Roles of Fc receptors in autoimmunity (original) (raw)
Autoimmune diseases are caused by immune responses to self-antigens in various tissues, and they can be classified broadly as being either antibody mediated or T-cell mediated. Rheumatoid arthritis, for example, involves joint inflammation and destruction that is caused by autoimmune antibody responses to unknown synovial antigens. By contrast, patients with type-1 diabetes develop insulitis as a result of T-cell infiltration and destruction of the pancreatic islets. Autoimmune responses are thought to have the same basis as adaptive immune responses to foreign antigens, in which antigen-specific T cells are activated by antigen-presenting cells. It is not known what causes the breakdown of CENTRAL and/or PERIPHERAL TOLERANCE to trigger autoreactive lymphocytes, but both environmental and genetic factors, such as MHC genotype, are thought to be crucial. Despite the difficulty of identifying genetic susceptibility factors in autoimmune patients, recent work has begun to focus on possible mutation of the FcγRIIB gene, which encodes a unique inhibitory Fc receptor (FcR) for immunoglobulin G. Why do such efforts make sense? In this review, I outline how the pivotal FcR control system might regulate the development of autoimmunity. This model is based on recent studies of autoimmune diseases in mice, in which activating FcRs have been shown to promote disease development, whereas the inhibitory FcR FcγRIIB maintains peripheral tolerance. In addition to antibody-mediated autoimmune diseases, I discuss the possible involvement of FcRs in T-cell-mediated autoimmune diseases.
Fc-receptor functions
Even before the identification of cell-surface receptors for the Fc of antibodies, it was well known that passively administered antibodies can activate or suppress immune responses1. So, antibody- or Fc-mediated activation and suppression have been studied since the 1960s2, which led to the identification of FcRs on various immune cells, such as B cells3. During the past decade, we have learned much more about FcRs at the molecular level and have shown that they are not simply cell-surface molecules that bind immunoglobulins — they can initiate various biological functions that can be classified into three main categories.
First, the most prominent function of FcRs, which has been discovered over the past several years, is the positive and negative regulation of immune-cell responses, such as the proliferation of B cells, phagocytosis by macrophages and degranulation of mast cells (Fig. 1a). Engagement of activating-type FcRs triggers many biological functions, such as phagocytosis, cytolysis, degranulation and the transcriptional activation of cytokine-encoding genes, which initiates inflammatory cascades. Simultaneously, in most cases, engagement of the unique inhibitory FcR, FcγRIIB, down-modulates these effector responses. Most of the activating-type FcRs associate with the Fc RECEPTOR COMMON γ-CHAIN (FcRγ), which contains an immunoreceptor tyrosine-based activation motif (ITAM) (Fig. 1a). By contrast, FcγRIIB is a single-chain molecule that contains an immunoreceptor tyrosine-based inhibitory motif (ITIM) in its cytoplasmic domain. FcγRIIB is expressed ubiquitously on immune cells — including B cells, macrophages and mast cells — and it can inhibit various cellular functions, such as B-cell activation/proliferation and mast-cell degranulation. This ITAM–ITIM regulatory pair is now recognized as a typical tool that is used frequently in the immune system.
Figure 1: Main functions of Fc receptors.
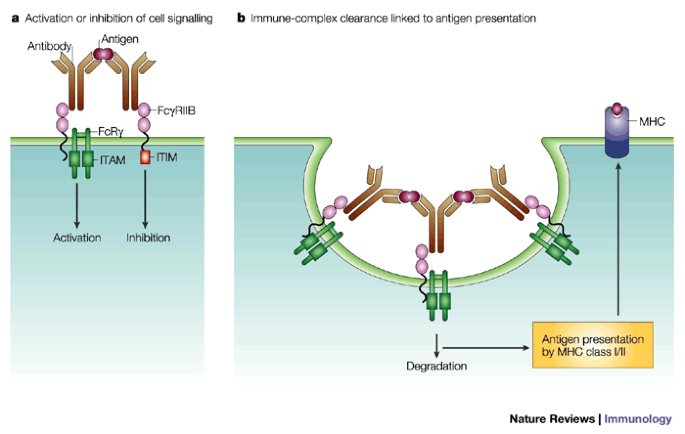
a | Positive and negative regulation of cellular signalling. Fc receptors (FcRs) are expressed by various cells of the immune system and have a central role in controlling immune responses after interaction with antigen–antibody complexes. The activation cascade through FcR common γ-chain (FcRγ)-associating FcRs results in cellular activation, which leads to phagocytosis, antibody-dependent cellular cytotoxicity, superoxide generation and the production and release of cytokines and pro-inflammatory mediators. By contrast, FcγRIIB contains an immunoreceptor tyrosine-based inhibitory motif (ITIM), and it mediates the inhibition of the immunoreceptor tyrosine-based activation motif (ITAM)-induced activation cascade. b | Clearance of immune complexes, and MHC class-I- and class-II-restricted antigen presentation. After phagocytosis or endocytosis by an FcR-mediated process, the immune complexes are efficiently broken down intracellularly, followed by antigen presentation in a class-I- and class-II-restricted manner.
The second important function is the uptake of immune complexes (ICs) (Fig. 1b). FcRs can trigger the internalization of captured ICs, which leads to degradation of the antigen–antibody complexes, as well as directing the antigenic peptides to the MHC class I or class II antigen-presentation pathway4. Macrophages take up and degrade ICs efficiently, whereas dendritic cells are more specialized for antigen presentation. The degradation of antigen is, of course, important for its elimination, which is a central purpose of the immune system. It is believed that defects in IC clearance are linked to the initiation of autoimmune diseases, such as SYSTEMIC LUPUS ERYTHEMATOSUS (SLE). Importantly, recent findings indicate that antigen presentation is much more efficient if the IC is internalized by FcRs than by non-specific uptake mechanisms, such as fluid-phase pinocytosis4.
Third, the neonatal FcR for IgG, FcRn, and the polymeric immunoglobulin receptor (poly-IgR) can transfer antibodies transcellularly. These receptors are important for the transplacental transfer of maternal IgG and the transfer of IgA to mucosal surfaces, respectively, but they are not thought to have immunoregulatory roles.
In addition to these three main functions of FcRs, compelling evidence exists that some types of FcR can be released into the blood in a soluble form and that these soluble FcRs can modulate immune responses5. For example, a soluble form of mouse FcγRIIb can suppress primary and secondary in vitro antibody responses. However, the physiological relevance of this phenomenon to susceptibility to autoimmune disease is not known and will not be discussed here. It has been proposed also that some FcRs can modify lymphocyte differentiation6,7,8. In spite of the large body of accumulated knowledge about the possible involvement of FcRs in cellular developmental pathways, more precise information is still required from studies of FcR-deficient mice.
This review deals mainly with the first two aspects of FcR function — positive and negative regulation of cellular signalling, and IC clearance and antigen presentation — and their relation to autoimmune diseases.
Recent advances in our knowledge of the regulation of mouse hypersensitivity responses by FcRs, which are the result of observations in FcR-deficient mice, might also provide a basis for understanding the role of FcRs in the development or suppression of antibody-mediated autoimmunity. Using FcRγ-, FcγRI (CD64)- or FcγRIII (CD16)-deficient mice, the mechanisms of initiating hypersensitivity and inflammatory cascades have been re-evaluated. It was shown that the binding of IgG-containing ICs to FcγRI and FcγRIII on effector cells are pivotal events that lead to IgG-induced anaphylaxis and inflammation9,10,11,12,13,14,15,16,17, such as the skin ARTHUS REACTION10,13,14. By contrast, suppression of these ITAM-initiated activation events through ITIM-bearing FcγRIIb is crucial for maintaining homeostasis and controlling the inappropriate activation of effector cells, such as mast cells15,18. Further study of these activating and inhibitory cascades, as well as the detailed physiological roles of FcγRs, will indicate ways in which they might prevent or promote autoimmunity, as discussed later.
Structural features of Fc receptors
FcR genes in humans and mice. Most FcRs are members of the immunoglobulin superfamily of proteins and are found on many haematopoietic lineages (Table 1). The genetic organization and molecular structures of FcRs have been reviewed extensively elsewhere19. Briefly, eight genes have been identified that encode human FcγRs — three genes for the high-affinity IgG receptor FcγRI ( FcγRIA , FcγRIB and FcγRIC ), and five genes for the low-affinity IgG receptors FcγRII ( FcγRIIA , FcγRIIB and FcγRIIC ) and FcγRIII ( FcγRIIIA and FcγRIIIB ) (Table 1). The low-affinity FcγR genes and the gene that encodes FcRγ are clustered on human chromosome 1q23. This region of 1q23 is syntenic with mouse chromosome 1 (92–94 cM), on which single genes for these receptors are located. The three FcγRI genes in humans map to chromosome 1q21; the mouse FcγRI gene has been mapped to chromosome 3 (45.2 cM). The human FcαR gene is located within the LEUKOCYTE-RECEPTOR COMPLEX (LRC) locus on chromosome 19q13.4 — where genes that encode many leukocyte receptors, such as killer immunoglobulin-like receptors, are located — which indicates that human FcαR might have evolved from a different ancestor to the FcγRs. A mouse counterpart of human FcαR has not been identified. Using expression cloning, Shibuya et al.20 have identified in both mouse and humans a new FcR for both IgM and IgA, called Fcα/μR. It is proposed that Fcα/μR is involved in the primary stages of the immune response to microorganisms. Both of these IgA-binding receptors, FcαR and Fcα/μR, might be involved in IgA nephropathy, which is a common form of glomerulonephritis21,22.
Table 1 Structural overview and cellular expression profiles of Fc receptors
A database screen to identify new FcR-like sequences in the human genome has identified five clones of immunoglobulin-superfamily members, termed FcR homology 1 (FcRH1), FcRH2, FcRH3, FcRH4 and FcRH5 (Refs 23,24) (Table 1). The genes that encode FcRHs are located on chromosome 1q21, in the middle of the FcR genes. The anticipated capacity for both activating and inhibitory function of the cytoplasmic tails of individual FcRH members predicts that they have a dual role in the regulation or modulation of signalling, although the cell-expression profiles at the protein level, as well as the detailed signalling pathways, of these receptors remain to be examined.
FcR structure and ligand binding. Recent studies of FcR crystallographic structures, together with molecular modelling, have provided us with an insight into ligand binding25,26,27. This is best exemplified by the three-dimensional structural model of human IgG1 binding to soluble FcγRIII, in which the extracellular portion of FcγRIII binds one IgG molecule asymmetrically (Box 1). This 1:1 stoichiometry model explains why IgG molecules are unable to trigger FcγR-mediated cellular responses spontaneously in the absence of crosslinking by multivalent antigens.
Of the three main types of FcγR in mice and humans, the high-affinity receptor FcγRI can bind monomeric IgG, whereas the two low-affinity receptors FcγRII and FcγRIII bind IgG in the form of ICs. In mice, FcγRI and FcγRIII trigger cell activation through a common FcRγ that contains an ITAM. By contrast, FcγRIIb — which is the most widely expressed FcR — contains an ITIM, which inhibits ITAM-mediated cellular activation triggered by the binding of antibody or ICs to activating FcRs28,29. FcRγ is not only important for cell activation, but is also necessary for the efficient assembly and cell-surface expression of at least four types of FcR— FcγRI, FcγRIII, FcɛRI and FcαRI — as well as other activating-type receptors, such as paired immunoglobulin-like receptor-A (PIR-A)30. Therefore, deletion of FcRγ results in the combined deficiency of activating-type FcRs (but not FcγRIIa, which does not use FcRγ; Table 1) and other receptors, such as PIR-A. However, we do not know the specific phenotype of PIR-A deficiency that results from the deletion of FcRγ.
Regulation of cell signalling by Fc receptors
Activating signalling by ITAM-containing FcRs. The molecular mechanisms by which clustering of FcγRs triggers or suppresses cell activation are crucial for defence against IgG-complexed antigens and for the development of autoimmune diseases28,31,32. Intracellular SRC-family protein tyrosine kinases are activated by the clustering of activating FcγRs, and they phosphorylate tyrosine residues in the ITAM. The phosphorylated ITAM then serves as a docking site for the SRC-homology 2 (SH2) domain of the cytosolic protein kinase SYK (Fig. 2a). The physical and functional association of SRC-family protein tyrosine kinases, such as LYN and HCK, with FcRγ-associating FcRs and FcγRIIa has been reported33,34. Activating signalling through ITAM-containing FcRs leads to an oxidative burst, cytokine release and phagocytosis by macrophages, antibody-dependent cellular cytotoxicity (ADCC) by natural killer (NK) cells and the degranulation of mast cells. The initiation of inflammatory and destructive responses by these effector cells is believed to be crucial for the development and pathogenesis of autoimmunity.
Figure 2: Signalling mechanisms of ITAM- and ITIM-induced regulatory FcR signalling.
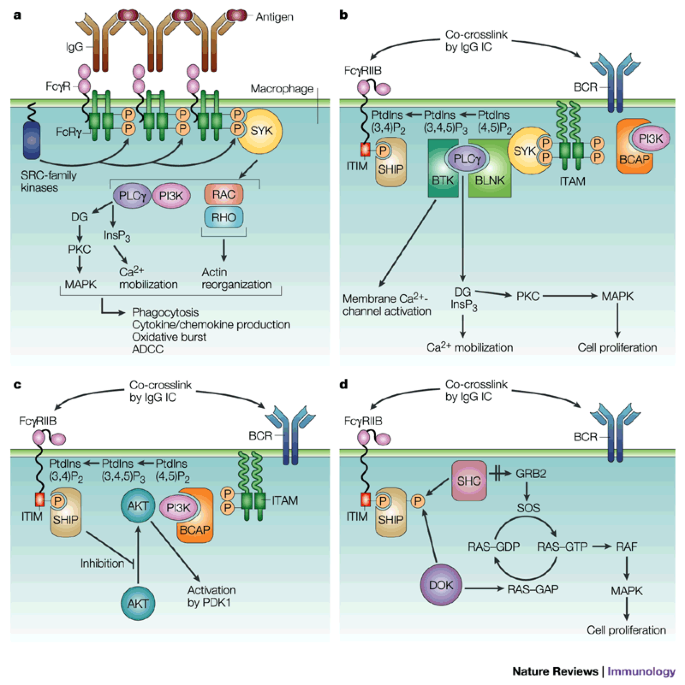
a | Activating signalling by ITAM-containing FcγRs in macrophages. Tyrosine residues in the ITAM become phosphorylated by SRC-family protein kinases, such as SRC, FYN, FGR, HCK and LYN, after crosslinking of cell-surface FcγRs by immunoglobulin-G-containing immune complexes. The downstream events of SYK activation include stimulation of phospholipase Cγ (PLCγ), phosphatidylinositol 3-kinase (PI3K), the cytoskeletal protein paxillin, ERK (mitogen-activated protein kinase; MAPK), and GTPases of the RHO and RAC families, which are involved in reorganization of the actin cytoskeleton. The activation pathway can be inhibited by co-aggregation of FcγRIIB. b | Inhibition of Bruton's tyrosine kinase (BTK) and the PLCγ pathway in B cells after co-crosslinking of B-cell receptor (BCR) and FcγRIIB. The activation of SH2-domain-containing inositol polyphosphate 5′ phosphatase (SHIP) causes hydrolysis of phosphatidylinositol-3,4,5-trisphosphate (PtdIns(3,4,5)P3) to PtdIns(3,4)P2. PtdIns(3,4,5)P3 is the docking site for pleckstrin-homology (PH)-domain-containing proteins, including BTK and PLCγ. BTK and PLCγ cannot be recruited to membrane PtdIns(3,4,5)P3, which blocks Ca2+ influx and protein kinase C (PKC) activation45,46,47. c | The AKT pathway. The anti-apoptotic kinase AKT cannot be recruited to the membrane by binding of its PH domain to PtdIns(3,4,5)P3 in the presence of activated SHIP. The current model of activation of AKT, a serine–threonine kinase, is that AKT is recruited to the membrane, causing a conformational change in AKT, which allows phosphorylation and activation by PDK1. AKT is activated by stimulation through the BCR in a PI3K-dependent manner. An adaptor, BCAP, has been identified as binding to PI3K, and its deletion rendered B cells less responsive to BCR crosslinking, although CD19 phosphorylation might be more important for PI3K activation112. d | RAS–MAPK pathway. Phosphorylated SHIP creates a binding site for the phosphotyrosine-binding (PTB) domains of SHC and DOK, which recruits these molecules to the plasma membrane. DOK becomes tyrosine phosphorylated and recruits RAS–GAP, which catalyses the conversion of RAS–GTP to RAS–GDP, leading to inhibition of the ERK–MAPK pathway. An inactivation study of the DOK gene showed that after BCR crosslinking, DOK suppresses MAPKs and is indispensable for FcγRIIB-mediated suppression of proliferation55. ADCC, antibody-dependent cellular cytotoxicity; DG, diacylglycerol; GRB2, growth-factor-receptor-bound protein 2; IC, immune complex; ITAM, immunoreceptor tyrosine-based activation motif; ITIM, immunoreceptor tyrosine-based inhibitory motif.
Inhibitory signalling by ITIM-containing FcγRIIB. FcγRIIB acts physiologically as a negative regulator of IC-triggered activation, and it might function in vivo to suppress autoimmunity by regulating both B-cell responses and effector-cell functions, such as phagocytosis by macrophages. The inhibitory function of FcγRIIB is characterized best in B cells (Fig. 2b–d), although it has also been shown in other cell types, such as myeloid and monocytic cells35,36. During the late phases of an immune response, ICs composed of IgG and antigen might bind simultaneously to B-cell receptors (BCRs) and FcγRIIB, which are co-expressed by B cells. Co-aggregation of the BCR with FcγRIIB inhibits BCR signalling, which blocks downstream biological responses of the B cell — including activation, antigen presentation, proliferation and antibody production — and might reduce the development of autoimmune disease. The initial event in inhibitory signalling is phosphorylation by the SRC-family kinase LYN of the ITIM tyrosine that is found in the FcγRIIB cytoplasmic tail37. This modification results in the recruitment of SH2-domain-containing phosphatases, predominantly SH2-domain-containing protein tyrosine phosphatase 1 (SHP1), SHP2 and SH2-domain-containing inositol polyphosphate 5′ phosphatase (SHIP)37,38,39,40. SHIP, which is the primary effector of FcγRIIB-mediated inhibition40,41,42,43,44, dephosphorylates phosphoinositides and inositol polyphosphates. Its main in vivo substrate is phosphatidylinositol-3,4,5-trisphosphate — PtdIns(3,4,5)P3 — which is formed by the action of phosphatidylinositol 3-kinase (PI3K). Thereafter, the proposed signalling cascade of inhibition is subdivided into three distinct, but mutually interacting, pathways.
First, SHIP-mediated hydrolysis of PtdIns(3,4,5)P3 leads to impaired membrane translocation of signal-transducing molecules, including Bruton's tyrosine kinase (BTK) and phospholipase-Cγ (PLCγ)45,46,47 (Fig. 2b). BTK is required for the activation of PLCγ and the hydrolysis of PtdIns(4,5)P2, which yields Ins(1,4,5)P3 and diacylglycerol (DAG). So, SHIP inhibits the generation of second messengers — Ins(1,4,5)P3 and DAG — that mediate calcium mobilization and the activation of protein kinase C (PKC), respectively.
Second, the activation of mitogen-activated protein (MAP) kinases and recruitment of the anti-apoptotic kinase AKT are suppressed by the co-aggregation of FcγRIIB with the BCR, which leads to the inhibition of cell proliferation and survival48 (Fig. 2c). AKT activation, itself, is also downregulated by co-crosslinking of the BCR with FcγRIIB49. SHIP-deficient B cells have enhanced proliferation in response to BCR stimulation41,50, and this enhancement is associated with the increased phosphorylation (activation) of both MAP kinases50 and AKT41,50.
Third, SHIP functions as an adaptor protein that binds SHC51 and p62DOK52 (Fig. 2d). The binding of SHIP to FcγRIIB inhibits RAS activation. After tyrosine phosphorylation of the FcγRIIB ITIM, the recruited SHIP is tyrosine phosphorylated and associates with SHC, a RAS-pathway adaptor53. It is proposed that SHIP competes with growth-factor-receptor-bound protein 2 (GRB2)–SOS complexes (which stimulate the RAS activation pathway) for SHC binding, and this is responsible for the observed decrease in RAS-bound GTP. As a result, impaired downstream activation of MAP kinases, and arrest of cell-cycle progression and proliferation occur.
Inhibition of MAP kinases has been attributed also to impaired PLCγ-mediated activation of protein kinase C (PKC)54 (Fig. 2b). Also, p62DOK inhibits the activation of MAP kinases, and it is indispensable for FcγRIIB-mediated suppression of proliferation55. Therefore, FcγRIIB-mediated inhibition of MAP kinases might occur by at least two mechanisms — SHIP linkage to SHC or DOK, and SHIP-mediated enzymatic degradation of PtdIns(3,4,5)P3, which prevents the activation of PKC.
FcγRIIB-mediated inhibition of BCR signalling might be mediated, at least in part, by selective dephosphorylation of CD19, which is a BCR accessory molecule and co-receptor. CD19 dephosphorylation prevents the association of CD19 with PI3K, and this, in turn, leads to termination of Ins(1,4,5)P3 production, intracellular Ca2+ release and Ca2+ influx56. It is speculated that SHP1 is responsible for the observed effects.
FcγRIIB might deliver an apoptotic signal. During the germinal-centre reaction, B cells that express high-affinity BCRs will be selected for antigenic stimulation and cognate T-cell interactions, which are facilitated by the preferential uptake of antigen by these high-affinity BCRs. In the absence of these stimulatory signals, cells that express low-affinity BCRs undergo apoptotic death. At least in vitro, the engagement of FcγRIIB on B cells can generate an apoptotic signal41,57. Crosslinking of FcγRIIB alone was sufficient to induce apoptosis in B cells independent of BCR co-ligation58. Interestingly, this response requires only an intact FcγRIIB transmembrane domain. Therefore, FcγRIIB might be an active determinant in the negative selection of B cells that express low-affinity BCRs. A defect in the negative selection of B cells could be a risk factor for autoimmunity.
Fc-receptor-mediated antigen presentation
One of the crucial features of FcγRs is their ability to enhance antigen presentation of IgG-containing ICs by antigen-presenting cells, such as dendritic cells (DCs) and epidermal Langerhans' cells, which leads to the activation of antigen-specific T cells4,5 (Fig. 1). Indeed, most FcγRs efficiently internalize antigen–antibody complexes and thereby induce the efficient processing of antigens into peptides that are presented by MHC class I and class II molecules in vitro. Importantly, ITAMs and cytosolic effectors of cell signalling determine the endocytic-transport and antigen-presentation capacities of FcγRs4,59. Recent findings indicate that ubiquitylation is required for FcγRIIA-mediated endocytosis, but not for PHAGOCYTOSIS60, which indicates that there are quite different mechanisms for endocytosis and phagocytosis by FcRs, although both of these processes lead to antigen presentation. FcγR-mediated antigen uptake can enhance antigen presentation by DCs to activate CD4+ and CD8+ T cells both in vitro59,61 and in vivo62; this implies that FcγRs have a pivotal role in augmenting humoral and cellular immune responses at the antigen-presentation step, which is an initial phase of the immune response (Fig. 1). In recent studies, targeting antigen to FcγRs on bone-marrow-derived DCs by complexing the antigen (ovalbumin; OVA) with anti-OVA IgG successfully elicited humoral responses that consisted of OVA-specific IgG production in vivo. Antigen-pulsed DCs from wild-type mice, but not from FcγR-deficient mice, could also activate antigen-specific cytotoxic T lymphocytes in vivo, which indicates a pivotal role for FcγRs in the efficient MHC class-I-restricted presentation of exogenous antigens, which is known as CROSS-PRESENTATION59 (K. Akiyama et al., unpublished observations).
Fc-receptor mechanisms in autoimmunity
The development of autoimmune diseases is complex and dependent on many genes and environmental factors. Therefore, animal models are useful for elucidating the genetic control of the various pathways that lead to disease. Mice that are deficient for FcRγ are unable to phagocytose IgG-opsonized particles or to mediate ADCC by NK cells, and they respond poorly to IgE-mediated mast-cell activation9. Mounting evidence indicates that the ITAM-containing FcRs have a role in initiating type I, II and III HYPERSENSITIVITY REACTIONS and anaphylaxis10,11,12,13,14,15,16,17,63,64,65,66,67,68,69. Importantly, FcRγ-deficient mice are resistant to the induction or spontaneous onset of various autoimmune diseases11,12,63,65,66,67, as summarized in Table 2. These results indicate that a wide range of inflammatory and autoimmune diseases — such as vasculitis, glomerulonephritis and AUTOIMMUNE HAEMOLYTIC ANAEMIA (AIHA)— might be mediated by FcγRs and not, as previously thought, primarily by complement factors. It is possible that the complement system mediates mainly innate immune responses, in which the initial interaction of NATURAL ANTIBODIES of the IgM class with pathogens triggers complement-mediated inflammation, whereas FcγR-mediated inflammation, which involves the interaction of IgG-containing ICs with effector cells, can only occur after the establishment of aquired immunity31.
Table 2 In vivo phenotypes of Fc-receptor-deficient mice
In contrast to FcRγ-deficient mice, targeted disruption of FcγRIIb in mice results in various enhanced responses — such as elevated immunoglobulin levels in response to both thymus-dependent and -independent antigens, enhanced passive cutaneous and systemic anaphylaxis reactions in response to antigen challenge15,18, and enhanced IC-mediated inflammatory responses12,66,70 — which indicates that FcγRIIb acts as a negative regulator of humoral responses and IC-triggered activation (Table 2). In particular, FcγRIIb might determine susceptibility to and severity of IC-mediated autoimmune diseases, such as collagen-induced arthritis (CIA)71,72.
Figure 3 illustrates the current view of the whole system of regulation by FcRs in terms of the two main roles of FcRs — regulation of cellular signalling and clearance of ICs linked to antigen presentation. Figure 3 also illustrates four main ways in which FcRs might contribute to the development of autoimmune disease. First, tissue-deposited ICs can cross-link FcRs, causing the release of pro-inflammatory molecules, mainly from neutrophils and macrophages, as seen in CIA and Goodpasture's syndrome (GPS), which will be discussed later. Second, FcR dysfunction can result in systemic autoimmune diseases, such as SLE, owing to the inefficient clearance of IgG-containing ICs. Third, the triggering of FcRs on cytotoxic effector cells, such as macrophages, can lead to the destruction of autoantibody-opsonized cells, such as erythrocytes in AIHA, or platelets in IDIOPATHIC THROMBOCYTIC PURPURA (ITP).
Figure 3: Overall view of activating Fc receptors and inhibitory FcγRIIB, and related autoimmune diseases.
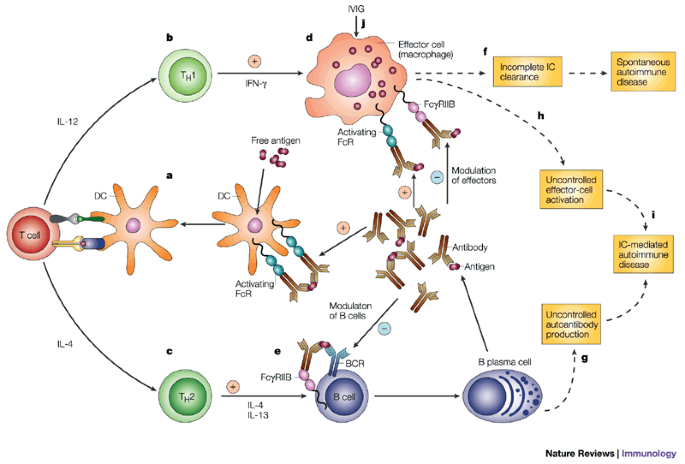
Fc receptors (FcRs) can initiate or augment an immune response at the initial antigen-presentation step (a) by facilitating immune complex (IC) uptake, and can drive cellular (b) and humoral (c) immune responses. In both cascades, FcγRIIB is crucial for inhibiting several activation loops of ITAM-containing FcRs (d,e). In humans, several FcR polymorphisms induce incomplete IC clearance, which leads to the sustained activation of effector cells and provokes IC-induced autoimmune diseases, such as systemic lupus erythematosus (SLE), rheumatoid arthritis (RA) and multiple sclerosis (MS) (f). In mice, FcγRIIb deletion leads to autoantibody production (g) and activation of effector cells (h), which also induce IC-mediated autoimmune diseases (i), such as Goodpasture's syndrome, collagen-induced arthritis and glomerulonephritis. IVIG treatment (j; see also Box 2) results in upregulation of the expression of FcγRIIB on macrophages. FcγRIIB engagement inhibits B-cell antigen presentation113,114. The negative regulation of the antigen-presentation process by FcRs on dendritic cells is not known. DC, dendritic cell; IFN-γ, intereferon-γ; IL, interleukin; ITAM, immunoreceptor tyrosine-based activation motif; IVIG, intravenous immunoglobulin; TH, T helper.
Fourth, FcγRIIB is one of the pivotal elements for controlling the activation of autoreactive B cells — which are often present even in normal individuals — and is important for maintaining peripheral tolerance. Its functional impairment leads directly to IC-induced autoimmune diseases. In relation to this, the extent of downregulation of expression of FcγRIIb in germinal-centre B cells was shown to be inversely related to the upregulation of IgG antibody responses and to correlate well with susceptibility to autoimmune diseases in several mouse strains73,74, which indicates that maintaining the expression level of FcγRIIB, especially in germinal-centre B cells, is important for suppressing the unwanted expansion of autoreactive B-cell populations.
So, FcγRIIB deletion, which leads to marked augmentation of autoantibody production, due to loss of the negative-feedback loop of B-cell regulation, and enhanced effector-cell responses, is sufficient for the onset of induced or spontaneous autoimmune disease, at least in mice (see below and Fig. 3).
Induced autoimmunity
Collagen-induced arthritis. CIA, a model of rheumatoid arthritis in humans, is a chronic inflammatory arthropathy that can be induced in susceptible rodents, such as DBA/1 mice, by immunization with type-II collagen (C-II)75. The development of arthritis is thought to be associated with the synergistic effects of high levels of cell-mediated and humoral immunity to C-II. Susceptibility is controlled by specific MHC class II molecules, such as H2-Aq, that bind defined immunodominant peptides of C-II. Activation of C-II-peptide-specific T cells triggers an immune-mediated cascade that results in inflammatory destruction of the peripheral joints. Many pathways and factors are likely to participate. B-cell-deficient mice do not develop arthritis76, and arthritis can be transferred between mice by hyperimmune anti-C-II serum concentrate77 or polyclonal IgG anti-C-II antibodies78,79.
DBA/1 mice that lack FcRγ are protected from CIA compared with wild-type mice, although both groups produce similar levels of IgG anti-C-II antibodies71 (T. Takai et al., unpublished observations). By contrast, FcγRIIb-deficient DBA/1 mice developed an augmented IgG anti-C-II humoral response and more severe arthritis compared with control DBA/1 mice71 (T. Takai et al., unpublished observations) (Fig. 3). Even on non-susceptible genetic backgrounds, such as C57BL/6, FcγRIIb deletion was sufficient to render mice susceptible to CIA72. These results indicate clearly that the development of CIA is dependent on the presence of the activating FcRs FcγRI and/or FcγRIII, and is negatively regulated by FcγRIIb, which downregulates both B-cell and effector-cell responses.
Models of Goodpasture's syndrome. A similar suppressive role for FcγRIIB might also be found in many other autoimmune disease models and in human autoimmune disorders. In humans, GPS is characterized by a rapid and progressive glomerulonephritis and haemorrhagic pneumonitis, often with fatal results80. The presence of antibodies that are specific for type-IV collagen (C-IV) and IC deposition along the basement membranes of both lungs and glomeruli has led to the proposal that autoantibodies specific for C-IV are important in the pathogenesis of this disease81. However, the mechanisms that result in the loss of tolerance and the development of autoantibodies to C-IV were unknown, until the recent success in developing an animal model for this disease in FcγRIIb-deficient mice82. Immunization of FcγRIIb-deficient mice with C-IV results in pulmonary haemorrhage and glomerulonephritis, whereas wild-type controls and FcRγ-deficient mice do not have evidence of disease, which indicates a role for the FcγRIIb regulatory pathway in the aetiology of this autoimmune disease. Importantly, FcγRIIb-deficient, but not wild-type or FcRγ-deficient, mice have elevated autoantibody responses to C-IV, which indicates that mouse GPS depends on autoantibody production in this susceptible background. The enhanced responses of effector cells, such as alveolar macrophages, to deposited autoantibodies are an important contributing factor to the development of disease, as described for IC-mediated alveolitis12 and CIA72. The role of FcγRIIb in mouse GPS, as well as mouse CIA, indicates that alterations in its function or expression could be a susceptibility factor for the pathogenesis of the human diseases.
Spontaneous autoimmunity
The involvement of FcRs in autoimmunity has been well documented in various 'induced' autoimmune disease models, as described above. However, it is important to clarify how FcRs are involved in the 'spontaneous' onset of autoimmune diseases to evaluate the role of FcRs in the crucial initiation phase of autoimmunity and in maintaining peripheral tolerance.
FcγRIIb deficiency and spontaneous autoimmunity. In this respect, Bolland and Ravetch83 have provided an unexpected example by showing that FcγRIIb-deficient mice develop autoantibodies and autoimmune glomerulonephritis in a strain-dependent fashion. Deficiency of FcγRIIb on the C57BL/6 backround results in the production of ANTI-DNA ANTIBODIES. These mice develop fatal autoimmune glomerulonephritis and have reduced survival. By contrast, FcγRIIb-deficient BALB/c mice maintain tolerance to nuclear antigens and are resistant to the development of autoimmunity. The most crucial element causing loss of tolerance in FcγRIIb-deficient C57BL/6 mice has been shown to be the absence of FcγRIIb on B cells83. Attempts to identify the other susceptibility loci for the enhanced production of anti-nuclear antibodies in C57BL/6, but not BALB/c, mice have been successful. Two new, recessive loci have been mapped to chromosomes 12 and 17, and are termed sbb2 and sbb3, respectively.
Protection from spontaneous autoimmunity. IC formation and tissue deposition triggers the pathogenic consequences of systemic autoimmune disease. Clynes et al.65 have found that the disruption of FcRγ results in the uncoupling of IC formation and deposition from the spontaneous onset of lupus nephritis in NZB/W F1 mice. FcRγ-deficient NZB/W F1 mice generated and deposited ICs, and activated complement, but they were protected from severe nephritis, which indicates that the activation of effector cells through FcRγ is crucial for disease development. In addition, Suzuki et al.66 have shown that FcRs have a pivotal role in anti-glomerular-basement-membrane antibody-induced glomerulonephritis. In FcRγ-deficient mice, renal injuries were markedly attenuated, whereas FcγRIIb-deficient mice had accelerated development of glomerular injuries. However, it remains to be determined whether FcγRIIb-deficient NZB/W F1 mice develop more severe renal disease than control mice.
MRL._Fas_lpr/lpr mice — which have a Fas mutation — have a lymphoproliferative phenotype with anti-nuclear-antibody production, which culminates in glomerulonephritis, vasculitis, arthritis and CRYOGLOBULINAEMIA. This disease is similar to the human autoimmune disease SLE. Interestingly, however, after backcrossing to C57BL/6 or C3H/HeJ genetic backgrounds, _Fas_lpr/lpr mice no longer develop any spontaneous autoimmune diseases, which indicates the presence of unknown inhibitory element(s), one of which could be FcγRIIb73,74 (K. Yajima et al., unpublished observations). In a recent article, Bolland et al.84 reported that Fas mutation rendered C57BL/6 _FcγRIIb_−/− mice more resistant to lupus-like disease, and they speculated that the _Fas_lpr/lpr mutation might attenuate IC deposition or effector-cell responses to these ICs by modifying the apoptotic pathway, thereby reducing disease progression. It will be interesting to clarify the mechanism of this protective effect of _Fas_lpr/lpr mutation.
NOD mice and FcR defects. The non-obese diabetic (NOD) mouse is a model of human type-1 diabetes, an autoimmune disease that is characterized by T-cell-mediated destruction of insulin-producing pancreatic β-cells. In addition, NOD mice have anomalies in the humoral immune response, including an elevation of serum levels of IgG (hyper IgG) and the production of autoantibodies — such as anti-insulin antibodies and natural thymocytotoxic antibodies — although the underlying mechanisms are largely unknown. Luan et al.85 have mapped a locus for hyper IgG in NOD mice to the distal part of chromosome 1, in the region of the FcγRII and FcγRIII genes. They also identified a defect of FcγRIIb expression in macrophages of NOD mice that is associated with the hyper-IgG phenotype, which indicates that macrophage FcγRIIb might regulate serum levels of IgG1 and IgG2b by means of their catabolism. An additional intriguing observation is that NOD mice can be induced to develop SLE, and that the susceptibility locus for anti-nuclear-autoantibody production in this inducible SLE model in NOD mice has been mapped to a distal region of chromosome 1 that contains FcγRIIb86.
It is not known yet whether FcγR-deficient NOD mice have more or less severe diabetes than control NOD mice. Such observations would clarify the involvement of FcγRs in autoimmune diabetes, particularly in terms of the antigen-presentation capacity of FcγRs.
FcR defects and EAE. As discussed below, FcR polymorphism could be a susceptibility factor for MULTIPLE SCLEROSIS (MS) in humans87. Recent observations88 in EXPERIMENTAL AUTOIMMUNE ENCEPHALOMYELITIS (EAE), an animal model of MS, might provide an insight into the mechanisms that are involved in the onset of the disease in humans. The development of EAE is dependent crucially on myeloid cells, both in the induction phase and the effector phase. Abdul-Majid et al.88 analysed the induction of EAE in FcRγ-deficient or FcγRIIb-deficient mice. They showed that the lack of FcγRIIb enhanced susceptibility to myelin oligodendrocyte glycoprotein (MOG)-induced EAE and increased the extent of demyelination. By contrast, FcRγ-deficient mice were protected from EAE. The authors speculated that the resistance of FcRγ-deficient mice to EAE is due to the inefficient antigen processing or presentation of myelin proteins during the induction of secondary immune responses locally in the central nervous system.
It should be noted that mice that are deficient for DAP12 (also known as KARAP) — an adaptor molecule that is homologous to FcRγ — are also protected from EAE89,90, which indicates that ITAM-containing receptor complexes, such as activating-type FcγRs and unidentified DAP12-associating receptors, might have important roles in the disease.
Fc-receptor polymorphisms in humans
Genetic differences between FcRs have been described in patients with autoimmune diseases19,87,91,92,93,94,95,96,97,98,99,100,101,102,103 (Table 3). In this section, I provide a brief overview of the polymorphisms that are found in FcR genes and their possible relation to autoimmune diseases. It should be noted, however, that there are some negative studies, in which no link between SLE and FcR polymorphisms was found104,105. Because FcγR genes are in close proximity to each other on human chromosome 1, it remains possible that they are in linkage disequilibrium with each other, so correlations with one FcγR genotype might in fact implicate other FcγR genes in disease susceptibility.
Table 3 Fc-receptor polymorphisms in human autoimmune diseases
FcγRIIA. The high-responder/low-responder (HR/LR) polymorphism of FcγRIIA is named after the ability of T cells from some normal individuals to proliferate in response to mouse IgG1. It was shown that IgG1 anti-T-cell-receptor-complex antibody was mitogenic to all human T cells in vitro, if the culture contained high-responder monocytes.106. FcγRIIA in high responders has an arginine at position 131 (131Arg), whereas this residue is a histidine in the low responders. The affinity of the high-responder FcγRIIA for all human IgG subclasses is reduced compared with the low-responder allele, and is almost abolished for IgG2, which indicates that this polymorphism is located near to the IgG-binding site of FcγRIIA. The distribution of FcγRIIA alleles differs according to ethnicity. The FcγRIIA-HR (FcγRIIA 131Arg) phenotype has been reported as a susceptibility factor for SLE in Caucasians94, African–Americans95 and Koreans96.
FcγRIIIA and FcγRIIIB. FcγRIIIA variants are also known, and they might be associated with autoimmunity. The 158Val allelic variant of FcγRIIIA has a higher affinity for IgG1 and IgG3 than the 158Phe-type receptor. The FcγRIIIA 158Phe/Phe phenotype is proposed to be a susceptibility factor for SLE97,98,99 and rheumatoid arthritis101, possibly due to the inefficient clearance of circulating or tissue-deposited ICs, as noted above.
Two common allelic forms of neutrophil-specific FcγRIIIB were recognized originally by serological techniques as neutrophil antigen 1 (NA1) and NA2 alloantigens107, which are involved in blood-transfusion reactions and alloimmune neutropaenia. There seems to be no difference in IgG-binding affinity between NA1 and NA2. However, NA2 is suggested to have a lower ability to mediate phagocytosis than NA1 (Ref. 108). The NA2 allele has been reported to be a susceptibility factor for SLE in Japanese individuals100, whereas the NA1 allele has been reported to be associated with Wegener's granulomatosis, a type of systemic vasculitis that is caused by anti-neutrophil cytoplasmic antibodies102. A correlation between the FcγRIIA 131Arg (HR) and FcγRIIIB NA2 allotypes and the severity of GUILLAIN-BARRÉ SYNDROME (GBS) and MS has been reported also87,103 (Table 2).
FcγRIIB. Among 100 Japanese healthy donors, seven single-nucleotide substitutions were identified in the FcγRIIB gene, five of which are missense substitutions in the IgG-binding domain, which might affect the binding capacity of FcγRIIB109. A recent analysis of Japanese patients with SLE has identified a single-nucleotide polymorphism in the FcγRIIB gene that results in the Ile232Thr substitution91. The 232Thr/Thr phenotype was found at a significantly higher frequency in Japanese SLE patients compared with normal individuals. These observations might be important, because no one has reported any reliable association of mutations in FcγRIIB with autoimmune diseases in general. Amino-acid position 232 of FcγRIIB is in the transmembrane region, and although it has not yet been determined whether the 232Thr/Thr phenotype leads to impairment of FcγRIIB function, this seems probable, because the intact membrane domain is necessary for induction of the apoptotic signal by mouse FcγRIIb58.
Conclusions and future perspectives
ITAM-containing FcRs can prime various autoimmune diseases, whereas FcγRIIB is one of the pivotal elements for maintaining peripheral tolerance. The impairment of the functional balance between activating and inhibitory FcRs leads directly to IC-mediated autoimmune diseases. In mice, the impairment of homeostatic mechanisms for eliminating autoreactive B cells, such as Fas mutation, and the loss of peripheral tolerance due to impaired FcγRIIb function might be sufficient for disease development. So far in humans, attempts to identify polymorphisms in FcRs have focused exclusively on their ectodomains, mutations of which might influence IC binding and clearance. Now, it is important to identify polymorphisms or mutations that impair FcR-regulated signalling. In particular, the identification of mutations in the human FcγRIIB gene will greatly facilitate our understanding of the role of FcRs in autoimmune diseases, as has been shown in mice.
Strategies that result in the upregulation of FcγRIIB signalling are potential new therapeutic approaches for the treatment of autoimmune diseases (Box 2). Whereas most studies so far have focused on antibody-mediated autoimmune diseases, additional studies are now necessary to elucidate the role of FcRs in autoimmune diseases for which T-cell-mediated responses are believed to be an important causal pathway, such as type-1 diabetes and MS. It will also be important to elucidate the molecular mechanisms that underlie the control of antigen presentation and cross-presentation by FcRs. As such mechanisms are revealed, they might also provide new targets for the modulation of immune responses for therapies for autoimmune diseases.