Ultraviolet B Light Emitting Diodes (LEDs) Are More Efficient and Effective in Producing Vitamin D3 in Human Skin Compared to Natural Sunlight (original) (raw)
Introduction
The beneficial role of ultraviolet radiation on bone health began in 1919 when Huldschinsky reported that children who were exposed to a mercury arc lamp showed significant radiologic improvement of their rickets several months later. He noted that exposure to one forearm of a child with rickets displayed the same radiologic improvements in the other arm not exposed to the mercury arc lamp1. He concluded that something was produced in the skin that entered the circulation causing widespread improvements in bone mineralization in children with rickets. The connection with sunlight was made when Hess et al.2 exposed rachitic children to the sun in New York City from half an hour to several hours and reported significant improvements in their rickets2.
It is now recognized that during exposure to sunlight, ultraviolet B (UVB) radiation between 290–315 nm penetrates into the skin and is absorbed by 7-dehydrocholesterol (7-DHC)3,4,5. This results in the cleavage of the bond between C9 and C10 to form cis-cis previtamin D3. The action spectrum for the production of previtamin D3 revealed that the most efficient wavelengths were 298 ± 2 nm4. Once formed, previtamin D3 is thermodynamically unstable, and the triene system rearranges into a more thermodynamically stable form, vitamin D3 1, 6,7,8,9,10. The phospholipid bilayer of the keratinocyte cell membrane in human skin plays a major role in this process by maintaining the previtamin D3 in a thermodynamically unstable conformer that causes it to rapidly isomerize to vitamin D3 7.
Vitamin D3 production in human skin depends on several factors. The size of the area exposed to UV radiation is directly proportional to the amount of vitamin D3 produced; the larger the area exposed, the more vitamin D3 is produced. For example, sunbathing in a swimsuit can produce an amount of vitamin D3 similar to ingesting ~ 20,000 IU of vitamin D1, 11. Aging, skin pigmentation, sunscreen use, time of day, latitude, season, and altitude are other factors that affect this vital cutaneous process1, 6, 8, 10, 11.
Since the first observations demonstrating that exposure to ultraviolet radiation was effective in curing rickets, various devices emitting ultraviolet radiation have been developed and used to treat and prevent vitamin D3 deficiency. The Sperti lamp was available in pharmacies in the United States for the treatment and prevention of rickets in the 1940s1. It was a high intensity mercury arc lamp similar to what Huldschinsky had used. A modern version that contains fluorescent tubes that emit ultraviolet radiation was effective in raising blood levels of 25-hydroxyvitamin D [25(OH)D] in healthy adults and in patients with a fat malabsorption syndrome associated with cystic fibrosis12, 13. Tanning beds that emit UVB radiation produce vitamin D3 14. Exposure to tanning bed radiation raised blood levels of 25(OH)D in a patient with Crohn’s disease who was unable to absorbed dietary or supplemental vitamin D3 15. Patients with fat malabsorption syndromes including those with inflammatory bowel disease, cystic fibrosis and gastric bypass surgery are at high risk for vitamin D3 deficiency and are in need of a user friendly device that can promote the cutaneous production of vitamin D3 8, 16.
UV wavelengths between 290–300 nm were found to be the most efficient for vitamin D3 production in human skin and human skin equivalent models4, 5. With the advancement of gallium nitride LED (Light Emitting Diode) technology that emits UV radiation, it is now possible to manufacture LEDs that are efficient and suitable for a wide range of commercial uses including for sterilization17, 18. These LEDs can be tuned to emit the desired wavelengths including those that can theoretically can convert 7-DHC to previtamin D3 in human skin.
Barnkob et al. investigated the efficiency of LEDs with different peak wavelengths in producing vitamin D3 in pig skin19. They found that vitamin D3 could be produced when pig skin was irradiated with LEDs that had peak wavelengths between 292–300 nm; 296 nm was found to be the most effective for vitamin D3 production. Morita et al. exposed mice to LEDs with peak wavelengths between 268 and 316 nm two times per week for 4 weeks (8 doses in total). They reported that serum levels of 25(OH)D significantly increased in exposed mice compared to controls regardless of the LED’s wavelength20.
Data regarding the efficiency of UVB emitting LEDs for producing vitamin D3 in human skin is lacking. This study had two objectives. First, to determine the efficiency of previtamin D3 production in ampoules containing 7-DHC following exposure to LEDs emitting different wavelengths to determine which one was most effective and efficient. The second objective was to compare the efficiency of vitamin D3 production in human skin exposed to the most effective and efficient LED to sunlight.
Methods
Equipment
Four LEDs with different peak wavelengths, 293, 295, 298, and 305 nm, were used in this study (Fig. 1).The 293 nm LED was obtained from RayVio (Hayward, CA, USA), 295 nm and 305 nm was from Sensor Electronic Technology, Inc (SETi, Columbia, SC, USA), and 298 nm was from DOWA Electronic Materials Company, Ltd (Chiyoda-Ku, Tokyo, Japan). The LEDs were powered with a power supply (supplied by RayVio) set to 50 V and 10 mA for all the experiments. The energy output of each LED was measured using a UVB meter, Solarmeter (Solar Light Company, Inc, Glenside, PA). This meter estimates the output in terms of Minimal Erythemal Dose (MED) per hour which is equivalent to 15.6 mJ/cm2/hr.
Figure 1
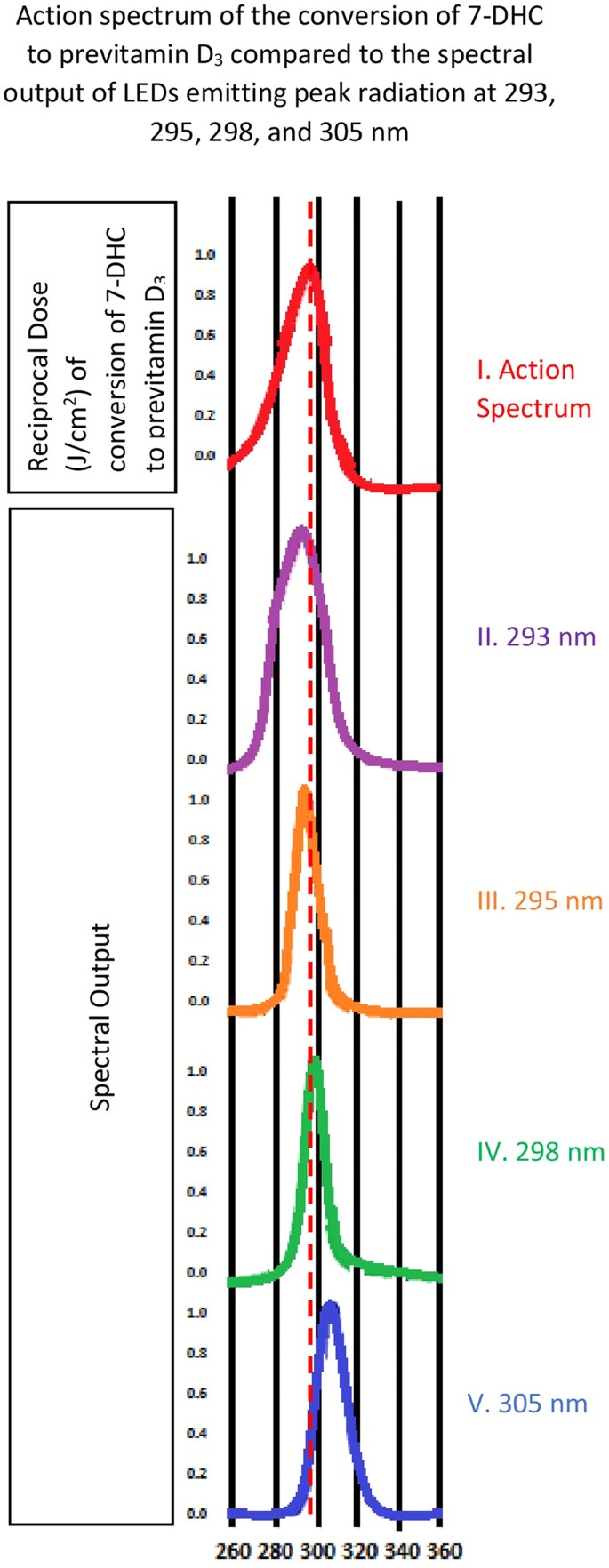
The action spectrum for the production of previtamin D3 in human skin (A) and the spectral output of the various LEDs that were evaluated (B–E). The dashed line represents the peak wavelength of 297.5 nm.
The ampoules used in this experiment were borosilicate ampoules from Wheaton Inc. (Millville, NJ USA) containing 50 µg/mL of 7-DHC dissolved in 1 mL of ethanol as previously described12. The skin samples used were surgically obtained from the Plastic Surgery Department at Boston Medical Center. Each skin sample was cut to have a surface area of approximately 4 cm2. This study was categorized as an approved exempt study by Boston University Medical Campus Institutional Review Board (BUMC IRB). All methods in this study were carried out in accordance with the guidelines and regulations issued by our IRB. Due to the exempt nature of this study, all of the discarded samples were deidentified and therefore informed consent was not required from those providing skin samples.
Ampoule and Skin Exposure to Various LEDs and Sunlight
For UV irradiation, the samples (ampoule or skin) were placed in a quartz dish on top of a plastic apparatus with a 1 cm2 opening in the center focused 10.0 mm ± 1.0 mm above the top of the LED. The ampoule or ~4 cm2 piece of skin was placed over the 1 cm2 opening. To ensure radiation of the entire piece of skin, this process was repeated for the unexposed areas so that the entire skin sample was exposed to the same amount of UVB radiation.
To determine which LED was most efficient in converting to previtamin D3, the energy output for each LED was measured using the Solarmeter to calculate the exposure time needed for each LED to reach 46.8 mJ/cm2 (equivalent to 3 MEDs). Three ampoules were exposed for each respective calculated time to determine the efficiency of each LED in converting 7-DHC to previtamin D3. The LED with the highest percent conversion and shortest/least exposure time was selected for additional experiments for a comparative analyses between the LED and sun exposure using human skin samples. Each skin sample that came from one patient was cut in half; one half was exposed to the LED and the other half was exposed to sunlight in Boston in October at noon time for the same energy exposure.
Sample Analysis
a. Ampoules
Immediately after the allotted time of exposure, 200 µl was recovered from each ampoule and transferred to a test tube and dried under nitrogen gas. The dried samples were re-dissolved in 1 mL 0.8% isopropyl alcohol (IPA) in hexane to be analyzed with a straight phase High-Pressure Liquid Chromatography (HPLC) at a flow rate of 1.5 mL/min as previously described12.
b. Skin
After the skin was irradiated, it was submerged in water at 60 °C for 1 minute12. The epidermis was separated from the dermis using a scalpel to scrape the layer off. The dermis was discarded and the epidermis was placed in 2.5 mL of 8% ethyl acetate in hexane and sonicated for 10 seconds. The samples were then incubated overnight at 50 °C to allow the conversion of previtamin D3 to vitamin D3. This process facilitated the separation of lipid contaminants that migrated near where previtamin D3 eluted, permitting the quantitation of the vitamin D3. Therefore, the vitamin D3 content was considered as the previtamin D3 equivalent observed in ampoules. After the overnight incubation the cellular particulates remained at the bottom and the solution was decanted to a test tube and dried under nitrogen gas. The samples were re-suspended in 1 mL of 0.8% IPA in hexane, centrifuged to remove any remaining particulates and the supernatant was dried under nitrogen, and resuspended in 140 µl of 0.8% IPA in hexane and analyzed on a straight phase HPLC at a flow rate of 1.5 mL/min.
Statistical Analysis
Descriptive statistics were used to present the data, mean and standard deviation. No significant difference in mean previtamin D3 percent conversion was expected between the 293, 295, and 298 nm LED, so no formal statistical testing was done to compare them. However, the percent conversion for the 305 nm LED was expected to be significantly different compared to the other LEDs based on the published previtamin D3 action spectrum4.
Results
Wavelength efficiency in previtamin D3 production in ampoules
Four ampoules containing 7-DHC were irradiated for a time that was equivalent to 46.8 mJ/cm2 (Table 1). The mean percent conversion of 7-DHC to previtamin D3 was similar for the 293, 295, and 298 nm LEDs. However, the percent conversion for the 305 nm LED was more than 90% lower compared to other LEDs (_P_-value < 0.001; Table 1). The 293 nm LED was able to generate the same amount of previtamin D3 in less than half the time compared to the other LEDs. This was also apparent when evaluating the percent conversion of 7-DHC to previtamin D3 for the same period of time of 2.55 minutes for each of the LEDs. For example only 0.47% of 7-DHC would be converted to previtamin D3 with the 305 nm LED compared to 11.2% with the 293 nm LED. Therefore the 293 nm LED was selected for the comparison of the vitamin D3 production efficiency with natural sunlight.
Table 1 Exposure Time and percent conversion of 7-DHC to previtamin D3.
Efficiency of Sunlight vs LED on Vitamin D3 Production in Human Skin
Fitzpatrick skin type II samples from different donors were exposed to the sun on different days for 32.15 minutes (11.7 mJ/cm2; 0.75 MED) and 1 hour (37.4 mJ/cm2) at 12 pm in the middle of October. The other half of the skin sample was exposed to the 293 nm LED on the same day for 1.36 min and 2.73 min to obtain the same energy exposure for the 30 minute (11.7 mJ/cm2) and one hour sun exposure (37.4 mJ/cm2) respectively. Figure 2 presents representative chromatograms and Fig. 3 presents the UV absorption spectrums that confirmed the identification of the peaks, of an ampoule exposed to UV radiation showing 7-DHC and previtamin D3 (A) and the thermal conversion of previtamin D3 to vitamin D3 (B). Figure 2C and D are representative chromatograms of human skin exposed to the 293 nm LED and sunlight respectively demonstrating the lipid contaminants that migrated near where previtamin D3 migrated. The UV absorption spectrum for the contaminant was different than previtamin D3.
Figure 2
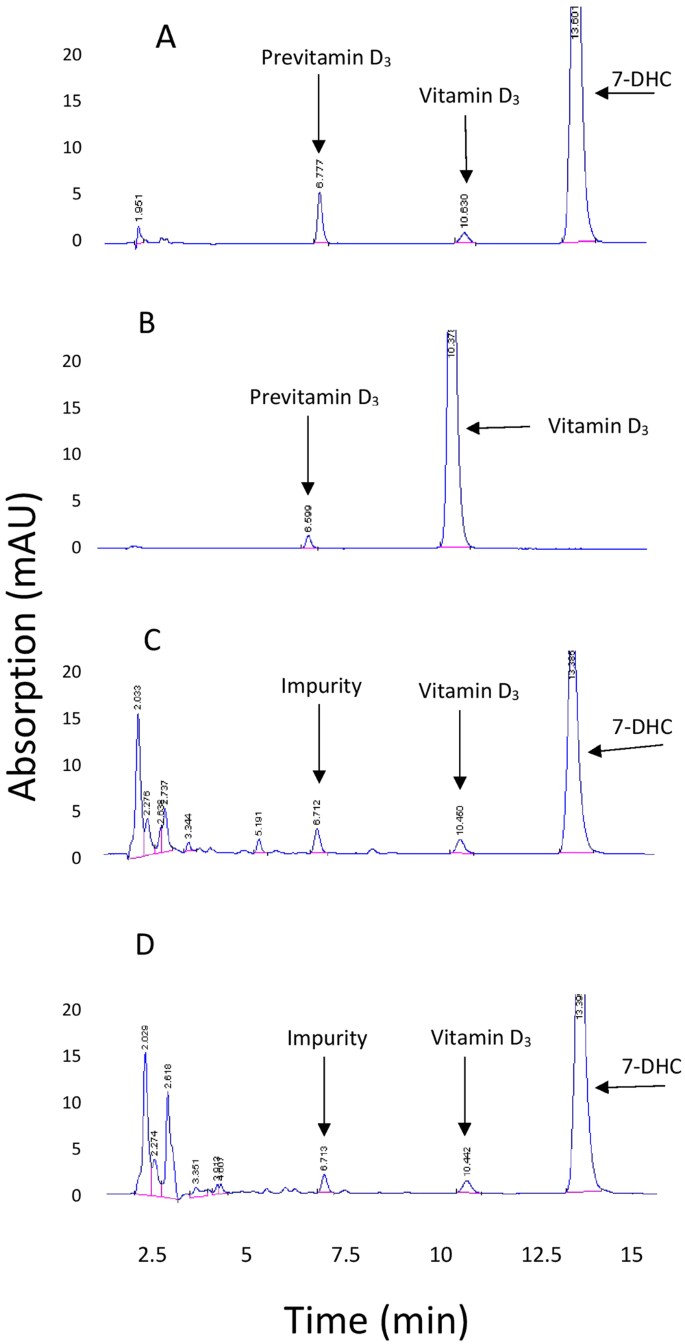
Chromatograms of ampoules containing 7-DHC and exposed to ultraviolet radiation (A) and standards of previtamin D3 and vitamin D3 (B). 2 C and 2D are chromatograms of lipid extracts of human skin after exposure to a 293 nm LED (C) and sunlight (D) followed by incubation overnight.
Figure 3
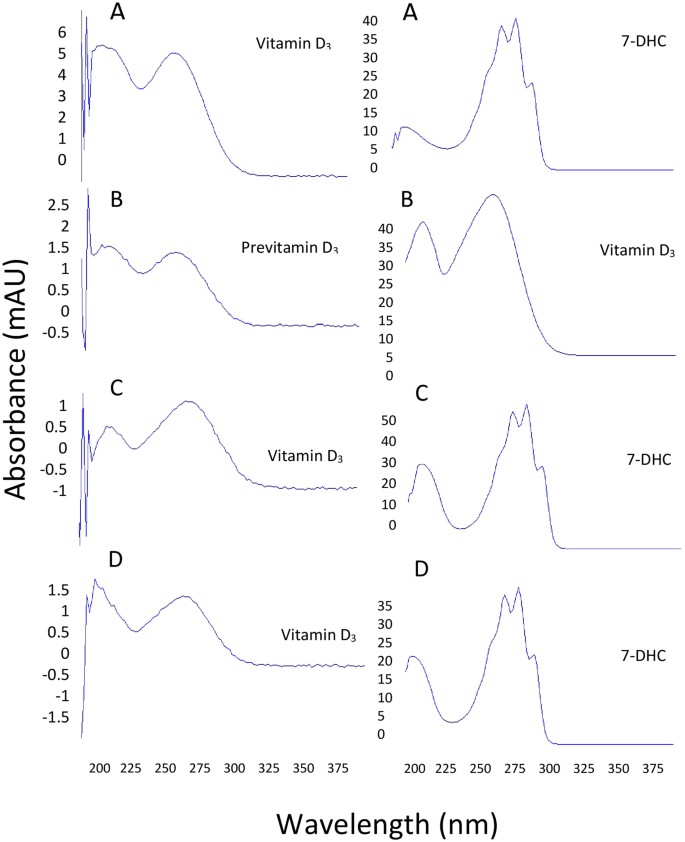
UV absorption spectrums of vitamin D3, previtamin D3, and 7-DHC obtained from ampoules (A and B) and from human skin after exposure to a 293 nm LED (C) and sunlight (D).
An evaluation of the efficiency of the 293 nm LED to produce vitamin D3 in type II skin compared to sunlight revealed that the LED was greater than 2 fold more effective (Table 2). It took only 0.52 minutes for the 293 nm LED to emit 11.7 mJ/cm2 which resulted 1.2% of the 7-DHC to be converted to vitamin D3. Exposure to the same amount of energy from the sun took 32.5 minutes and only 0.5% of the 7-DHC was converted to vitamin D3. When a separate type II sample was exposed to 37.4 mJ/cm2 on a different day similar results were obtained. It took only 2.73 minutes for 1.9% of 7-DHC to be converted to vitamin D3 compared to 60 minutes of sun exposure converting 1.3% of 7-DHC to vitamin D3. To determine the effect of increased skin pigmentation on the cutaneous production of vitamin D by the LED compared to sunlight, skin type III from 2 subjects was exposed to 31.2 mJ/cm2 from the 293 LED and sun on the same day. It took 92.2 minutes of sun exposure to convert 0.6% of 7-DHC to vitamin Ds compared to only 2.47 minutes to convert 1.3 and 1.7% of the 7-dehydrocholesterol to vitamin D3 in the type III skin samples.
Table 2 Percent conversions of 7-DHC to previtamin D3 in skin Type II and skin Type III following LED/Sun exposure.
Discussion
We evaluated several LEDs of varying wavelengths to determine which was most desirable to develop for human trials. We found that the 293 nm LED, provided by Rayvio, was best suited for human trials due to a more than 50% shorter exposure time to produce the same amount of vitamin D3 as the other LEDs. This LED was also found to be 2.4 and 2.5 times more efficient in producing vitamin D3 in Type II and Type III human skin respectively compared to being exposed to the same amount of energy from the sun in a much shorter time. For example the suberythemal exposure of the skin type II to 0.75 MED from the 293 LED produced 2.3 IUs cm2 (5.63 ng/cm2) in one half minute compared to a less than half the amount (0.9 IUs; 2.35 ng/cm2) vitamin D3 when the same skin sample was exposed to the sun for more than 60 times longer time (32.15 min). Assuming an average adult body surface area 1.7 m2 21, a 0.75 MED exposure of the whole body to the 293 nm LED would generate 39,100 IUs. The Institute of Medicine recommends that for most children and adults their requirement is 600 IUs of vitamin D a day. This would translate into exposing 260 cm2 (40.3 in2) of the skin surface to the 293 nm LED for approximately one half minute. This is compared to generating 15,300 IUs exposed to 0.75 M ED of sunlight. To generate 600 IUs of vitamin D3 would require 666 cm2 (103 in2) of the skin surface to be exposed to approximately 30 minutes of sunlight.
Vitamin D production in human skin following sun exposure depends on the position of the sun in the sky, or the zenith angle6, 8, 11, 22. The amount of UV radiation reaching the earth’s surface increases when the zenith angle decreases. Moreover, the zenith angle depends on the latitude, season, and time of the day1, 23, 24. As a result, the optimal times for vitamin D production in human skin is in the summer between the hours of 10 AM-3PM1, 24, 25. However because time of day, season, latitude, altitude, and weather conditions can all influence the cutaneous production of vitamin D3 it is difficult to obtain an adequate amount of vitamin D3 from sun exposure without some guidance. Furthermore it is often unrealistic to be outdoors between 10 AM and 3 PM because of working schedules. Therefore, LEDs would offer an alternative efficient way of providing the user with a defined suberythemal amount of UVB radiation for producing their vitamin D requirement. These LEDs can also be developed for treating and preventing recurrent vitamin D deficiency in patients who are unable to absorb vitamin D through their gastrointestinal tract due to fat malabsorption syndromes15. Another use could be in patients with chronic kidney disease. It was observed that patients with end-stage chronic kidney disease who were exposed to UVB radiation were able to improve their vitamin D status as well as increase their blood levels of 1,25-dihydroxyvitamin D3 and decrease their parathyroid hormone levels thereby improving their calcium and bone metabolism26. In addition, these patients required less erythropoietin to maintain their blood hematocrit and had significant improvement in their cardiovascular status26.
However, prolonged exposure to UV radiation from the sun increases the risk for non-melanoma skin cancer27. This occurs mainly due to DNA damage from wavelengths that are absorbed by DNA that lead to the formation of DNA damage products including cyclobutane pyrimidine dimers (CPD)27,28. Masuma et al. studied CPD formation after exposing rat pheochromocytoma cell line, PC 12 cells, to different UV wavelengths (250 nm–310 nm). They found that CPD formation to be highest after 250 nm exposure and lowest after 310 nm exposure[29](/articles/s41598-017-11362-2#ref-CR29 "Masuma, R., Kashima, S., Kurasaki, M. & Okuno, T. Effects of UV wavelength on cell damages caused by UV irradiation in PC12 cells. J Photochem Photobiol B. 125, 202–8, doi: 10.1016/j.jphotobiol.2013.06.003
(2013)."). Thus, the longer the wavelength, the lesser the DNA damage. Furthermore, Felton _et al_. reported that suberythemal exposure to simulated sunlight in the UK was effective in raising blood levels of 25-hydroxyvitamin D3 (a measure of vitamin D status) while at the same time demonstrating enhanced DNA repair mechanisms that minimized DNA damage from the exposure[27](/articles/s41598-017-11362-2#ref-CR27 "Felton, S. J. et al. Concurrect beneficial (vitamin D production) and hazardous (cutaneous DNA damage) impact of low-level summer sunlight exposures. Br J Dermatol.
175(6), 1320–1328 (2016).") suggesting that humans have adapted to sensible sun exposure[30](/articles/s41598-017-11362-2#ref-CR30 "Holick. M. F. Can you have your cake and eat it too? The sunlight D-lema. Br J Dermatol. 175(6), 1129–1131 (2016)."). Although the 305 nm would have been thought to be the most desired due to its lower energy, because of the marked decrease in quantum efficiency, there was a more than 10 fold decrease in the production of previtamin D3 compared to the other LEDs. It would likely require 10 times more 305 nm photons to generate the same amount of previtamin D3 as the 293 nm LED. Therefore another advantage of the 293 nm LED may be reduced risk of skin damage when compared to exposure to sunlight or the 305 nm LED.LEDs can be manufactured with any desired wavelength that has a narrow range. It is possible to have an LED with a wavelength that can maximally produce vitamin D3 more efficiently than sunlight. These LEDs can be used for different functions including vitamin D3 production for patients with malabsorption syndromes. The LED can also be incorporated into wearable gadget devices to provide individuals with their daily vitamin D3 requirement. Moreover, LEDs can be used for vitamin D3 for patients with chronic kidney disease (CKD). It has been showed that UVB exposure was superior to oral supplements in elevating serum levels of 25(OH)D in patients with CKD26.
Conclusion
The optimal range of LEDs emitting UVB radiation for vitamin D production was found to be between 293 and 298 nm. The 293 nm LED was found to be 2.4 times more efficient in converting 7-DHC to previtamin D3 in human skin than the sun, thus improving its safety profile. This data provides helpful information for medical device development in the future that can be used for vitamin D supplementation in both healthy and diseased individuals.
References
- Wacker, M. & Holick, M. F. Sunlight and Vitamin D: A global perspective for health. Dermatoendocrinol. 5, 51–108 (2013).
Article CAS PubMed PubMed Central Google Scholar - Hess, A. F. & Ungerm, L. J. The cure of infantile rickets by artificial light and by sunlight. Exp Biol Med. 18(8), 298 (2016).
Article Google Scholar - Lehmann, B., Genehr, T., Knuschke, P., Meurer, M. & Pietzsch, J. UVB-induced conversion of 7-dehydrocholesterol to 1α,25-dihydroxyvitamin D3 in an in vitro human skin equivalent model. J Invest Dermatol. 117, 1179–85 (2001).
Article CAS PubMed Google Scholar - MacLaughlin, J. A., Anderson, R. R. & Holick, M. F. Spectral character of sunlight modulates photosynthesis of previtamin D3 and its photoisomers in human skin. Science. 216, 1001–3 (1982).
Article ADS CAS PubMed Google Scholar - Nemanic, M. K., Whitney, J. & Elias, P. M. In vitro synthesis of vitamin D3 by cultured human keratinocytes and fibroblasts: action spectrum and effect of AY-9944. Biochim Biophys Acta. 841, 267–77 (1985).
Article CAS PubMed Google Scholar - Holick, M. F. The cutaneous photosynthesis of previtamin D3: a unique photoendocrine system. J Invest Dermatol. 77, 51–8 (1981).
Article CAS PubMed Google Scholar - Holick, M. F., Tian, X. O. & Allen, M. Evolutionary importance for the membrane enhancement of the production of vitamin D3 in the skin of poikilothermic animals. Proc Natl Acad Sci. 92, 3124–3126 (1995).
Article ADS CAS PubMed PubMed Central Google Scholar - Holick, M. F. Vitamin D deficiency. N Engl J Med. 357, 266–81 (2007).
Article CAS PubMed Google Scholar - Holick, M. F. Vitamin D: A D-lightful solution for good health. J Med Biochem. 31, 263–4 (2012).
Article Google Scholar - Holick, M. F. & Chen, T. C. Vitamin D deficiency: a worldwide problem with health consequences. Am J Clin Nutr. 87, 1080S–6S (2008).
CAS PubMed Google Scholar - Nimitphong, H. & Holick, M. F. Vitamin D status and sun exposure in southeast Asia. Dermatoendocrinol. 5, 34–7 (2013).
Article PubMed PubMed Central Google Scholar - Dabai, N., Pramyothin, P. & Holick, M. F. The effect of ultraviolet radiation from a novel portable fluorescent lamp on serum 25-hydroxyvitamin D3 levels in healthy adults with Fitzpatrick skin types II and III. Photodermatol., Photoimmunol., Photomed. 28(6), 307–311 (2012).
Article CAS Google Scholar - Chandra, P. et al. Treatment of vitamin D deficiency with UV light in patients with malabsorption syndromes: a case series. Photodermatol Photoimmunol Photomed. 23, 179–85 (2007).
Article CAS PubMed PubMed Central Google Scholar - Tangpricha, V. et al. Tanning is associated with optimal vitamin D status (serum 25-hydroxyvitamin D concentration) and higher bone mineral density. Am J Clin Nutr. 80, 1645–9 (2004).
CAS PubMed Google Scholar - Koutkia, P., Lu, Z., Chen, T. C. & Holick, M. F. Treatment of vitamin D deficiency due to Crohn’s disease with tanning bed ultraviolet B radiation. Gastroenterology. 121, 1485–8 (2001).
Article CAS PubMed Google Scholar - Margulies, S. L., Kurian, D., Elliott, M. S. & Han, Z. Vitamin D deficiency in patients with intestinal malabsorption syndromes – think in and outside the gut. J Dig Dis. 16, 617–33 (2015).
Article CAS PubMed Google Scholar - Kneissl, M. et al. Advances in group III-nitride-based deep UV light-emitting diode technology. Semiconductor Science and Technology. 26 (2011).
- Nakamura, S. & Krames, M. R. History of Gallium-Nitride-Based Light-Emitting Diodes for Illumination. Proceedings of the Ieee. 101, 2211–20 (2013).
Article CAS Google Scholar - Barnkob, L. L., Argyrak, I. A., Petersen, P. M. & Jakobsen, J. Investigation of the effect of UV-LED exposure conditions on the production of vitamin D in pig skin. Food Chem. 212, 386–91 (2016).
- Morita, D. et al. Short-range ultraviolet irradiation with LED device effectively increases serum levels of 25(OH)D. J Photochem Photobiol B. 164, 256–63 (2016).
Article CAS PubMed Google Scholar - Sacco, J. J., Botten, J., Macbeth, F., Bagust, A. & Clark, P. The average body surface area of adult cancer patients in the UK: a multicentre retrospective study. PLOS ONE. 5(1), e8933 (2010).
Article ADS PubMed PubMed Central Google Scholar - Webb, A. R., Kline, L. & Holick, M. F. Influence of season and latitude on the cutaneous synthesis of vitamin D: Exposure to winter sunlight in Boston and Edmonton will not promote vitamin D synthesis in human skin. J Clin Endo Metab. 67(2), 373–378 (1988).
- Chen, T. C. et al. Factors that influence the cutaneous synthesis and dietary sources of vitamin D. Arch Biochem Biophys. 460, 213–7 (2007).
- Holick, M. F. Biological effects of sunlight, ultraviolet radiation, visible light, infrared radiation and vitamin D for health. Anticancer Res. 36, 1345–1356 (2016).
- Webb, A. R. Who, what, where and when-influences on cutaneous vitamin D synthesis. Prog Biophys Mol Biol. 92, 17–25 (2006).
- Krause, R., Roth, H. J., Kaase, H., Stange, R. & Holick, M. F. Vitamin D status in chronic kidney disease - UVB irradiation is superior to oral supplementation. Anticancer Res. 36, 1397–401 (2016).
- Felton, S. J. et al. Concurrect beneficial (vitamin D production) and hazardous (cutaneous DNA damage) impact of low-level summer sunlight exposures. Br J Dermatol. 175(6), 1320–1328 (2016).
- Pfeifer, G. P. & Besaratinia, A. UV wavelength-dependent DNA damage and human non-melanoma and melanoma skin cancer. Photochem Photobiol Sci. 11, 90–7 (2012).
- Masuma, R., Kashima, S., Kurasaki, M. & Okuno, T. Effects of UV wavelength on cell damages caused by UV irradiation in PC12 cells. J Photochem Photobiol B. 125, 202–8, doi:10.1016/j.jphotobiol.2013.06.003 (2013).
- Holick. M. F. Can you have your cake and eat it too? The sunlight D-lema. Br J Dermatol. 175(6), 1129–1131 (2016).
Acknowledgements
This work was supported in part by an Ignition Award from Boston University. We are grateful to Dr. Theodore Moustakas, who pioneered the development of gallium nitride LEDs, for his helpful advice and assistance in helping to design LEDs that can efficiently produce vitamin D3. We are also grateful to Dr. Jaromir Slama, who gracioulsy collaborated with us to provide us with surgically obtained human skin from the plastic surgery department at Boston Medical Center.
Author information
Authors and Affiliations
- Boston University School of Medicine, Boston Medical Center, Section Endocrinology, Diabetes, Nutrition and Weight Management, Department of Medicine, Vitamin D, Skin, and Bone Research Laboratory, Boston, MA, 02118, USA
T. A. Kalajian, A. Aldoukhi, A. J. Veronikis, K. Persons & M. F. Holick
Authors
- T. A. Kalajian
You can also search for this author inPubMed Google Scholar - A. Aldoukhi
You can also search for this author inPubMed Google Scholar - A. J. Veronikis
You can also search for this author inPubMed Google Scholar - K. Persons
You can also search for this author inPubMed Google Scholar - M. F. Holick
You can also search for this author inPubMed Google Scholar
Contributions
T.A.K., M.F.H. and A.A. conceived and designed the experiments. T.A.K., A.A., A.J.V. and K.P. collected data. T.A.K., A.A., A.J.V. and M.F.H. analyzed and interpreted the data. T.A.K., M.F.H. and A.A. drafted the manuscript. All authors reviewed the manuscript. M.F.H. provided final approval for publication.
Corresponding author
Correspondence toM. F. Holick.
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article
Cite this article
Kalajian, T.A., Aldoukhi, A., Veronikis, A.J. et al. Ultraviolet B Light Emitting Diodes (LEDs) Are More Efficient and Effective in Producing Vitamin D3 in Human Skin Compared to Natural Sunlight.Sci Rep 7, 11489 (2017). https://doi.org/10.1038/s41598-017-11362-2
- Received: 22 June 2017
- Accepted: 22 August 2017
- Published: 13 September 2017
- DOI: https://doi.org/10.1038/s41598-017-11362-2