Non-high-density lipoprotein cholesterol (non-HDL-C) levels in children with nonalcoholic fatty liver disease (NAFLD) (original) (raw)
Abstract
Non-alcoholic fatty liver disease (NAFLD) is associated with increased cardiovascular disease (CVD) risk in children. Non-high density lipoprotein-cholesterol (non-HDL-C) has been shown to be a good predictor of cardiovascular events. Recent data in adults found non-alcoholic steatohepatitis (NASH) to be associated with significantly higher levels of non–HDL-C than simple steatosis, suggestive it might be used as a non-invasive tool to diagnose NASH. The goal of our study was to assess non-HDL-C levels in children with NAFLD. Our cohort consisted of pediatric patients with biopsy-proven NAFLD. Anthropometric, laboratory, and histologic data were obtained on all patients. Univariable analysis was performed to assess differences in clinical characteristics between groups. Spearman rank correlation coefficients were calculated to assess the correlation between non-HDL-C levels and clinical variables. ANCOVA was used to adjust for possible confounders. 302 subjects with NAFLD were included in our study; 203 with NASH and 99 without NASH. Subjects with NASH had significantly higher non-HDL-C levels than those without (p = 0.004). Histologic features of NASH, including ballooning, inflammation, and fibrosis were found to be weakly correlated with non-HDL-C levels, (p < 0.05 for all). After adjusting for the presence of metabolic syndrome (MetS), ALT, and GGT, the association between non-HDL-C and NASH was not significant (p = 0.66). In Conclusion, non-HDL-C levels are higher in children with NASH than those with simple steatosis, suggesting increased CVD risk. This may be a reflection of the higher prevalence of MetS. Non-HDL-C had a positive association with histologic features of NASH.
Similar content being viewed by others
Introduction
The incidence of nonalcoholic fatty liver disease (NAFLD) has been increasing dramatically over the past three decades, which has been in parallel with the childhood obesity epidemic. NAFLD is now the most common cause of chronic liver disease in children and adolescents (Schwimmer et al. 2006; Wieckowska and Feldstein 2005; Chan et al. 2004). NAFLD encompasses a spectrum of diseases that ranges from simple steatosis (characterized by hepatic lipid accumulation) to non-alcoholic steatohepatitis (NASH) (characterized by evidence of lipid accumulation with associated hepatocyte inflammation, injury, and varying degrees of fibrosis), which can progress to cirrhosis and even end-stage liver disease (Vajro et al. 2012; Feldstein et al. 2009). Multiple studies are suggesting that NAFLD may be the hepatic manifestation of metabolic syndrome (MetS) (Abdelmalek and Diehl 2007; Pagano et al. 2002). There appears to be a strong association between NAFLD, MetS, and insulin resistance, which has brought into question the possibility of NAFLD playing a role in cardiovascular disease (CVD). Furthermore, recent evidence has now linked NAFLD with an increased prevalence of CVD, independent of the presence of MetS or traditional risk factors (Alkhouri et al. 2011; Targher 2007; Targher et al. 2008a). More importantly, it has also been found that children with NASH can be at an even higher risk for atherosclerosis than those patients with simple steatosis (Nobili et al. 2010).
Recently, non-high-density lipoprotein cholesterol (non-HDL-C) has become increasingly recognized as an important measure of atherogenic particles, as it reflects the cholesterol in all lipoprotein particles that are considered to be atherogenic. Non-HDL-C has been strongly associated with predicting coronary artery disease (Orakzai et al. 2009). In adults, it has been added on to a recommended screening algorithm by The Adult Treatment Panel III of the National Cholesterol Education Program (Grundy et al. 2004). Additionally, in a consensus report by the American Diabetes Association and American College of Cardiology Foundation, they identified that non-HDL-C was a better marker than low-density lipoprotein (LDL) cholesterol for identifying high-risk patients at cardiovascular risk (Brunzell et al. 2008).
Taking into consideration that patients with NAFLD are at increased cardiovascular risk, and that those patients with NASH may be at even higher risk for atherosclerosis than those with simple steatosis, a recent adult study investigated the ability of non-HDL-C to differentiate NASH from simple steatosis in patients with NAFLD. In those patients who did not take any lipid-lowering agents, NASH was associated with significantly higher levels of non-HDL-C as compared to those patients with just simple steatosis. Their study concluded that non-HDL-C could be utilized as a non-invasive biomarker to differentiate between steatosis and NASH (Corey et al. 2012). In our study we aimed to examine non-HDL-C levels in pediatric patients with NAFLD to assess if increased CVD risk may be associated with worsening histologic severity of NAFLD, and more specifically NASH as compared to simple steatosis.
Materials and methods
Patients
Pediatric patients with biopsy-proven NAFLD were seen at and enrolled in this study performed at the Bambino Gesù Children’s Hospital (Rome, Italy) between January 2003 and December 2009. This study was approved by the ethics committee of the Bambino Gesù Children’s Hospital and Research Institute. The study was carefully explained to the children’s guardians and written consent was obtained.
All included subjects raised suspicion for NAFLD based on persistently elevated serum aminotransferase levels and imaging studies that revealed a diffusely hyperechogenic liver suggestive of fatty liver, with a final diagnosis of NAFLD made on liver biopsy. Exclusion criteria for these patients with NAFLD including (1) alcohol consumption; (2) hepatic viral infections (such as hepatitis A, B, C, D, and E; cytomegalovirus; and Epstein-Barr virus); (3) history of parenteral nutrition; (4) use of drugs that are known to induce steatosis (e.g.: prednisone, valproate, or amiodarone), affect body weight or carbohydrate metabolism; and (5) known liver disease, such as autoimmune liver disease, metabolic liver disease, alpha-1-antitrypsin associated liver disease, and Wilson’s disease. These were ruled out using standard clinical, laboratory, and histological criteria.
Anthropometric data
Clinical variables were recorded, which included standard procedures for height and weight (Lohman et al. 1988). The body mass index (BMI) and its standard deviation score (Z score) were calculated (Kuczmarski et al. 2000). Obesity was defined by a BMI greater than or equal to 95th percentile adjusted for age and sex. Waist circumference was also measured, which was evaluated at the highest point of the iliac crest with a standing subject (Li et al. 2006). Waist circumference to height ratio was also calculated.
MetS in this cohort was defined as having three or more of the following five criteria: (1) abdominal obesity, defined as waist circumference (WC) ≥ 90th percentile for age (Fernandez et al. 2004); (2) low HDL-cholesterol, defined as concentrations <5th percentile for age and sex (American Academy of Pediatrics 1992); (3) hypertriglyceridemia, defined as triglyceride (TG) level >95th percentile for age and sex (American Academy of Pediatrics 1992); (4) hypertension, defined as systolic or diastolic blood pressure >95th percentile for age and sex (Report of the Second Task Force on Blood Pressure Control in Children 1987); and (5) impaired fasting glucose (≥110 mg/dL), impaired glucose tolerance or known type 2 diabetes mellitus (Genuth et al. 2003).
Laboratory assessment
Laboratory data collection included total cholesterol (TC), HDL cholesterol, triglycerides, aspartate aminotransferase (AST), alanine aminotransferase (ALT), serum γ-glutamyltransferase (GGT), total bilirubin, albumin, and INR. These were obtained and measured by standard laboratory methods. The non-HDL-C was calculated from the total cholesterol subtracted by the HDL cholesterol (non-HDL-C = TC – HDL). The homeostasis model assessment of insulin resistance (HOMA-IR) (Matthews et al. 1985) was calculated as markers for insulin sensitivity. None of the patients were on lipid-lowering medications at the time of the lipid profile measurements.
Liver histology
Liver biopsy was performed in all subjects because of the clinical indication to either assess the presence of NASH, degree of fibrosis, and/or to identify if other liver diseases were present. After an overnight fast, liver biopsy was performed under general anesthesia and ultrasound guidance utilizing the automatic core biopsy 18 gauge needle (Biopince, Amedic, Sweden). The Sonoline Omnia ultrasound machine (Siemens, Munich, Germany) was used, which is equipped with a 5-MHz probe (5.0 C 50, Siemens) and biopsy adaptor. For each subject, two biopsy passes in different liver segments were made, and the length of the liver specimen was recorded in millimeters. Only samples that included at least 5–6 complete portal tracts and with a length of ≥ 15 mm (Poynard et al. 2007) met the requirements for this study. Biopsies were routinely processed and staining of liver tissue included hematoxylin-eosin, Periodic acid-Schiff diastase, Van Gieson, and Prussian blue stain. A single hepatopathologist reviewed the biopsies and was blinded to the clinical and laboratory data.
Biopsies were evaluated by a single expert pediatric hepatopathologist who established the histopathological diagnosis of NASH. Based on this categorization patients were divided into two groups: 1) “NASH” or 2) diagnosis not compatible with NASH or “not NASH”. Liver histology was scored using the NAFLD activity scoring (NAS) system developed by the NASH Clinical Research Network (Kleiner et al. 2005). The grade of steatosis (0 – 3), hepatocyte ballooning (0 – 2), and lobular inflammation (0 – 3) were totaled to determine the NAS (0 – 8) score. Portal inflammation (PI) was graded from 0 to 2 (0 = no PI, 1 = mild PI, and 2 = more than mild PI). Mild PI was defined as a few mononuclear cells, usually in more than one portal tract. More than mild PI was defined as at least one portal area showing moderate to marked density of inflammation, and/or the presence of lymphoid aggregates. Fibrosis was staged as the following: 0 = no fibrosis, 1 = periportal or perisinusoidal, 2 = perisinusoidal and portal/periportal fibrosis, 3 = bridging fibrosis, and 4 = cirrhosis.
Statistical analysis
Descriptive statistics were performed for all variables. Categorical variables were presented as frequencies and percentages. Continuous variables were presented as mean ± standard deviation or median [25th, 75 percentiles]. Univariable analysis was performed to assess differences between subjects with and without NASH. Student’s t-tests or the non-parametric Wilcoxan rank sum tests were used to compare continuous or ordinal variables. Pearson’s chi-square tests were used for categorical factors. Spearman rank correlation coefficients (rho) were calculated to assess the correlation between non-HDL cholesterol levels and liver histology features (steatosis, ballooning, inflammation, and degree of fibrosis) and clinical characteristics. Analysis of covariance (ANCOVA) was used to adjust for possible confounders. All demographic and clinical factors were considered for inclusion in the model, and an automated stepwise variable selection was performed on 1,000 bootstrap samples to choose the final model. Variables with inclusion rates of at least 50% were included in the model. A p < 0.05 was considered statistically significant. All analyses were performed using SAS (version 9.2, The SAS Institute, Cary, NC) and R (version 2.13.1, The R Foundation for Statistical Computing, Vienna, Austria).
Results
Demographic and clinical characteristics
Three hundred and two children with biopsy-proven NAFLD were included in this study. Table 1 summarizes the anthropometric, clinical and laboratory data. There were 203 subjects with biopsy proven NASH (67.2%) and 99 subjects without NASH (32.8%). Of the total subjects, 36.4% were male, 63.6% were female. The mean age at initial visit for this study was 12.3 ± 3.1 years. Two hundred and sixty-eight (88.7%) children were found to be obese. One hundred and sixty-eight (55.6%) children were found to have MetS. Univariable analysis was performed, which showed that obesity, greater WC, hypercholesterolemia, hypertriglyceridemia, MetS, and higher non-HDL cholesterol were significantly associated with NASH. Total cholesterol and triglyceride levels were significantly higher in NASH patients; whereas, HDL-C levels were similar in the two groups. In addition, AST, GGT, and lower total bilirubin were also significantly associated with NASH.
Table 1 Demographic and clinical characteristics of subjects
Liver biopsy findings
Histologic features for subjects are represented in Table 2. As expected, subjects with NASH had higher NAS scores than those without. Majority of subjects with NASH had mild (134 subjects; 66%) or more than mild (21 subjects; 10.3%) portal inflammation, and ballooning was present in 135 subjects (66.5%). Lastly, in those patients with NASH, some degree of fibrosis was noted in majority of patients: mild fibrosis (grade 1) in 137 patients (67.5%); moderate fibrosis (grade 2) in 15 patients (7.4%); and advanced fibrosis (grade 3) in 18 patients (8.9%). None of these patients had liver cirrhosis. The mean NAS score in patients with NASH was 4.5 ± 1.4. In those patients without NASH, NAS was 2.2 ± 0.65, p <0.001.
Table 2 Histologic features
Non-HDL-C levels were higher in the NASH cohort and had positive correlation with histological features
Subjects with NASH were found to have significantly higher non-HDL-C levels than those without NASH (105.8 ± 40.2 versus 92.3 ± 32.8; p = 0.004) (Figure 1). Importantly, histologic features of pediatric NASH including lobular inflammation, portal inflammation, and ballooning had a positive correlation with non-HDL-C levels that was statistically significant (p = 0.005, p = 0.001, p = 0.01 respectively), and the NAS score was significantly associated with non-HDL-C (p = 0.024) as shown in Table 3. Moreover, fibrosis was also found to be positively correlated to non-HDL-C levels (Spearman’s rho of 0.25, 95% CI: 0.14, 0.36; p <0.001). The grade of steatosis, on the other hand, was not significantly associated with non-HDL-C. The association between non-HDL-C level and the histologic diagnosis of NASH was not significant after adjusting for MetS, WC/Height ratio, GGT and ALT in the multivariable analysis (Figure 2) (adjusted mean (95% CI): 102 (97.4, 106.6) vs 100.1 (93.4, 106.9); p = 0.66) implicating that other factors known to be associated with increased cardiovascular risk may explain the association noted in the univariable analysis.
Figure 1
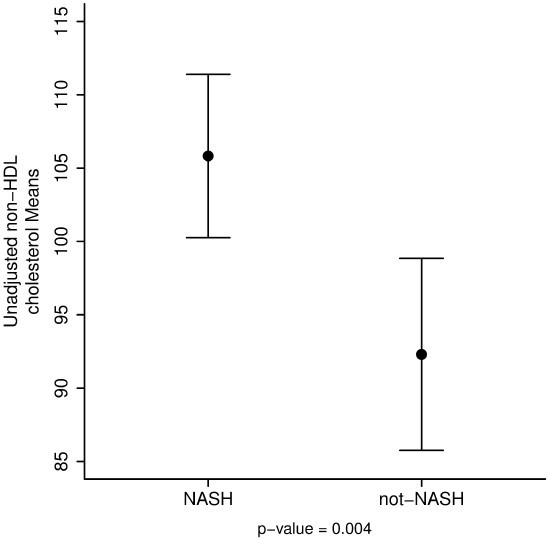
Unadjusted non-HDL cholesterol levels.
Table 3 Correlations between non-HDL cholesterol levels and histologic features
Figure 2
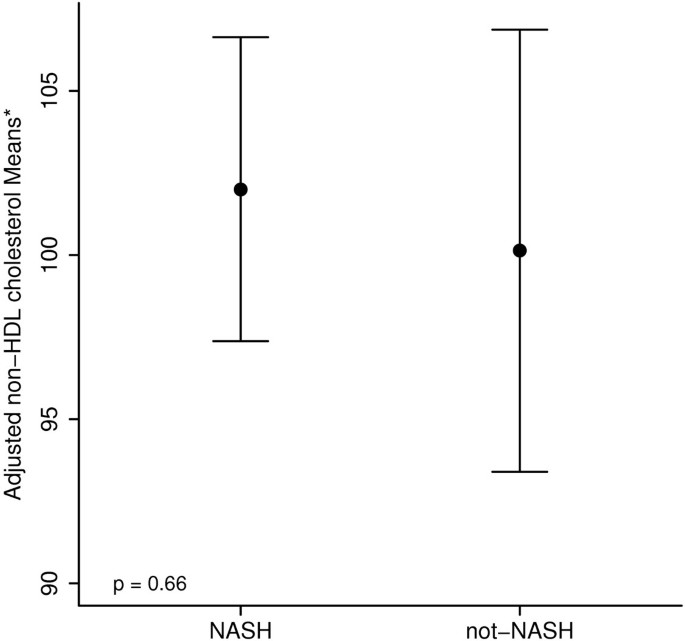
Adjusted non-HDL cholesterol levels.
Discussion
In this large study of pediatric patients with biopsy-proven NAFLD, our main findings have demonstrated that (1) non-HDL-C levels were higher in children with biopsy proven NASH as compared to children with simple steatosis and (2) histologic features of NASH, such as ballooning, lobular inflammation, portal inflammation and fibrosis were found to be correlated with non-HDL-C levels. This data has further extended the knowledge base of the cardiovascular complications of NASH in the pediatric population with NAFLD. The higher-non-HDL-C levels found in this study adds to prior studies that have shown an increased risk of CVD in patients with NASH. Interestingly, on multivariable analysis this finding did not hold when adjusting for MetS, WC/Height ratio (a measure of central obesity and associated with MetS) (Bener et al. 2013), GGT, and ALT. Given the lack of a significant difference of non-HDL-C in those patients with and without NASH on multivariable analysis, our study does not support non-HDL-C as a single biomarker for NASH. The etiology of this finding on multivariable analysis remains unclear, and while it may be more of a reflection of the increased prevalence of MetS in NASH, there is also a likely component of increased hepatic inflammation given the role that GGT and ALT have in this study’s multivariable analysis.
Studies in both adults and children have shown an association between NAFLD and CVD (Alkhouri et al. 2011; Targher 2007; Schwimmer et al. 2008). In one case control study of 150 overweight children with biopsy proven NAFLD versus those without, NAFLD was found to be strongly associated with risk factors for cardiovascular disease, including higher glucose, insulin, blood pressure, TC, LDL, triglyceride, and lower HDL. Furthermore, obese children with NAFLD were significantly more likely to have metabolic syndrome as compared to obese children without NAFLD (Schwimmer et al. 2008). Various adult studies have also looked at diagnostic markers for early atherosclerosis, which has included findings of a significant increase in carotid intima-media thickness (CIMT) in patients with NAFLD (Brea et al. 2005), with some CIMT studies even suggesting NAFLD to be an independent risk factor for developing atherosclerosis (Mohammadi et al. 2011; Li et al. 2012). Interestingly, while one pediatric study did not show CIMT to be associated with NAFLD in children (Manco et al. 2010), a recent pediatric study in 2012 showed CIMT to be significantly higher in patients with NAFLD as compared to obese and normal controls (Gokce et al. 2013). Other studies have also found impaired endothelial function and increased arterial stiffness in patients with NAFLD (Vlachopoulos et al. 2010; Villanova et al. 2005).
There continues to be a growing body of evidence that has shown an increased prevalence of CVD risk in patients with NAFLD, with additional studies showing that it can be independent of the presence of MetS or traditional risk factors (Alkhouri et al. 2011; Targher 2007; Targher et al. 2008a). A recent adult study found lipid ratios to be significantly associated with NAFLD, with a stepwise statistically significant difference between patients who had normal biopsies versus simple steatosis versus NASH. But more interestingly, the histologic severity of inflammation and liver injury appeared to be strongly associated with a more atherogenic lipid profile and increased CVD (Alkhouri et al. 2010). The atherogenic risk of NAFLD can be found not only in the adult population, but also in the pediatric population, with increased risk with progression of disease. A prior pediatric study from our institution evaluated 118 consecutive children with biopsy-proven NAFLD and found that the severity of liver injury and fibrosis was strongly associated with certain markers of atherogenic risk, in particular, ratios of cholesterol ester-rich lipoproteins such as TC/HDL, LDL/HDL, and TG/HDL. These lipid ratios were found to have a significant positive correlation with the NAFLD activity and fibrosis scores, with also a significant difference found between those with definitive NASH as compared to those with simple steatosis or borderline diagnosis. Additionally, this association was found to be independent of the presence of MetS, insulin resistance, and obesity (Nobili et al. 2010). In our current study we investigated CVD risk in obese children through non-HDL-C levels, which were found to be significantly higher in children with biopsy proven NASH as compared to those with simple steatosis. In addition, histologic features of NASH were also found to be correlated with non-HDL-C levels.
Potential biological mechanisms for a higher risk for atherosclerosis in NAFLD have been described, which includes increased systemic inflammation and oxidative stress. Markers, such as C-reactive protein (CRP) and fibrinogen levels, which are known to be inflammatory markers, are increased in patients with NAFLD, and particularly in those with NASH (Yoneda et al. 2007; Targher et al. 2008b). In our study, the significant difference of non-HDL-C in those patients with NASH versus simple steatosis highlights the cardiovascular implications of NASH. But in addition, the positive correlation of non-HDL-C levels with histologic scores of ballooning, inflammation, and fibrosis in NASH speaks towards the potential relationship between severity of hepatic damage and an atherogenic lipid profile.
Hepatic inflammation in it of itself is thought to be atherogenic, as studies have found a strong association between CVD and elevated ALT and GGT, which are surrogate markers of inflammation (Schindhelm et al. 2007; Lee et al. 2007; Ioannou et al. 2006). Recent animal studies have also suggested that hepatic insulin resistance and hepatic inflammation can also contribute to the development of dyslipidemia and increased cardiovascular disease risk (Guillen et al. 2008; Biddinger et al. 2008). In our study, the significance of non-HDL-C as a distinguishing marker for NASH on multivariate analysis was lost when controlling for such serum markers as GGT and ALT, which themselves are markers of inflammation and associated with cardiovascular risk.
It is also hypothesized that alterations in lipid metabolism may influence the development of steatosis versus NASH. Some recent studies have discussed the role of very low density lipoprotein (VLDL) and triglyceride production in the development of MetS and NASH (Choi and Ginsberg 2011; Choi and Diehl 2008; Fujita et al. 2009; Adiels et al. 2008). It is additionally thought that alterations in the exportation of triglycerides (packaged as VLDL and intermediate density lipoprotein (IDL)) may influence hepatic lipid storage and the development of NAFLD (Fujita et al. 2009; Choi et al. 2007; Yamaguchi et al. 2007). Unfortunately, direct measures of VLDL and IDL are not readily available to clinicians and are expensive. However, non-HDL-C is an indirect measure that encompasses both VLDL and IDL along with other lipoproteins, which include LDL, lipoprotein A, and chylomicrons. Our findings in this study may indirectly highlight the potential influence that VLDL and IDL may have on development of steatosis versus NASH.
The main strength of this study is the inclusion of a large group of over 300 children with biopsy-proven NAFLD that includes a full spectrum of the disease and varying degrees of fibrosis. None of the children in the current study were on lipid lower agents at the time of lipid measurement. In addition, there was an extensive characterization of anthropometric, metabolic, and histologic profile of these patients. To our knowledge, this is the first pediatric study to look at non-HDL-C in patients with NAFLD. However, this study has some limitations, which includes the fact that our patients were seen at a large referral tertiary care medical center, with a majority of our NAFLD patients having biopsy-proven NASH and a high prevalence rate of fibrosis. These findings therefore may not be generalizable to the pediatric population in the community. In addition, the majority of children were of Caucasian descent, thus the association between NAFLD and non-HDL-C may be different among other ethnicities. Lastly, this study is a cross-sectional study, thus it only showed an association between the severity of NAFLD and non-HDL-C, and thus could not infer causation.
In conclusion, non-HDL-C levels were found to be higher in children with NASH as compared to those with simple steatosis, suggestive of an increased risk for CVD. This may be more of a reflection of an increased prevalence of MetS in this population, but the increased hepatic inflammation of NASH may have played a role in the finding. Histologic features of NASH, such as ballooning, inflammation, and fibrosis were found to be correlated with non-HDL-C levels. Together, this continues to highlight again the association of NASH with increased CVD risk. Future studies would be beneficial to further evaluate the role of non-HDL-C and its association with increased CVD risk in children with NAFLD.
Informed consent and ethics committee approval
Informed consent was obtain in all patients. This study was approved by the responsible ethics committee of the Bambino Gesù Children’s Hospital and Research Institute.
Compliance with ethical requirements
All authors declare no conflict of interest for this study.
All procedures were followed in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Informed consent was obtained from all patients included in this study.
Abbreviations
NAFLD:
Nonalcoholic fatty liver disease
NASH:
Non-alcoholic steatohepatitis
non-HDL-C:
Non-high density lipoprotein cholesterol
NAS:
NAFLD activity score
CVD:
Cardiovascular disease
MetS:
Metabolic syndrome
BMI:
Body mass index
WC:
Waist circumference
HOMA-IR:
Homeostasis model assessment index of insulin resistance
IGT:
Impaired glucose tolerance
TG:
Triglycerides
IDL:
Intermediate density lipoprotein
LDL:
Low density lipoprotein
AST:
Aspartate aminotransferase
ALT:
Alanine aminotransferase
GGT:
Serum γ-glutamyltransferase
INR:
International normalized ratio
ANCOVA:
Analysis of covariance
CIMT:
Carotid intima-media thickness
PI:
Portal inflammation.
References
- Abdelmalek MF, Diehl AM: Nonalcoholic fatty liver disease as a complication of insulin resistance. Med Clin North Am 2007, 91: 1125-1149. ix
Article Google Scholar - Adiels M, Olofsson SO, Taskinen MR, Boren J: Overproduction of very low-density lipoproteins is the hallmark of the dyslipidemia in the metabolic syndrome. Arterioscler Thromb Vasc Biol 2008, 28: 1225-1236.
Article Google Scholar - Alkhouri N, Tamimi TA, Yerian L, Lopez R, Zein NN, Feldstein AE: The inflamed liver and atherosclerosis: a link between histologic severity of nonalcoholic fatty liver disease and increased cardiovascular risk. Dig Dis Sci 2010, 55: 2644-2650.
Article Google Scholar - Alkhouri N, Carter-Kent C, Elias M, Feldstein AE: Atherogenic dyslipidemia and cardiovascular risk in children with nonalcoholic fatty liver disease. Clin Lipidol 2011, 6: 305-314.
Article Google Scholar - American Academy of Pediatrics: National cholesterol education program: report of the expert panel on blood cholesterol levels in children and adolescents. Pediatrics 1992, 89: 525-584.
Google Scholar - Bener A, Yousafzai MT, Darwish S, Al-Hamaq AO, Nasralla EA, Abdul-Ghani M: Obesity index that better predict metabolic syndrome: body mass index, waist circumference, waist hip ratio, or waist height ratio. J Obes 2013, 2013: 269038.
Article Google Scholar - Biddinger SB, Hernandez-Ono A, Rask-Madsen C, Haas JT, Aleman JO, Suzuki R, Scapa EF, Agarwal C, Carey MC, Stephanopoulos G, Cohen DE, King GL, Ginsberg HN, Kahn CR: Hepatic insulin resistance is sufficient to produce dyslipidemia and susceptibility to atherosclerosis. Cell Metab 2008, 7: 125-134.
Article Google Scholar - Brea A, Mosquera D, Martin E, Arizti A, Cordero JL, Ros E: Nonalcoholic fatty liver disease is associated with carotid atherosclerosis: a case–control study. Arterioscler Thromb Vasc Biol 2005, 25: 1045-1050.
Article Google Scholar - Brunzell JD, Davidson M, Furberg CD, Goldberg RB, Howard BV, Stein JH, Witztum JL: Lipoprotein management in patients with cardiometabolic risk: consensus conference report from the American Diabetes Association and the American College of Cardiology Foundation. J Am Coll Cardiol 2008, 51: 1512-1524.
Article Google Scholar - Chan DF, Li AM, Chu WC, Chan MH, Wong EM, Liu EK, Chan IH, Yin J, Lam CW, Fok TF, Nelson EA: Hepatic steatosis in obese Chinese children. Int J Obes Relat Metab Disord 2004, 28: 1257-1263.
Article Google Scholar - Choi SS, Diehl AM: Hepatic triglyceride synthesis and nonalcoholic fatty liver disease. Curr Opin Lipidol 2008, 19: 295-300.
Article Google Scholar - Choi SH, Ginsberg HN: Increased very low density lipoprotein (VLDL) secretion, hepatic steatosis, and insulin resistance. Trends Endocrinol Metab 2011, 22: 353-363.
Article Google Scholar - Choi CS, Savage DB, Kulkarni A, Yu XX, Liu ZX, Morino K, Kim S, Distefano A, Samuel VT, Neschen S, Zhang D, Wang A, Zhang XM, Kahn M, Cline GW, Pandey SK, Geisler JG, Bhanot S, Monia BP, Shulman GI: Suppression of diacylglycerol acyltransferase-2 (DGAT2), but not DGAT1, with antisense oligonucleotides reverses diet-induced hepatic steatosis and insulin resistance. J Biol Chem 2007, 282: 22678-22688.
Article Google Scholar - Corey KE, Lai M, Gelrud LG, Misdraji J, Barlow LL, Zheng H, Andersson KL, Thiim M, Pratt DS, Chung RT: Non-high-density lipoprotein cholesterol as a biomarker for nonalcoholic steatohepatitis. Clin Gastroenterol Hepatol 2012, 10: 651-656.
Article Google Scholar - Feldstein AE, Charatcharoenwitthaya P, Treeprasertsuk S, Benson JT, Enders FB, Angulo P: The natural history of non-alcoholic fatty liver disease in children: a follow-up study for up to 20 years. Gut 2009, 58: 1538-1544.
Article Google Scholar - Fernandez JR, Redden DT, Pietrobelli A, Allison DB: Waist circumference percentiles in nationally representative samples of African-American, European-American, and Mexican-American children and adolescents. J Pediatr 2004, 145: 439-444.
Article Google Scholar - Fujita K, Nozaki Y, Wada K, Yoneda M, Fujimoto Y, Fujitake M, Endo H, Takahashi H, Inamori M, Kobayashi N, Kirikoshi H, Kubota K, Saito S, Nakajima A: Dysfunctional very-low-density lipoprotein synthesis and release is a key factor in nonalcoholic steatohepatitis pathogenesis. Hepatology 2009, 50: 772-780.
Article Google Scholar - Genuth S, Alberti KG, Bennett P, Buse J, Defronzo R, Kahn R, Kitzmiller J, Knowler WC, Lebovitz H, Lernmark A, Nathan D, Palmer J, Rizza R, Saudek C, Shaw J, Steffes M, Stern M, Tuomilehto J, Zimmet P, Expert Committee on the Diagnosis and Classification of Diabetes Mellitus: Follow-up report on the diagnosis of diabetes mellitus. Diabetes Care 2003, 26: 3160-3167.
Article Google Scholar - Gokce S, Atbinici Z, Aycan Z, Cinar HG, Zorlu P: The relationship between pediatric nonalcoholic fatty liver disease and cardiovascular risk factors and increased risk of atherosclerosis in obese children. Pediatr Cardiol 2013, 34(2):308-315.
Article Google Scholar - Grundy SM, Cleeman JI, Merz CN, Brewer HB Jr, Clark LT, Hunninghake DB, Pasternak RC, Smith SC Jr, Stone NJ, Coordinating Committee of the National Cholesterol Education Program: Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines. J Am Coll Cardiol 2004, 44: 720-732.
Article Google Scholar - Guillen N, Acin S, Navarro MA, Perona JS, Arbones-Mainar JM, Arnal C, Sarria AJ, Surra JC, Carnicer R, Orman I, Segovia JC, Ruiz-Gutierrez V, Osada J: Squalene in a sex-dependent manner modulates atherosclerotic lesion which correlates with hepatic fat content in apoE-knockout male mice. Atherosclerosis 2008, 197: 72-83.
Article Google Scholar - Ioannou GN, Weiss NS, Boyko EJ, Mozaffarian D, Lee SP: Elevated serum alanine aminotransferase activity and calculated risk of coronary heart disease in the United States. Hepatology 2006, 43: 1145-1151.
Article Google Scholar - Kleiner DE, Brunt EM, Van Natta M, Behling C, Contos MJ, Cummings OW, Ferrell LD, Liu YC, Torbenson MS, Unalp-Arida A, Yeh M, McCullough AJ, Sanyal AJ, Nonalcoholic Steatohepatitis Clinical Research Network: Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41: 1313-1321.
Article Google Scholar - Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, Flegal KM, Guo SS, Wei R, Mei Z, Curtin LR, Roche AF, Johnson CL: CDC growth charts: United States. Adv Data 2000, 8(314):1-27.
Google Scholar - Lee DS, Evans JC, Robins SJ, Wilson PW, Albano I, Fox CS, Wang TJ, Benjamin EJ, D’Agostino RB, Vasan RS: Gamma glutamyl transferase and metabolic syndrome, cardiovascular disease, and mortality risk: the Framingham heart study. Arterioscler Thromb Vasc Biol 2007, 27: 127-133.
Article Google Scholar - Li C, Ford ES, Mokdad AH, Cook S: Recent trends in waist circumference and waist-height ratio among US children and adolescents. Pediatrics 2006, 118: e1390-e1398.
Article Google Scholar - Li X, Xia M, Ma H, Hofman A, Hu Y, Yan H, He W, Lin H, Jeekel J, Zhao N, Gao J, Gao X: Liver fat content is associated with increased carotid atherosclerosis in a Chinese middle-aged and elderly population: the Shanghai Changfeng study. Atherosclerosis 2012, 224: 480-485.
Article Google Scholar - Lohman TG, Roche AF, Martorell R: Anthropometric standardization reference manual. Human Kinetics Books, Champaign, IL; 1988:177.
Google Scholar - Manco M, Bedogni G, Monti L, Morino G, Natali G, Nobili V: Intima-media thickness and liver histology in obese children and adolescents with non-alcoholic fatty liver disease. Atherosclerosis 2010, 209: 463-468.
Article Google Scholar - Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC: Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28: 412-419.
Article Google Scholar - Mohammadi A, Bazazi A, Ghasemi-Rad M: Evaluation of atherosclerotic findings in patients with nonalcoholic fatty liver disease. Int J Gen Med 2011, 4: 717-722.
Article Google Scholar - Nobili V, Alkhouri N, Bartuli A, Manco M, Lopez R, Alisi A, Feldstein AE: Severity of liver injury and atherogenic lipid profile in children with nonalcoholic fatty liver disease. Pediatr Res 2010, 67: 665-670.
Article Google Scholar - Orakzai SH, Nasir K, Blaha M, Blumenthal RS, Raggi P: Non-HDL cholesterol is strongly associated with coronary artery calcification in asymptomatic individuals. Atherosclerosis 2009, 202: 289-295.
Article Google Scholar - Pagano G, Pacini G, Musso G, Gambino R, Mecca F, Depetris N, Cassader M, David E, Cavallo-Perin P, Rizzetto M: Nonalcoholic steatohepatitis, insulin resistance, and metabolic syndrome: further evidence for an etiologic association. Hepatology 2002, 35: 367-372.
Article Google Scholar - Poynard T, Halfon P, Castera L, Charlotte F, Le Bail B, Munteanu M, Messous D, Ratziu V, Benhamou Y, Bourliere M, De Ledinghen V, FibroPaca Group: Variability of the area under the receiver operating characteristic curves in the diagnostic evaluation of liver fibrosis markers: impact of biopsy length and fragmentation. Aliment Pharmacol Ther 2007, 25: 733-739.
Article Google Scholar - Report of the Second Task Force on Blood Pressure Control in Children: Task force on blood pressure control in children. National heart, lung, and blood institute, Bethesda, Maryland. Pediatrics 1987, 79: 1-25.
Google Scholar - Schindhelm RK, Dekker JM, Nijpels G, Bouter LM, Stehouwer CD, Heine RJ, Diamant M: Alanine aminotransferase predicts coronary heart disease events: a 10-year follow-up of the Hoorn study. Atherosclerosis 2007, 191: 391-396.
Article Google Scholar - Schwimmer JB, Deutsch R, Kahen T, Lavine JE, Stanley C, Behling C: Prevalence of fatty liver in children and adolescents. Pediatrics 2006, 118: 1388-1393.
Article Google Scholar - Schwimmer JB, Pardee PE, Lavine JE, Blumkin AK, Cook S: Cardiovascular risk factors and the metabolic syndrome in pediatric nonalcoholic fatty liver disease. Circulation 2008, 118: 277-283.
Article Google Scholar - Targher G: Non-alcoholic fatty liver disease, the metabolic syndrome and the risk of cardiovascular disease: the plot thickens. Diabet Med 2007, 24: 1-6.
Article Google Scholar - Targher G, Marra F, Marchesini G: Increased risk of cardiovascular disease in non-alcoholic fatty liver disease: causal effect or epiphenomenon? Diabetologia 2008, 51: 1947-1953.
Article Google Scholar - Targher G, Bertolini L, Rodella S, Lippi G, Franchini M, Zoppini G, Muggeo M, Day CP: NASH predicts plasma inflammatory biomarkers independently of visceral fat in men. Obesity (Silver Spring) 2008, 16: 1394-1399.
Article Google Scholar - Vajro P, Lenta S, Socha P, Dhawan A, McKiernan P, Baumann U, Durmaz O, Lacaille F, McLin V, Nobili V: Diagnosis of nonalcoholic fatty liver disease in children and adolescents: position paper of the ESPGHAN Hepatology Committee. J Pediatr Gastroenterol Nutr 2012, 54: 700-713.
Article Google Scholar - Villanova N, Moscatiello S, Ramilli S, Bugianesi E, Magalotti D, Vanni E, Zoli M, Marchesini G: Endothelial dysfunction and cardiovascular risk profile in nonalcoholic fatty liver disease. Hepatology 2005, 42: 473-480.
Article Google Scholar - Vlachopoulos C, Manesis E, Baou K, Papatheodoridis G, Koskinas J, Tiniakos D, Aznaouridis K, Archimandritis A, Stefanadis C: Increased arterial stiffness and impaired endothelial function in nonalcoholic Fatty liver disease: a pilot study. Am J Hypertens 2010, 23: 1183-1189.
Article Google Scholar - Wieckowska A, Feldstein AE: Nonalcoholic fatty liver disease in the pediatric population: a review. Curr Opin Pediatr 2005, 17: 636-641.
Article Google Scholar - Yamaguchi K, Yang L, McCall S, Huang J, Yu XX, Pandey SK, Bhanot S, Monia BP, Li YX, Diehl AM: Inhibiting triglyceride synthesis improves hepatic steatosis but exacerbates liver damage and fibrosis in obese mice with nonalcoholic steatohepatitis. Hepatology 2007, 45: 1366-1374.
Article Google Scholar - Yoneda M, Mawatari H, Fujita K, Iida H, Yonemitsu K, Kato S, Takahashi H, Kirikoshi H, Inamori M, Nozaki Y, Abe Y, Kubota K, Saito S, Iwasaki T, Terauchi Y, Togo S, Maeyama S, Nakajima A: High-sensitivity C-reactive protein is an independent clinical feature of nonalcoholic steatohepatitis (NASH) and also of the severity of fibrosis in NASH. J Gastroenterol 2007, 42: 573-582.
Article Google Scholar
Author information
Authors and Affiliations
- Department of Pediatric Gastroenterology, Cleveland Clinic, 9500 Euclid Avenue, A111, Cleveland, OH, 44195, USA
Naim Alkhouri & Katharien Eng - Digestive Disease Institute, Cleveland Clinic, 9500 Euclid Avenue, A51, Cleveland, OH, 44195, USA
Naim Alkhouri - Quantitative Health Sciences, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH, 44195, USA
Rocio Lopez - Liver Unit, Bambino Gesù Children’s Hospital and Research Institute, 37 Salita di Sant’onofrio, 00165, Rome, Italy
Valerio Nobili
Authors
- Naim Alkhouri
- Katharien Eng
- Rocio Lopez
- Valerio Nobili
Corresponding author
Correspondence toNaim Alkhouri.
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
KE, RL, VN and NA were involved in developing study concept and design; acquisition of data; analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Alkhouri, N., Eng, K., Lopez, R. et al. Non-high-density lipoprotein cholesterol (non-HDL-C) levels in children with nonalcoholic fatty liver disease (NAFLD).SpringerPlus 3, 407 (2014). https://doi.org/10.1186/2193-1801-3-407
- Received: 27 January 2014
- Accepted: 16 July 2014
- Published: 05 August 2014
- DOI: https://doi.org/10.1186/2193-1801-3-407