neck.
https://doi.org/10.1002/hed.26164
(Published online ahead of print, 2020 Apr 9)"), [6](/article/10.1007/s00405-020-06112-6#ref-CR6 "Phua J, Weng L, Ling L et al (2020) Intensive care management of Coronavirus disease 2019 (COVID-19): challenges and recommendations. Lancet Respir Med 8:506–517")\], due to its high transmissibility and the sheer number of infected patients, SARS-CoV-2 is placing a major burden on health systems globally, causing an unprecedented overwhelming of hospital facilities, especially intensive care units (ICU) \[[5](/article/10.1007/s00405-020-06112-6#ref-CR5 "Kowalski LP, Sanabria A, Ridge JA et al (2020) COVID-19 pandemic: Effects and evidence-based recommendations for otolaryngology and head and neck surgery practice. Head Neck.
https://doi.org/10.1002/hed.26164
(Published online ahead of print, 2020 Apr 9)")\]. In the recent experience, the median time from symptom onset to the development of pneumonia was approximately 5 days, while the mean time from symptoms onset to ICU admission for severe hypoxemia was approximately 7–12 days. The cause of severe hypoxemia was essentially correlated to the acute respiratory distress syndrome in 60–70% of cases, followed by shock in 30%, myocardial dysfunction in 20–30%, and acute renal failure in 10–30% \[[6](/article/10.1007/s00405-020-06112-6#ref-CR6 "Phua J, Weng L, Ling L et al (2020) Intensive care management of Coronavirus disease 2019 (COVID-19): challenges and recommendations. Lancet Respir Med 8:506–517")\].COVID-19 patients admitted to the ICU often require prolonged mechanical ventilation with high positive end-expiratory pressure through an endotracheal tube, with a frequency reported as high as 88% in a series of 1591 consecutive patients treated at 72 hospitals included in the COVID-19 Lombardy ICU Network, Italy [7]. In pre-COVID-19 settings, tracheostomy performed after 7–14 days from endotracheal intubation significantly improved the chance of successful weaning and lowered the risk of complications and mortality when compared to long-term maintenance of the orotracheal tube in place [[8](#ref-CR8 "Tay JK, Khoo ML, Loh WS (2020) Surgical considerations for tracheostomy during the COVID-19 pandemic: lessons learned from the Severe Acute Respiratory Syndrome outbreak. JAMA Otolaryngol Head Neck Surg. https://doi.org/10.1001/jamaoto.2020.0764
(Published online ahead of print, 2020 Mar 31)"),[9](#ref-CR9 "Freeman BD, Morris PE (2012) Tracheostomy practice in adults with acute respiratory failure. Crit Care Med 40:2890–2896"),[10](#ref-CR10 "Siempos II, Ntaidou TK, Filippidis FT, Choi AMK (2015) Effect of early versus late or no tracheostomy on mortality and pneumonia of critically ill patients receiving mechanical ventilation: a systematic review and meta-analysis. Lancet Respir Med 3:150–158"),[11](#ref-CR11 "Cheung NH, Napolitano LM (2014) Tracheostomy: epidemiology, indications, timing, technique, and outcomes. Respir Care 59:895–899"),[12](#ref-CR12 "Huang H, Li Y, Ariani F, Chen X, Lin J (2014) Timing of tracheostomy in critically ill patients: a meta-analysis. PLoS ONE 9:e92981"),[13](/article/10.1007/s00405-020-06112-6#ref-CR13 "Lin WC, Chen CW, Wang JD, Tsai LM (2015) Is tracheostomy a better choice than translaryngeal intubation for critically ill patients requiring mechanical ventilation for more than 14 days? A comparison of short-term outcomes. BMC Anesthesiol 15:181")\]. Moreover, in a resource-constrained scenario like that associated to the current pandemic, early tracheostomy would present the advantages of a more rapid weaning and ensuing higher availability of ventilators.Despite these pros, the actual clinical practice for COVID-19 patients admitted in several ICUs worldwide is to try to postpone tracheostomy until the patient no longer needs to be ventilated in the prone position and has been determined to be cleared of the virus with isolation precautions ceasing. This is mainly because of the high risk of accidental decannulation during proning and the chance of cross-infection of healthcare professionals (HCPs) due to prolonged duration of tracheal viral positivity compared with the salivary viral load [[14](/article/10.1007/s00405-020-06112-6#ref-CR14 "Sommer DD, Engels PT, Weitzel EK et al (2020) Recommendations from the CSO-HNS taskforce on performance of tracheotomy during the COVID-19 pandemic. J Otolaryngol Head Neck Surg 49(1):23. https://doi.org/10.1186/s40463-020-00414-9
"), [15](/article/10.1007/s00405-020-06112-6#ref-CR15 "To KK, Tsang OT, Leung WS et al (2020) Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: an observational cohort study. Lancet Infect Dis 20:565–574")\]. Unfortunately, when strictly followed, such a policy may mean that patients remain intubated for up to 3–4 weeks. This is clearly far from the usual pre-pandemic standards and a strong effort should be prospectively made to demonstrate that a potential increase in the incidence and severity of laryngotracheal injuries in a given patient is counterbalanced by the potential benefits for him (in terms of reduced risk of accidental decannulation) and to other patients and HCPs (in terms of reduced risk of cross-infections). In the meantime, however, as a consequence of the combination of an increased number of long-term intubated, critically ill patients, and delayed tracheostomy, it is probable that, in the near future, an unprecedented rise of iatrogenic sequelae ranging from granulomas, webs, and laryngotracheal stenosis (LTS), to tracheomalacia, tracheal necrosis, tracheo-esophageal, and tracheo-innominate fistulae may come to arise \[[16](/article/10.1007/s00405-020-06112-6#ref-CR16 "Fiz I, Monnier P, Koelmel JC et al (2019) Multicentric study applying the European Laryngological Society classification of benign laryngotracheal stenosis in adults treated by tracheal or cricotracheal resection and anastomosis. Laryngoscope.
https://doi.org/10.1002/lary.28274
(Published online ahead of print, 2019 Sep 11)"), [17](/article/10.1007/s00405-020-06112-6#ref-CR17 "Nikolovski N, Kopacheva-Barsova G, Pejkovska A (2019) Laryngotracheal stenosis: a retrospective analysis of their aetiology, diagnose and treatment. Open Access Maced J Med Sci 7:1649–1656")\].The aim of the present paper from the Laryngotracheal Stenosis Committee of the European Laryngological Society is, therefore, to alert the medical and scientific communities to the possibility of a surge in the number of airway injuries in the short and medium term, to provide a narrative review of the main mechanisms potentially leading to laryngotracheal injuries during prolonged intubation and tracheostomy, and to help in proactively diagnosing and treating LTS.
Preventive measures to avoid airway stenosis
Airway management, by either endotracheal intubation or tracheostomy/cricothyrotomy placement, must be acknowledged as an hazardous procedure due to the potential SARS-CoV-2 airborne cross-infection of HCPs and other patients [18]. Consequently, it is of utmost importance that the ‘most appropriate’ clinician manages the airway to enable its successful establishment in a safe, accurate, and swift manner.
The first step for doing this is represented by an accurate plan, taking into account the possibility of difficult airway management, possibly associated to COVID-19-related laryngitis and laryngeal edema [[19](/article/10.1007/s00405-020-06112-6#ref-CR19 "McGrath BA, Wallace S, Goswamy J (2020) Laryngeal oedema associated with COVID-19 complicating airway management. Anaesthesia. https://doi.org/10.1111/anae.15092
(Published online ahead of print, 2020 Apr 17)")\]. Difficult intubation is defined by repeated failing attempts to introduce an endotracheal tube, prolonged duration of such maneuvers, or necessity for multiple approaches and/or intubation devices \[[20](/article/10.1007/s00405-020-06112-6#ref-CR20 "Barjaktarevic I, Esquinas AM, West FM, Albores J, Berlin D (2017) Noninvasive ventilation in difficult endotracheal intubation: systematic and review analysis. Anaesthesiol Intensive Ther 49:294–302")\]. It usually refers to the Grades III or IV of the modified Cormack–Lehane scale \[[21](/article/10.1007/s00405-020-06112-6#ref-CR21 "Rao KVN, Dhatchinamoorthi D, Nandhakumar A, Selvarajan N, Akula HR, Thiruvenkatarajan V (2018) Validity of thyromental height test as a predictor of difficult laryngoscopy: a prospective evaluation comparing modified Mallampati score, interincisor gap, thyromental distance, neck circumference, and neck extension. Indian J Anaesth 62:603–608")\]. According to Schnittker et al. \[[22](/article/10.1007/s00405-020-06112-6#ref-CR22 "Schnittker R, Marshall SD, Berecki-Gisolf J (2020) Patient and surgery factors associated with the incidence of failed and difficult intubation. Anaesthesia 75:756–766")\], the difficult intubation rate is generally in between 0.43 and 0.52% of patients, and in 2% of these selected unfavorable cases, the procedures can fail. As a consequence, if a ‘cannot intubate cannot ventilate’ scenario unfolds, airway must be secured by emergent surgery (tracheostomy or cricothyrotomy), under suboptimal conditions with the ensuing risk of large scale viral aerosolization and severe airway damage. To try to predict beforehand these difficulties, different factors have been considered through the years, using various scoring systems, such as the modified Mallampati score, or trying to quantify a number of anatomical landmarks alone or in combination (i.e. thyromental distance, sternomental distance, thyromental height test, body mass index, gender, and age) \[[21](#ref-CR21 "Rao KVN, Dhatchinamoorthi D, Nandhakumar A, Selvarajan N, Akula HR, Thiruvenkatarajan V (2018) Validity of thyromental height test as a predictor of difficult laryngoscopy: a prospective evaluation comparing modified Mallampati score, interincisor gap, thyromental distance, neck circumference, and neck extension. Indian J Anaesth 62:603–608"),[22](#ref-CR22 "Schnittker R, Marshall SD, Berecki-Gisolf J (2020) Patient and surgery factors associated with the incidence of failed and difficult intubation. Anaesthesia 75:756–766"),[23](#ref-CR23 "Nasa VK, Kamath SS (2014) Risk factors assessment of the difficult intubation using Intubation Difficulty Scale (IDS). J Clin Diagn Res 8:GC01–GC03"),[24](/article/10.1007/s00405-020-06112-6#ref-CR24 "Myers LA, Gallet CG, Kolb LJ, Lohse CM, Russi CS (2016) Determinants of success and failure in prehospital endotracheal intubation. West J Emerg Med 17:640–647")\]. Nonetheless, up to date, there is no universally recognized objective algorithm that can per se identify a difficult intubation scenario with a sufficiently high sensitivity and specificity. Only the anesthesiologist’s experience, after a comprehensive patient’s evaluation taking into consideration all the available data, can possibly foresee a potentially difficult endotracheal intubation. Moreover, a number of devices (i.e. GlideScope or transnasal fiberoptic endoscopy) are now available to help anesthesiologists, emergency care, and ICU physicians in such a difficult situation, certainly improving the odds of a successful intubation. However, some of these tools may increase the risk of airborne contamination of HCPs. For this reason, in a COVID-19 pandemic scenario, guidelines from the British Difficult Airway Society, the Association of Anaesthetists, the Intensive Care Society, the Faculty of Intensive Care Medicine, and the Royal College of Anaesthetists \[[18](/article/10.1007/s00405-020-06112-6#ref-CR18 "Cook TM, El-Boghdadly K, McGuire B, McNarry AF, Patel A, Higgs A (2020) Consensus guidelines for managing the airway in patients with COVID-19. Anaesthesia 75:785–799")\] recommend to always wear proper personal protective equipment (PPE), and to use the larger cuffed tube possible (7.0–8.0 mm internal diameter for women and 8.0–9.0 mm for men), inflating the cuff to seal the airway before starting ventilation. Similar guidelines from different countries have followed in the last 2 months, substantially confirming the above-mentioned caveat.In daily clinical practice, acute laryngeal injury may take place as a consequence of endotracheal intubation [25]. For obvious reasons, use of large caliber tubes exposes the patient to an endolaryngeal (especially at the level of the posterior commissure and subglottis) and/or endotracheal damage, in particular whenever the intubation should be prolonged in time. Moreover, it is well known that poor monitoring of tracheal tube cuff pressure, with undue overinflation, may result in further ischemic damage to the airway mucosa (Fig. 1). Careful use of a manometer is recommended to keep safe cuff pressure values between 20 and 30 cm H2O [26,27,28]. When the cuff pressure reaches 50 mmHg for 15 min, ischemic injury to the tracheal mucosa invariably occurs. It is possible to find a correlation between excessive tube cuff pressure and presence of tracheal pain, hoarseness, sore throat, and blood-streaked expectoration. However, there is no good correlation between the degree of mucosal damage and the severity of patients’ symptoms, since they are always subjective and difficult to collect [28]. The same injury can occur in the larynx, due to the fact that the endolaryngeal tube lays on the posterior aspect of the larynx, causing a chronic pressure on the crico-arytenoid joints, posterior commissure, and cricoid plate. The mucosal ischemic process may lead to progressive ulceration, possibly causing perichondritis, chondritis and, finally, chondronecrosis and airway malacia or perforation. Ulceration at the level of the vocal processes of the arytenoid cartilages can also cause granulomas, occurring within days to weeks after extubation. If bilaterally present, and associated to a posterior commissure ulcerative process, these lesions may merge and evolve into a posterior glottic web which, combining with uni- or bilateral crico-arytenoid fixation, represents the most difficult type of airway stenosis to be successfully managed (Fig. 1a, b). On the top of this, we currently do not fully appreciate the real role of COVID-19-induced laryngitis and laryngeal edema in the context of prolonged endotracheal intubation [[19](/article/10.1007/s00405-020-06112-6#ref-CR19 "McGrath BA, Wallace S, Goswamy J (2020) Laryngeal oedema associated with COVID-19 complicating airway management. Anaesthesia. https://doi.org/10.1111/anae.15092
(Published online ahead of print, 2020 Apr 17)")\]. Only large cohorts of prospectively followed patients will be able to ascertain the possible role of such a pathologic condition on long-term outcomes of the airway managed in the ICU.Fig. 1
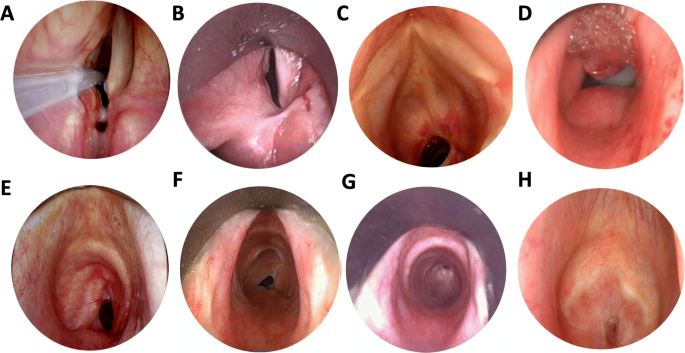
Different patterns of LTS associated with endotracheal intubation and tracheostomy placement. a Bilateral vocal fold immobility caused by still inflamed posterior glottic web. b Same condition due to a mature posterior glottic and inter-arytenoid stenosis. c Cicatricial stenosis at the junction between the cricoid and trachea due to long-term intubation and tracheostomy. d Tracheostomy-related suprastomal collapse. e Suprastomal contracture and tracheal stenosis (so called “lambdoid deformity”). f, g Tracheal stenoses resulting from tracheostomy cuff injury at different levels of the airay. h Complete (grade IV) LTS
The degree and depth of injury mainly depends on duration of intubation, size of tracheal tube, depth of sedation, patient’s general conditions (with cardiovascular diseases, diabetes, and obesity playing an ominous role), and superimposing local infections. This has been commonly described after prolonged mechanical ventilation in the supine position. However, to the best of our knowledge, no precise description on what happens to the laryngotracheal junction of COVID-19 patients ventilated for prolonged time in prone position has been so far produced. In every case, it is always of utmost importance to diagnose and treat these changes as soon as possible to prevent the stabilization of such conditions into irreversible sequelae [[29](/article/10.1007/s00405-020-06112-6#ref-CR29 "Mehel DM, Özdemir D, Çelebi M, Aydemir S, Akgül G, Özgür A (2020) Classification of laryngeal injury in patients with prolonged intubation and to determine the factors that cause the injury. Am J Otolaryngol. https://doi.org/10.1016/j.amjoto.2020.102432
(Published online ahead of print, 2020 Feb 17)")\].As far as the modalities of tracheostomy is concerned, we are lacking prospective randomized clinical trials comparing different surgical techniques like open tracheostomy vs. various types of percutaneous approaches. However, in a COVID-19 scenario, open tracheostomy seems to pose reduced hazards to the HCPs due to the quicker airway entry and lesser aerosolization [[8](/article/10.1007/s00405-020-06112-6#ref-CR8 "Tay JK, Khoo ML, Loh WS (2020) Surgical considerations for tracheostomy during the COVID-19 pandemic: lessons learned from the Severe Acute Respiratory Syndrome outbreak. JAMA Otolaryngol Head Neck Surg. https://doi.org/10.1001/jamaoto.2020.0764
(Published online ahead of print, 2020 Mar 31)"), [14](/article/10.1007/s00405-020-06112-6#ref-CR14 "Sommer DD, Engels PT, Weitzel EK et al (2020) Recommendations from the CSO-HNS taskforce on performance of tracheotomy during the COVID-19 pandemic. J Otolaryngol Head Neck Surg 49(1):23.
https://doi.org/10.1186/s40463-020-00414-9
")\]. Apart from the proper use of PPE ranging from face shields to powered air-purifying respirators, surgical airway establishment should be performed at bedside to avoid unnecessary transport of patients from ICU to the surgical theatre and vice versa. Surgical team should be reduced to a minimum and waste disposal and/or decontamination of equipment used during surgery applied to minimize the risk of environmental contamination. Common to every surgical or endoscopic attempt to create an artificial airway should be the intent of entering the trachea at the level of the first rings, creating the least disruption as possible in terms of number of rings damaged during tracheal opening and cannula positioning. The smallest possible tracheostomy cannula should be inserted, always bearing in mind the body habitus, neck morphology, and clinical conditions of a given patient. Moreover, thick secretions and the need for frequent bronchoscopies to clear the distal airway from mucus plugging may initially prompt to use larger cannula. This, however, should be reduced in size as soon as safe. Appropriate antibiotics and careful medication of the stoma would subsequently prevent superinfection with potential drawbacks, as described above.After patient’s extubation or decannulation, a few days window period is needed before considering definitive stabilization of the patient’s respiratory conditions. Usually, LTS does not manifest itself in this time frame but, rather, after ICU discharge, frequently when the patient is already at home, and not before the third–fourth week or more after normal respiratory conditions re-establish [30].
Early diagnosis of airway stenosis in COVID-19 patients
Every patient with an history of COVID-19-related ICU stay should be followed after discharge by an otolaryngologist or other airway specialist to proactively diagnose early complications at the level of the larynx and trachea. Systemic and topical medications, local debridement, endoscopic dilatations or even just surveillance of subclinical conditions may play a fundamental role in avoiding major airway problems to be diagnosed later only after admission in an Emergency Room (ER) for acute dyspnea. As a consequence of the aforementioned potential complications related to long-term endotracheal intubation and tracheostomy in the upcoming months, the medical community must be prepared to face a rise in the number of patients arriving at our attention due to worsening breathless on exertion and at rest, variously associated to hoarseness, stridor, dry cough, and swallowing problems. These are the most common symptoms of presentation of benign LTS, usually well known to every otolaryngologist. Nevertheless, to maintain a low threshold of suspicion regarding such a diagnosis, we must also elicit such a feeling of urgency among general practitioners, internists, pulmonologists, ER specialists, physiotherapists, and other welfare workers seeing patients who have been exposed to COVID-19-related intubation. Prompt referral of patients to tertiary centers with specific expertise in proper evaluation and treatment of LTS should follow. Of utmost importance is trying to avoid as much as possible that LTS be misdiagnosed as asthma or other pulmonary conditions causing dyspnea, thus retarding initiation of the appropriate diagnostic and therapeutic processes. In this sense, one of the most common and useful first-line diagnostic tool, available also in non-specialist clinical settings, is represented by routine lung function tests. It has been demonstrated that the expiratory disproportion index, defined as the ratio of forced expiratory volume in 1 s to peak expiratory flow rate, has a great clinical utility in differentiating LTS from other respiratory diseases [31, 32]. Moreover, its simplicity and non-invasiveness are particularly welcomed in a COVID-19-related LTS screening, before referral to airway specialists for a more detailed evaluation of the underlying condition.
To identify the best therapeutic option for acquired LTS, an adequate diagnostic work-up should include a thorough preoperative endoscopic and radiologic assessment, associated with an in-depth intraoperative airway evaluation [33]. An accurate endoscopy provides almost all of the required information; details must be gathered on vocal fold mobility, residual airway inflammation and/or infection, cranio-caudal extent of mature scar tissue (with measurement of degree of LTS and description or video-documentation of the sites involved), presence of tracheal damage related to the previous or present stoma/cannula, or secondary airway lesions. Other clinical conditions such as swallowing difficulties with or without chronic aspiration, obstructive sleep apnea-related issues, severe gastro-esophageal reflux, and eosinophilic esophagitis must be taken into consideration.
Thorough awake transnasal and/or transoral videolaryngoscopy using flexible and rigid scopes should always be performed first. Together with flexible bronchoscopy, it allows gathering the necessary dynamic information on laryngeal mobility, swallowing function, and malacia at the level of the tracheostomy site or distal airway. If LTS is apparent, this step should be followed by airway evaluation under general anesthesia to complement the previous picture with the static information needed. In such a situation, to complete the endoscopic diagnostic work-up and have a better visualization of the pharyngo-larynx and subglottis, a suspension laryngoscopy may be of great help. The use of rigid 0° and angled telescopes allows to correctly evaluate the site, degree, and length of LTS [33, 34]. Special issues of interest should include differentiating between unilateral vocal cord palsy vs. arytenoid fixation and/or subluxation, and bilateral vocal cords palsy vs. posterior commissure stenosis. Manipulation of arytenoids and vocal cords during the procedure using a Lindholm vocal cords retractor and angulated probes greatly assists the surgeon in diagnosing the exact cause of vocal cord(s) immobility (recurrent nerve palsy vs. cricoarytenoid joint ankylosis).
CT scan of the larynx and trachea (more rarely an MR) can be complementary in evaluating the length of LTS in case of complete (Grade IV) airway obstruction (Fig. 1h) and to get a deeper insight of an altered laryngotracheal framework due to its deformity, fracture or collapse [[8](/article/10.1007/s00405-020-06112-6#ref-CR8 "Tay JK, Khoo ML, Loh WS (2020) Surgical considerations for tracheostomy during the COVID-19 pandemic: lessons learned from the Severe Acute Respiratory Syndrome outbreak. JAMA Otolaryngol Head Neck Surg. https://doi.org/10.1001/jamaoto.2020.0764
(Published online ahead of print, 2020 Mar 31)")\].As an ancillary consideration in a post-COVID-19 clinical scenario, among the potential comorbidities of the patient, pulmonary functions should be thoroughly evaluated in a multidisciplinary environment, and preoperatively considered during appropriate boards with pulmonologists and anesthesiologists. A bronchoalveolar lavage should be considered to definitively rule out residual SARS-CoV-2 infection (in case of recent COVID-19 hospitalization), while obtaining bacterial culture and antibiotic sensitivity testing.
Treatment strategies
The majority of patients with airway-related symptoms after COVID-19 management will present to the attention of otolaryngologists with incipient LTS as a result of acute or subacute post-intubation/post-tracheostomy airway narrowing, with various degrees of mucosal edema, ulcerations, fibrin, and florid granulation tissue. Early diagnosis and treatment of these conditions by gentle debridement, topical application/injection of corticosteroids, and systemic use of antibiotics and anti-inflammatory drugs, when needed, will help in prevention of excessive scar tissue formation. Most importantly, the final goal of such an initial clinical evaluation and therapeutic management is to avoid as much as possible a tracheostomy or redo-tracheostomy with further damage to the airway framework [33]. As a temporary measure to get a partial relief from dyspnea, endoscopic removal of granulation tissue, dilatations by balloon, bougies or rigid bronchoscopic instrumentation, and steroid injection may be applied. A close cooperation with interventional pneumologists is, in this sense, of paramount importance and sometimes allows bridging the gap between an ER admittance and definitive treatment. However, if absolutely necessary, tracheostomy should be performed into the already damaged and stenosed crico-tracheal tract not to further compromise the adjacent healthy tracheal rings.
After completion of the above-mentioned careful diagnostic work-up, the choice between an endoscopic or open-neck approach to the LTS must be made. As a general rule, purely intrinsic, short (around 1 cm), low-grade stenoses, limited to just one subsite of the airway, may benefit from endoscopic treatments, such as laser radial incisions or balloon dilatation, alone or in combination [33, 35, 36]. These maneuvers are usually well tolerated even by heavily comorbid patients, may be repeated and, if adequately performed, do not cause additional harm. Moreover, as already mentioned, they can play a temporary and symptomatic role while waiting for definitive open surgery. In selected patients with extreme comorbidities (obesity, advanced age, post-COVID-19 severe cardiopulmonary conditions or morbid ICU polyneuropathy) in whom extensive surgery and complex postoperative course might represent an overshooting, palliative care could be considered by positioning an endoluminal stent or, if present, leaving the tracheostomy in situ.
On the other hand, long, high-grade, and complex LTS involving more than one subsites, especially when associated with airway malacia, major laryngeal framework alterations or prior failed endoscopic attempts, can benefit from open-neck surgical techniques. While these can range from laryngotracheal reconstruction with cartilage graft augmentation to (crico-) tracheal resection with end-to-end anastomosis, defining the pros and cons of each of these options is beyond the scope of the present communication. As a general rule, in recent years, a paradigm shift towards a more liberal use of airway circumferential resection and anastomosis techniques has been documented, with reported higher decannulation rates, and lower need for redo-endoscopic or open procedures [37]. For sure, they represent much more demanding surgical procedures, and the overall general conditions of the patients to be treated in such a way must be adequately assessed. Moreover, in this perspective, a quite delicate issue is represented by the anatomy and function of the posterior larynx, potentially affected by long-term intubation as mentioned above (Fig. 1a, b). The balance between respiration, swallowing, airway hygiene and protection is the result of a healthy cricoarytenoid complex. Changes at this level may cause problems, not only related to the airway patency, but to its protective function, potentially facilitating aspiration, and increasing risks of pulmonary complications. Therefore, in every respect, LTS extended to the posterior commissure and inter-arytenoids area represents the most difficult scenario be effectively solved by every kind of surgical procedure.
Conclusions
It is highly probable that in the future months and years, otolaryngologists will be called to manage an increasing number of LTS due to the worldwide emerging issues related to the COVID-19 pandemic. Apart from every attempt to prevent such an airway complication starting from a good team work in the ICUs, a low threshold of doubt should be always maintained among general practitioners, ER physicians, and other medical professionals to straightforward address these patients to the attention of dedicated tertiary centers with an adequate expertise in the field of airway surgery. Comprehensive diagnostic work-up and state-of-art surgical techniques may efficiently solve the majority of these conditions either by endoscopic or open-neck approaches. Moreover, centralizing the management of LTS represents a unique opportunity for optimizing resources as well as trying to understand if such a cluster of patients presents any specific COVID-19-related clinical or epidemiological features as a consequence of prolonged ICU intubation and/or tracheostomy.
References
- Guan WJ, Ni ZY, Hu Y et al (2020) Clinical characteristics of Coronavirus disease 2019 in China. N Engl J Med 382:1708–1720
Article CAS Google Scholar - Wu Z, McGoogan JM (2020) Characteristics of and important lessons from the Coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72314 cases from the Chinese Center for Disease Control and Prevention. JAMA. https://doi.org/10.1001/jama.2020.2648(Published online ahead of print, 2020 Feb 24)
Article PubMed PubMed Central Google Scholar - Huang C, Wang Y, Li X et al (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395:497–506
Article CAS Google Scholar - Wang D, Hu B, Hu C et al (2020) Clinical characteristics of 138 hospitalized patients with 2019 novel Coronavirus-infected pneumonia in Wuhan. JAMA 323:1061–1069
Article CAS Google Scholar - Kowalski LP, Sanabria A, Ridge JA et al (2020) COVID-19 pandemic: Effects and evidence-based recommendations for otolaryngology and head and neck surgery practice. Head Neck. https://doi.org/10.1002/hed.26164(Published online ahead of print, 2020 Apr 9)
Article PubMed PubMed Central Google Scholar - Phua J, Weng L, Ling L et al (2020) Intensive care management of Coronavirus disease 2019 (COVID-19): challenges and recommendations. Lancet Respir Med 8:506–517
Article CAS Google Scholar - Grasselli G, Zangrillo A, Zanella A et al (2020) Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy Region, Italy. JAMA 323:1574–1581
Article CAS Google Scholar - Tay JK, Khoo ML, Loh WS (2020) Surgical considerations for tracheostomy during the COVID-19 pandemic: lessons learned from the Severe Acute Respiratory Syndrome outbreak. JAMA Otolaryngol Head Neck Surg. https://doi.org/10.1001/jamaoto.2020.0764(Published online ahead of print, 2020 Mar 31)
Article PubMed Google Scholar - Freeman BD, Morris PE (2012) Tracheostomy practice in adults with acute respiratory failure. Crit Care Med 40:2890–2896
Article Google Scholar - Siempos II, Ntaidou TK, Filippidis FT, Choi AMK (2015) Effect of early versus late or no tracheostomy on mortality and pneumonia of critically ill patients receiving mechanical ventilation: a systematic review and meta-analysis. Lancet Respir Med 3:150–158
Article Google Scholar - Cheung NH, Napolitano LM (2014) Tracheostomy: epidemiology, indications, timing, technique, and outcomes. Respir Care 59:895–899
Article Google Scholar - Huang H, Li Y, Ariani F, Chen X, Lin J (2014) Timing of tracheostomy in critically ill patients: a meta-analysis. PLoS ONE 9:e92981
Article Google Scholar - Lin WC, Chen CW, Wang JD, Tsai LM (2015) Is tracheostomy a better choice than translaryngeal intubation for critically ill patients requiring mechanical ventilation for more than 14 days? A comparison of short-term outcomes. BMC Anesthesiol 15:181
Article Google Scholar - Sommer DD, Engels PT, Weitzel EK et al (2020) Recommendations from the CSO-HNS taskforce on performance of tracheotomy during the COVID-19 pandemic. J Otolaryngol Head Neck Surg 49(1):23. https://doi.org/10.1186/s40463-020-00414-9
Article CAS PubMed PubMed Central Google Scholar - To KK, Tsang OT, Leung WS et al (2020) Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: an observational cohort study. Lancet Infect Dis 20:565–574
Article CAS Google Scholar - Fiz I, Monnier P, Koelmel JC et al (2019) Multicentric study applying the European Laryngological Society classification of benign laryngotracheal stenosis in adults treated by tracheal or cricotracheal resection and anastomosis. Laryngoscope. https://doi.org/10.1002/lary.28274(Published online ahead of print, 2019 Sep 11)
Article PubMed Google Scholar - Nikolovski N, Kopacheva-Barsova G, Pejkovska A (2019) Laryngotracheal stenosis: a retrospective analysis of their aetiology, diagnose and treatment. Open Access Maced J Med Sci 7:1649–1656
Article Google Scholar - Cook TM, El-Boghdadly K, McGuire B, McNarry AF, Patel A, Higgs A (2020) Consensus guidelines for managing the airway in patients with COVID-19. Anaesthesia 75:785–799
Article CAS Google Scholar - McGrath BA, Wallace S, Goswamy J (2020) Laryngeal oedema associated with COVID-19 complicating airway management. Anaesthesia. https://doi.org/10.1111/anae.15092(Published online ahead of print, 2020 Apr 17)
Article PubMed PubMed Central Google Scholar - Barjaktarevic I, Esquinas AM, West FM, Albores J, Berlin D (2017) Noninvasive ventilation in difficult endotracheal intubation: systematic and review analysis. Anaesthesiol Intensive Ther 49:294–302
PubMed Google Scholar - Rao KVN, Dhatchinamoorthi D, Nandhakumar A, Selvarajan N, Akula HR, Thiruvenkatarajan V (2018) Validity of thyromental height test as a predictor of difficult laryngoscopy: a prospective evaluation comparing modified Mallampati score, interincisor gap, thyromental distance, neck circumference, and neck extension. Indian J Anaesth 62:603–608
Article Google Scholar - Schnittker R, Marshall SD, Berecki-Gisolf J (2020) Patient and surgery factors associated with the incidence of failed and difficult intubation. Anaesthesia 75:756–766
Article CAS Google Scholar - Nasa VK, Kamath SS (2014) Risk factors assessment of the difficult intubation using Intubation Difficulty Scale (IDS). J Clin Diagn Res 8:GC01–GC03
Google Scholar - Myers LA, Gallet CG, Kolb LJ, Lohse CM, Russi CS (2016) Determinants of success and failure in prehospital endotracheal intubation. West J Emerg Med 17:640–647
Article Google Scholar - Shinn JR, Kimura KS, Campbell BR et al (2019) Incidence and outcomes of acute laryngeal injury after prolonged mechanical ventilation. Crit Care Med 47:1699–1706
Article Google Scholar - Sengupta P, Sessler DI, Maglinger P et al (2004) Endotracheal tube cuff pressure in three hospitals, and the volume required to produce an appropriate cuff pressure. BMC Anesthesiol 4:4–9
Article Google Scholar - Seegobin RD, Van Hasselt GL (1984) Endotracheal cuff pressure and tracheal mucosal blood flow: endoscopic study of effects of four large volume cuffs. Br Med J 288:965–968
Article CAS Google Scholar - Liu J, Zhang X, Gong W et al (2010) Correlations between controlled endotracheal tube cuff pressure and postprocedural complications: a multicenter study. Anesth Analg 111:1133–1137
Article Google Scholar - Mehel DM, Özdemir D, Çelebi M, Aydemir S, Akgül G, Özgür A (2020) Classification of laryngeal injury in patients with prolonged intubation and to determine the factors that cause the injury. Am J Otolaryngol. https://doi.org/10.1016/j.amjoto.2020.102432(Published online ahead of print, 2020 Feb 17)
Article PubMed Google Scholar - de Kleijn BJ, Wedman J, Zijlstra JG, Dikkers FG, van der Laan BFAM (2019) Short- and long-term complications of surgical and percutaneous dilatation tracheotomies: a large single-center retrospective cohort study. Eur Arch Otorhinolaryngol 276:1823–1828
Article Google Scholar - Nouraei SA, Winterborn C, Nouraei SM et al (2007) Quantifying the physiology of laryngotracheal stenosis: changes in pulmonary dynamics in response to graded extrathoracic resistive loading. Laryngoscope 117:581–588
Article Google Scholar - Nouraei SA, Nouraei SM, Patel A et al (2013) Diagnosis of laryngotracheal stenosis from routine pulmonary physiology using the Expiratory Disproportion Index. Laryngoscope 123:3099–3104
Article Google Scholar - Monnier P, Dikkers FG, Eckel H et al (2015) Preoperative assessment and classification of benign laryngotracheal stenosis: a consensus paper of the European Laryngological Society. Eur Arch Otorhinolaryngol 272:2885–2896
Article Google Scholar - Myer CM, O’Connor DM, Cotton RT (1994) Proposed grading system for subglottic stenosis based on endotracheal tube sizes. Ann Otol Rhinol Laryngol 103:319–323
Article Google Scholar - Kocdor P, Siegel ER, Suen JY, Richter G, Tulunay-Ugur OE (2016) Comorbidities and factors associated with endoscopic surgical outcomes in adult laryngotracheal stenosis. Eur Arch Otorhinolaryngol 273:419–424
Article Google Scholar - Bogdasarian RS, Olson NR (1980) Posterior glottic laryngeal stenosis. Otolaryngol Head Neck Surg 88:765–772
Article CAS Google Scholar - Lewis S, Earley M, Rosenfeld R, Silverman J (2017) Systematic review for surgical treatment of adult and adolescent laryngotracheal stenosis. Laryngoscope 127:191–198
Article Google Scholar