Burkitt Lymphoma and Burkitt-like Lymphoma Workup: Approach Considerations, Diagnostic Studies, Radiologic Studies (original) (raw)
Approach Considerations
The least invasive procedure should be used to establish the diagnosis, which usually involves pathologic evaluation of the involved tissue biopsy. The staging workup must be expedited, because Burkitt tumor grows rapidly, causing life-threatening complications.
A diagnosis can sometimes be made by bone marrow aspiration and biopsy if the marrow is involved. If the marrow is not involved, diagnosis will require sampling lymph nodes or the involved extranodal site.
The detection of the classic reciprocal c-myc translocations as well as is not always feasible on routine cytogenetics studies; the use of fluorescence in situ hybridization (FISH) and polymerase chain reaction (PCR) can be very helpful in detecting the presence of c-myc translocations in those cases. [51]
Flow cytometry of biopsied tissue or bone marrow may reveal expression of surface immunoglobulin M (IgM) (most common), as well as other mature B-cell markers, such as the following:
- CD19
- CD20
- CD22
- CD79a
- CD10
In contrast, Tdt, CD5, CD23, and CD34 are negative.
![]()
Diagnostic Studies
General laboratory studies should include complete blood cell (CBC) count with differentials; a platelet count; serum levels of electrolytes, uric acid, lactate dehydrogenase (LDH), and creatinine; and liver function tests. All patients should also be checked for human immunodeficiency virus (HIV) and hepatitis B (HBV) infection.
CBC count and coagulation studies
CBC counts may reveal pancytopenia (anemia, thrombocytopenia, and/or leukopenia) due to the involvement of the bone marrow. Coagulation studies (prothrombin time [PT], partial thromboplastin time [PTT], and fibrinogen) should be performed to evaluate the presence of disseminated intravascular coagulopathy (DIC).
Serum chemistries
Electrolyte imbalances occur as a result of renal infiltration with lymphoma. The rapid turnover of the Burkitt lymphoma (BL) cells may cause primary tumor lysis, which is characterized by hyperkalemia, hyperphosphatemia, hyperuricemia, and hypocalcemia—with resultant uric acid nephropathy and oliguric renal failure.
Serum lactate dehydrogenase (LDH) levels are almost always elevated, often to extreme levels. The diagnosis of Burkitt lymphoma (BL) should be considered in any patient with a marked elevation of LDH. This test is also a useful indicator of the patient's response to treatment and can be used as an early nonspecific indicator of disease relapse.
Liver function test results, if abnormal, may be indicative of visceral involvement with lymphoma.
Serum uric acid levels are often high and reflect the high-grade nature of the disease and correlate with the probability of tumor lysis syndrome with initiation of cytotoxic therapy.
Beta2 microglobulin is a predictor of the extent of disease and is used as a surrogate marker for early relapse.
![]()
Radiologic Studies
Imaging studies help assess tumor burden and measurement of tumor masses before therapy. Head or spinal computed tomography (CT) scanning or magnetic resonance imaging (MRI) is indicated if neurologic signs and symptoms are present (see the following images), whereas bone scanning and plain bone radiography are needed for patients with symptoms of bone involvement. These imaging studies are helpful in evaluating the extent of disease and used in assessing sites of relapse. Although complete staging is helpful in assessing the patient, treatment should not be delayed while extensive tests are performed.

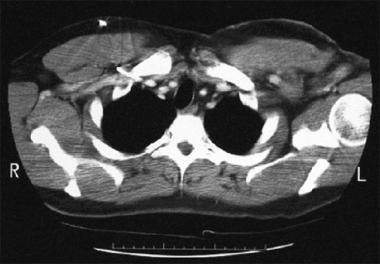
Computed tomography scan in a patient with a large, left-sided axillary mass from which a biopsy was obtained. Biopsy findings were consistent with small noncleaved cell non-Hodgkin lymphoma.
Postchemotherapy computed tomography scan in a patient diagnosed with small noncleaved cell lymphoma (SNCCL) (same patient as in previous image). This image shows regression of a left axillary mass.
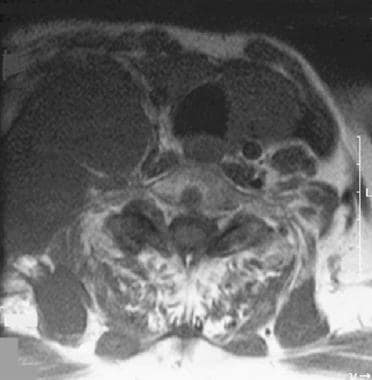
Coronal magnetic resonance imaging (MRI) section in a patient with large neck mass (same patient as in previous image). Biopsy findings showed Burkitt-like non-Hodgkin lymphoma (NHL). MRI was performed to assess for cord involvement.

Sagittal magnetic resonance imaging (MRI) section of the neck area showing a large mass invading the cervical spine with epidural encroachment (same patient as in the previous image). MRI was performed to rule out cord compression. The first image shows the gallium scan of this patient that correlates with the site of the tumor.

Right-sided pleural effusion in a patient with small noncleaved cell lymphoma (SNCCL) non-Hodgkin lymphoma.
Obtain a CT scan of the chest, abdomen, and pelvis with intravenous contrast. If the patient has evidence of renal insufficiency due to hyperuricemia, obstruction, or renal infiltration, then intravenous (IV) contrast medium should be omitted.
Positron emission tomography (PET) scanning has been reported to be very useful in staging non-Hodgkin lymphomas (NHL) and monitoring treatment response, but this modality is unlikely to alter management in Burkitt lymphoma (BL), therefore, it is reserved for use in clinical trials.
Cardiac imaging studies
Echocardiography (ECG) is indicated for possible arrhythmia resulting from cardiac involvement.
Multiple-gate acquisition (MUGA) scanning is used to evaluate the ejection fraction before chemotherapy treatment, especially if anthracyclines will be used, as these agents have a potential cardiotoxic effect.
![]()
Diagnostic Procedures and Associated Studies
The diagnosis of Burkitt lymphoma (BL) or Burkitt-like lymphoma (BLL) is made by obtaining a biopsy of the tumor mass for histopathology, immunochemistry, and flow cytometry (see the following image). Cytogenetic studies to identify c-myc mutation will aid in the diagnosis. The most suggestive lymph nodes should be selected for excisional biopsy. Frozen sections and needle biopsies are discouraged. Aspiration of bone marrow or effusions may provide the diagnosis and avoid lymph node biopsy.
A unilateral bone marrow aspirate and biopsy should be performed for every patient with Burkitt lymphoma (BL), because the frequent presence of unexpected bone marrow involvement has important implications for treatment planning. If lymphoma cells are present in the aspirate, flow cytometry/immunophenotyping should be ordered to further characterize the disease. Bone marrow is involved in 20% of sporadic cases and 8% of endemic cases of Burkitt lymphoma (eBL).
Lumbar puncture (LP) is considered part of the staging workup to evaluate for cerebrospinal fluid (CSF) involvement. This test should be deferred in the presence of significant thrombocytopenia or coagulation defects. The CSF should be sent for cytology and flow cytometry evaluation in addition to the usual studies. Intrathecal chemotherapy is usually given at the time of the initial lumbar puncture.
Paracentesis or thoracentesis may be needed for cytogenetic studies if ascites or pleural effusion is present.
Years ago, laparotomy was indicated for the initial diagnosis and for resection of the disease; this procedure is not recommended by current guidelines.
![]()
Histologic Features
Burkitt cells are homogeneous in size and shape, with round to oval nuclei and slightly coarse chromatin, with multiple nucleoli, and with intensely basophilic vacuolated cytoplasm that contains neutral fat. Extranodal involvement shows infiltration with monotonous cells of uniform size and shape. The cytoplasm is scanty, and the nucleus is round or slightly irregular with slightly coarse chromatin and several nucleoli.
Burkitt lymphoma
Histologically, Burkitt lymphoma (BL) is characterized by a monoclonal proliferation of medium-sized, noncleaved B-cells that are uniform in appearance and that produce a diffuse pattern of tissue involvement. These cells typically have a scant basophilic cytoplasm characterized by numerous lipid vacuoles, round nuclei with stippled chromatin and multiple small nucleoli.
Under the microscope, the hallmark of Burkitt lymphoma (BL) is the presence of a "starry sky" appearance (also observed in other highly proliferative lymphomas), imparted by scattered macrophages phagocytizing cell debris and apoptotic cells (tingible body macrophages) (see the image below). [2] However, the starry sky pattern is not pathognomonic for Burkitt lymphoma (BL) and may be observed in other highly proliferative lymphomas. Immunophenotype and cytogenetic studies aid in the diagnosis of Burkitt lymphoma (BL). [2, 46]
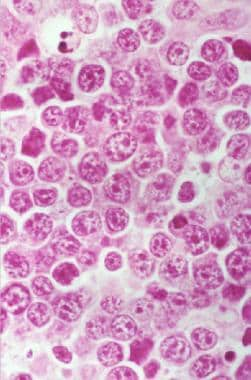
Hematoxylin and eosin (H&E) stain. Sheets of monotonous-appearing lymphoid cells with one or more prominent nucleoli and an area of pale staining resulting from the presence of benign macrophages reveal a starry sky pattern.
Burkitt lymphoma (BL) tumor cells are derived from mutated activated germinal center B-lymphocytes based on the fact that they share the same surface markers such as CD10, CD77, and bcl-6 (nuclear staining only) and the presence of somatic mutations in their immunoglobulins gene, similar to normal germinal center B cells. [52] They also express other B-cell antigens like CD10, CD19, CD20, CD22, as well as HLA-DR and surface immunoglobulin M (IgM) (see the image below). Ki67 staining usually approaches 100%. They typically lack CD5, CD23, TdT and are usually bcl-2 negative. [2] Expression of CD21 (Epstein-Barr virus [EBV]-C3d receptor) is present only in EBV-positive patients (endemic BL). [53]
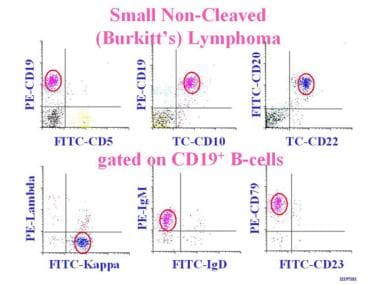
The 2-dimensional flow cytometry demonstrates the highlighted cells to be CD5 negative and CD23 negative as well as lambda negative. Small noncleaved cell lymphoma (SNCCL) cells are typically CD19+, CD20+, CD22+, and CD10+.
Burkitt-like lymphoma
Burkitt-like lymphoma (BLL), a subcategory of Burkitt lymphoma (BL) in the World Health Organization (WHO) classification, has greater polymorphism in the nuclear size and shape, and the expression of surface markers is more variable. Morphologically, these tumors have features that are intermediate between diffuse large B-cell lymphoma (DLBCL) and classic Burkitt lymphoma (BL), with some large cells resembling DLBCL and other, smaller cells resembling typical BL cells. They are also characterized by a high proliferation rate, a starry-sky pattern, and an immunophenotype similar to classic Burkitt lymphoma (BL). [54]
The WHO describes cases that are morphologically typical of Burkitt lymphoma (BL) but that have an atypical immunophenotype or genetic features. Around 35-50% of these cases have 8q24/c-myc translocations, and approximately 15% have bcl-2 translocations (double hit lymphoma). Interestingly, not all c-myc translocations in Burkitt-like lymphoma (BLL) patients involve immunoglobulin loci (Non IG-MYC). [46]
![]()
- Molyneux EM, Rochford R, Griffin B, Newton R, Jackson G, Menon G, et al. Burkitt's lymphoma. Lancet. 2012 Mar 31. 379 (9822):1234-44. [QxMD MEDLINE Link].
- Swerdlow SH, Campo E, Pileri SA, Harris NL, Stein H, Siebert R, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016 May 19. 127 (20):2375-90. [QxMD MEDLINE Link]. [Full Text].
- Gong JZ, Stenzel TT, Bennett ER, et al. Burkitt lymphoma arising in organ transplant recipients: a clinicopathologic study of five cases. Am J Surg Pathol. 2003 Jun. 27(6):818-27. [QxMD MEDLINE Link].
- Husain M, Grunebaum E, Naqvi A, et al. Burkitt's lymphoma in a patient with adenosine deaminase deficiency-severe combined immunodeficiency treated with polyethylene glycol-adenosine deaminase. J Pediatr. 2007 Jul. 151(1):93-5. [QxMD MEDLINE Link].
- Ferry JA. Burkitt's lymphoma: clinicopathologic features and differential diagnosis. Oncologist. 2006 Apr. 11(4):375-83. [QxMD MEDLINE Link].
- Blum KA, Lozanski G, Byrd JC. Adult Burkitt leukemia and lymphoma. Blood. 2004 Nov 15. 104(10):3009-20. [QxMD MEDLINE Link].
- Burkitt DP. Classics in oncology. A sarcoma involving the jaws in African children. CA Cancer J Clin. 1972 Nov-Dec. 22(6):345-55. [QxMD MEDLINE Link].
- Burkitt D, O'Conor GT. Malignant lymphoma in African children. I. A clinical syndrome. Cancer. 1961 Mar-Apr. 14:258-69. [QxMD MEDLINE Link].
- Epstein MA, Achong BG, Barr YM. Virus particles in cultured lymphoblasts from Burkitt's lymphoma. Lancet. 1964 Mar 28. 1(7335):702-3. [QxMD MEDLINE Link].
- Magrath I. The pathogenesis of Burkitt's lymphoma. Adv Cancer Res. 1990. 55:133-270. [QxMD MEDLINE Link].
- Magrath IT. African Burkitt's lymphoma. History, biology, clinical features, and treatment. Am J Pediatr Hematol Oncol. 1991 Summer. 13(2):222-46. [QxMD MEDLINE Link].
- Summerauer AM, Jäggi V, Ogwang R, Traxel S, Colombo L, Amundsen E, et al. Epstein-Barr virus and malaria upregulate AID and APOBEC3 enzymes, but only AID seems to play a major mutagenic role in Burkitt lymphoma. Eur J Immunol. 2022 May 3. 22 (1):45. [QxMD MEDLINE Link].
- De Falco G, Antonicelli G, Onnis A, Lazzi S, Bellan C, Leoncini L. Role of EBV in microRNA dysregulation in Burkitt lymphoma. Semin Cancer Biol. 2009 Dec. 19(6):401-6. [QxMD MEDLINE Link].
- Thorley-Lawson DA, Allday MJ. The curious case of the tumour virus: 50 years of Burkitt's lymphoma. Nat Rev Microbiol. 2008 Dec. 6(12):913-24. [QxMD MEDLINE Link].
- Preudhomme C, Dervite I, Wattel E, et al. Clinical significance of p53 mutations in newly diagnosed Burkitt's lymphoma and acute lymphoblastic leukemia: a report of 48 cases. J Clin Oncol. 1995 Apr. 13(4):812-20. [QxMD MEDLINE Link].
- Gaidano G, Ballerini P, Gong JZ, et al. p53 mutations in human lymphoid malignancies: association with Burkitt lymphoma and chronic lymphocytic leukemia. Proc Natl Acad Sci U S A. 1991 Jun 15. 88(12):5413-7. [QxMD MEDLINE Link]. [Full Text].
- Dang CV, Resar LM, Emison E, et al. Function of the c-Myc oncogenic transcription factor. Exp Cell Res. 1999 Nov 25. 253(1):63-77. [QxMD MEDLINE Link].
- Dang CV, O'Donnell KA, Juopperi T. The great MYC escape in tumorigenesis. Cancer Cell. 2005 Sep. 8(3):177-8. [QxMD MEDLINE Link].
- Coller HA, Grandori C, Tamayo P, et al. Expression analysis with oligonucleotide microarrays reveals that MYC regulates genes involved in growth, cell cycle, signaling, and adhesion. Proc Natl Acad Sci U S A. 2000 Mar 28. 97(7):3260-5. [QxMD MEDLINE Link]. [Full Text].
- Molina-Privado I, Rodriguez-Martinez M, Rebollo P, et al. E2F1 expression is deregulated and plays an oncogenic role in sporadic Burkitt's lymphoma. Cancer Res. 2009 May 1. 69(9):4052-8. [QxMD MEDLINE Link]. [Full Text].
- Love C, Sun Z, Jima D, et al. The genetic landscape of mutations in Burkitt lymphoma. Nat Genet. 2012 Dec. 44 (12):1321-5. [QxMD MEDLINE Link]. [Full Text].
- Richter J, et al; ICGC MMML-Seq Project. Recurrent mutation of the ID3 gene in Burkitt lymphoma identified by integrated genome, exome and transcriptome sequencing. Nat Genet. 2012 Dec. 44 (12):1316-20. [QxMD MEDLINE Link].
- Davi F, Delecluse HJ, Guiet P, et al. Burkitt-like lymphomas in AIDS patients: characterization within a series of 103 human immunodeficiency virus-associated non-Hodgkin's lymphomas. Burkitt's Lymphoma Study Group. J Clin Oncol. 1998 Dec. 16(12):3788-95. [QxMD MEDLINE Link].
- Cardy HA, Sharp L, Little J. Burkitt's lymphoma: a review of the epidemiology. Kuwait Med J. 2001. 33:293-306.
- Makata AM, Toriyama K, Kamidigo NO, Eto H, Itakura H. The pattern of pediatric solid malignant tumors in western Kenya, east Africa, 1979-1994: an analysis based on histopathologic study. Am J Trop Med Hyg. 1996 Apr. 54(4):343-7. [QxMD MEDLINE Link].
- Swerdlow SH, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th Edition. Lyon, France: International Agency for Research on Cancer; 2008.
- Havelange V, Pepermans X, Ameye G, Théate I, Callet-Bauchu E, Barin C, et al. Genetic differences between paediatric and adult Burkitt lymphomas. Br J Haematol. 2016 Apr. 173 (1):137-44. [QxMD MEDLINE Link].
- Ladenstein R, Pearce R, Hartmann O, Patte C, Goldstone T, Philip T. High-dose chemotherapy with autologous bone marrow rescue in children with poor-risk Burkitt's lymphoma: a report from the European Lymphoma Bone Marrow Transplantation Registry. Blood. 1997 Oct 15. 90(8):2921-30. [QxMD MEDLINE Link].
- Thomas DA, Faderl S, O'Brien S, et al. Chemoimmunotherapy with hyper-CVAD plus rituximab for the treatment of adult Burkitt and Burkitt-type lymphoma or acute lymphoblastic leukemia. Cancer. 2006 Apr 1. 106(7):1569-80. [QxMD MEDLINE Link].
- Magrath I, Adde M, Shad A, et al. Adults and children with small non-cleaved-cell lymphoma have a similar excellent outcome when treated with the same chemotherapy regimen. J Clin Oncol. 1996 Mar. 14(3):925-34. [QxMD MEDLINE Link].
- Kantarjian HM, Walters RS, Keating MJ, et al. Results of the vincristine, doxorubicin, and dexamethasone regimen in adults with standard- and high-risk acute lymphocytic leukemia. J Clin Oncol. 1990 Jun. 8(6):994-1004. [QxMD MEDLINE Link].
- Ostronoff M, Soussain C, Zambon E, et al. Burkitt's lymphoma in adults: a retrospective study of 46 cases. Nouv Rev Fr Hematol. 1992. 34(5):389-97. [QxMD MEDLINE Link].
- Hoelzer D, Ludwig WD, Thiel E, et al. Improved outcome in adult B-cell acute lymphoblastic leukemia. Blood. 1996 Jan 15. 87(2):495-508. [QxMD MEDLINE Link].
- McMaster ML, Greer JP, Greco FA, Johnson DH, Wolff SN, Hainsworth JD. Effective treatment of small-noncleaved-cell lymphoma with high-intensity, brief-duration chemotherapy. J Clin Oncol. 1991 Jun. 9(6):941-6. [QxMD MEDLINE Link].
- Soussain C, Patte C, Ostronoff M, et al. Small noncleaved cell lymphoma and leukemia in adults. A retrospective study of 65 adults treated with the LMB pediatric protocols. Blood. 1995 Feb 1. 85(3):664-74. [QxMD MEDLINE Link].
- Tholouli E, Watt S, Lucas GS, et al. Stage IV adult sporadic Burkitt lymphoma/leukemia with complex bone marrow cytogenetics is associated with a very poor outcome. Blood. 2009 Jul 9. 114(2):485-6; author reply 486-7. [QxMD MEDLINE Link].
- Thomas DA, Cortes J, O'Brien S, et al. Hyper-CVAD program in Burkitt's-type adult acute lymphoblastic leukemia. J Clin Oncol. 1999 Aug. 17(8):2461-70. [QxMD MEDLINE Link].
- Castillo JJ, Winer ES, Olszewski AJ. Population-based prognostic factors for survival in patients with Burkitt lymphoma: an analysis from the Surveillance, Epidemiology, and End Results database. Cancer. 2013 Oct 15. 119 (20):3672-9. [QxMD MEDLINE Link]. [Full Text].
- Armitage JO, Weisenburger DD. New approach to classifying non-Hodgkin's lymphomas: clinical features of the major histologic subtypes. Non-Hodgkin's Lymphoma Classification Project. J Clin Oncol. 1998 Aug. 16(8):2780-95. [QxMD MEDLINE Link].
- Derinkuyu BE, Boyunağa Ö, Öztunalı Ç, Tekkeşin F, Damar Ç, Alımlı AG, et al. Imaging features of Burkitt lymphoma in pediatric patients. Diagn Interv Radiol. 2016 Jan-Feb. 22 (1):95-100. [QxMD MEDLINE Link]. [Full Text].
- Lee AC, Li CH. Burkitt Lymphoma Presenting as Acute Pancreatitis: Report of 3 Cases and Review of the Literature. J Pediatr Hematol Oncol. 2019 Oct 29. 21(5):515-20. [QxMD MEDLINE Link].
- Legault S, Couture C, Bourgault C, Bergeron S, Poirier P, Sénéchal M. Primary cardiac Burkitt-like lymphoma of the right atrium. Can J Cardiol. 2009 Mar. 25(3):163-5. [QxMD MEDLINE Link]. [Full Text].
- Gutierrez-Garcia L, Medina Ramos N, Garcia Rodriguez R, Barber MA, Arias MD, Garcia JA. Bilateral ovarian Burkitt's lymphoma. Eur J Gynaecol Oncol. 2009. 30(2):231-3. [QxMD MEDLINE Link].
- Okudaira T, Nagasaki A, Miyagi T, Taira T, Ohshima K, Takasu N. Intensive chemotherapy for a patient with primary cutaneous diffuse large B-cell lymphoma with Burkitt-like morphology. Intern Med. 2009. 48(6):475-8. [QxMD MEDLINE Link].
- Braziel RM, Arber DA, Slovak ML, et al. The Burkitt-like lymphomas: a Southwest Oncology Group study delineating phenotypic, genotypic, and clinical features. Blood. 2001 Jun 15. 97(12):3713-20. [QxMD MEDLINE Link].
- Kluin PM, Harris NL, Stein H, Leoncini L. B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and Burkitt lymphoma. Swerdlow SH, Campo E, Harris NL, et al, eds. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th ed. Lyon, France: IARC Press; 2008. 265-7.
- Dogan A, Bagdi E, Munson P, Isaacson PG. CD10 and BCL-6 expression in paraffin sections of normal lymphoid tissue and B-cell lymphomas. Am J Surg Pathol. 2000 Jun. 24(6):846-52. [QxMD MEDLINE Link].
- McClure RF, Remstein ED, Macon WR, Dewald GW, Habermann TM, Hoering A. Adult B-cell lymphomas with burkitt-like morphology are phenotypically and genotypically heterogeneous with aggressive clinical behavior. Am J Surg Pathol. 2005 Dec. 29(12):1652-60. [QxMD MEDLINE Link].
- Dave SS, Fu K, Wright GW, Lam LT, et al, for the Lymphoma/Leukemia Molecular Profiling Project. Molecular diagnosis of Burkitt's lymphoma. N Engl J Med. 2006 Jun 8. 354(23):2431-42. [QxMD MEDLINE Link].
- Hummel M, Bentink S, Berger H, et al, for the Molecular Mechanisms in Malignant Lymphomas Network Project of the Deutsche Krebshilfe. A biologic definition of Burkitt's lymphoma from transcriptional and genomic profiling. N Engl J Med. 2006 Jun 8. 354(23):2419-30. [QxMD MEDLINE Link].
- Burmeister T, Schwartz S, Horst HA, Rieder H, Gokbuget N, Hoelzer D, et al. Molecular heterogeneity of sporadic adult Burkitt-type leukemia/lymphoma as revealed by PCR and cytogenetics: correlation with morphology, immunology and clinical features. Leukemia. 2005 Aug. 19(8):1391-8. [QxMD MEDLINE Link].
- Küppers R, Klein U, Hansmann ML, Rajewsky K. Cellular origin of human B-cell lymphomas. N Engl J Med. 1999 Nov 11. 341(20):1520-9. [QxMD MEDLINE Link].
- Garcia CF, Weiss LM, Warnke RA. Small noncleaved cell lymphoma: an immunophenotypic study of 18 cases and comparison with large cell lymphoma. Hum Pathol. 1986 May. 17(5):454-61. [QxMD MEDLINE Link].
- Magrath IT, Janus C, Edwards BK, et al. An effective therapy for both undifferentiated (including Burkitt's) lymphomas and lymphoblastic lymphomas in children and young adults. Blood. 1984 May. 63(5):1102-11. [QxMD MEDLINE Link].
- Smeland S, Blystad AK, Kvaloy SO, et al. Treatment of Burkitt's/Burkitt-like lymphoma in adolescents and adults: a 20-year experience from the Norwegian Radium Hospital with the use of three successive regimens. Ann Oncol. 2004 Jul. 15(7):1072-8. [QxMD MEDLINE Link].
- Bishop PC, Rao VK, Wilson WH. Burkitt's lymphoma: molecular pathogenesis and treatment. Cancer Invest. 2000. 18(6):574-83. [QxMD MEDLINE Link].
- Todeschini G, Bonifacio M, Tecchio C, et al. Intensive short-term chemotherapy regimen induces high remission rate (over 90%) and event-free survival both in children and adult patients with advanced sporadic Burkitt lymphoma/leukemia. Am J Hematol. 2012 Jan. 87(1):22-5. [QxMD MEDLINE Link].
- Hill QA, Owen RG. CNS prophylaxis in lymphoma: who to target and what therapy to use. Blood Rev. 2006 Nov. 20(6):319-32. [QxMD MEDLINE Link].
- Mead GM, Barrans SL, Qian W, et al, for the UK National Cancer Research Institute Lymphoma Clinical Studies Group and the Australasian Leukaemia and Lymphoma Group. A prospective clinicopathologic study of dose-modified CODOX-M/IVAC in patients with sporadic Burkitt lymphoma defined using cytogenetic and immunophenotypic criteria (MRC/NCRI LY10 trial). Blood. 2008 Sep 15. 112(6):2248-60. [QxMD MEDLINE Link]. [Full Text].
- Lee EJ, Petroni GR, Schiffer CA, et al. Brief-duration high-intensity chemotherapy for patients with small noncleaved-cell lymphoma or FAB L3 acute lymphocytic leukemia: results of cancer and leukemia group B study 9251. J Clin Oncol. 2001 Oct 15. 19(20):4014-22. [QxMD MEDLINE Link].
- Rizzieri DA, Johnson JL, Niedzwiecki D, et al. Intensive chemotherapy with and without cranial radiation for Burkitt leukemia and lymphoma: final results of Cancer and Leukemia Group B Study 9251. Cancer. 2004 Apr 1. 100(7):1438-48. [QxMD MEDLINE Link].
- Oriol A, Ribera JM, Bergua J, et al. High-dose chemotherapy and immunotherapy in adult Burkitt lymphoma: comparison of results in human immunodeficiency virus-infected and noninfected patients. Cancer. 2008 Jul 1. 113(1):117-25. [QxMD MEDLINE Link].
- Dunleavy K, Pittaluga S, Janik J, et al. Novel treatment of Burkitt lymphoma with dose-adjusted EPOCH-rituximab: Preliminary results showing excellent outcome (abstract). Blood. 2006. 108:774A.
- Sweetenham JW, Pearce R, Taghipour G, Blaise D, Gisselbrecht C, Goldstone AH. Adult Burkitt's and Burkitt-like non-Hodgkin's lymphoma--outcome for patients treated with high-dose therapy and autologous stem-cell transplantation in first remission or at relapse... J Clin Oncol. 1996 Sep. 14(9):2465-72. [QxMD MEDLINE Link].
- Wu J, Cao Y, Zhang Q, Liu W, Zhou X, Ming X, et al. Chimeric Antigen Receptor-Modified T Cell Immunotherapy for Relapsed and Refractory Adult Burkitt Lymphoma. Front Immunol. 2022. 13:879983. [QxMD MEDLINE Link]. [Full Text].
- Song KW, Barnett MJ, Gascoyne RD, et al. Haematopoietic stem cell transplantation as primary therapy of sporadic adult Burkitt lymphoma. Br J Haematol. 2006 Jun. 133(6):634-7. [QxMD MEDLINE Link].
- Philip T, Biron P. High-dose chemotherapy and autologous bone marrow transplantation in diffuse intermediate- and high-grade non-Hodgkin lymphoma. Crit Rev Oncol Hematol. 2002 Feb. 41(2):213-23. [QxMD MEDLINE Link].
- Nademanee A, Molina A, O'Donnell MR, et al. Results of high-dose therapy and autologous bone marrow/stem cell transplantation during remission in poor-risk intermediate- and high-grade lymphoma: international index high and high-intermediate risk group. Blood. 1997 Nov 15. 90(10):3844-52. [QxMD MEDLINE Link].
- Philip T, Armitage JO, Spitzer G, et al. High-dose therapy and autologous bone marrow transplantation after failure of conventional chemotherapy in adults with intermediate-grade or high-grade non-Hodgkin's lymphoma. N Engl J Med. Jun 11 1987. 316(24):1493-8. [QxMD MEDLINE Link].
- Grigg AP, Seymour JF. Graft versus Burkitt's lymphoma effect after allogeneic marrow transplantation. Leuk Lymphoma. 2002 Apr. 43(4):889-92. [QxMD MEDLINE Link].
- Peniket AJ, Ruiz de Elvira MC, Taghipour G, et al, for the European Bone Marrow Transplantation (EBMT) Lymphoma Registry. An EBMT registry matched study of allogeneic stem cell transplants for lymphoma: allogeneic transplantation is associated with a lower relapse rate but a higher procedure-related mortality rate than autologous transplantation. Bone Marrow Transplant. 2003 Apr. 31(8):667-78. [QxMD MEDLINE Link].
- Weinthal JA, Goldman SC, Lenarsky C. Successful treatment of relapsed Burkitt's lymphoma using unrelated cord blood transplantation as consolidation therapy. Bone Marrow Transplant. 2000 Jun. 25(12):1311-3. [QxMD MEDLINE Link].
- National Cancer Institute sponsored study of classifications of non-Hodgkin's lymphomas: summary and description of a working formulation for clinical usage. The Non-Hodgkin's Lymphoma Pathologic Classification Project. Cancer. 1982 May 15. 49 (10):2112-35. [QxMD MEDLINE Link].
- Harris NL, Jaffe ES, Stein H, Banks PM, Chan JK, Cleary ML, et al. A revised European-American classification of lymphoid neoplasms: a proposal from the International Lymphoma Study Group. Blood. 1994 Sep 1. 84 (5):1361-92. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] NCCN Clinical Practice Guidelines in Oncology. B-Cell Lymphomas. National Comprehensive Cancer Network. Available at https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf. Version 4.2022 — June 9, 2022; Accessed: July 5, 2022.
Author
Coauthor(s)
Ronald A Sacher, MD, FRCPC, DTM&H Professor Emeritus of Internal Medicine and Hematology/Oncology, Emeritus Director, Hoxworth Blood Center, University of Cincinnati Academic Health Center
Ronald A Sacher, MD, FRCPC, DTM&H is a member of the following medical societies: American Association for the Advancement of Science, American Association of Blood Banks, American Clinical and Climatological Association, American Society for Clinical Pathology, American Society of Hematology, College of American Pathologists, International Society of Blood Transfusion, International Society on Thrombosis and Haemostasis, Royal College of Physicians and Surgeons of Canada
Disclosure: Nothing to disclose.
Chief Editor
Emmanuel C Besa, MD Professor Emeritus, Department of Medicine, Division of Hematologic Malignancies and Hematopoietic Stem Cell Transplantation, Kimmel Cancer Center, Jefferson Medical College of Thomas Jefferson University
Emmanuel C Besa, MD is a member of the following medical societies: American Association for Cancer Education, American Society of Clinical Oncology, American College of Clinical Pharmacology, American Federation for Medical Research, American Society of Hematology, New York Academy of Sciences
Disclosure: Nothing to disclose.
Acknowledgements
Patturajah Anbumani, MD, MBBS, MS, MCh Associate Medical Director, Best Medical Care; Former Associate Medical Director, Jeanes Hospital, Temple University Health System; Former Adjunct Clinical Assistant Professor, New York College of Osteopathic Medicine; Former Clinical Assistant Professor, Department of Medicine, State University of New York-Downstate
Patturajah Anbumani, MD, MBBS, MS, MCh is a member of the following medical societies: American College of Physicians, American Medical Association, and American Medical Women’s Association
Disclosure: Nothing to disclose.
Samer A Bleibel, MD Staff Physician, Department of Internal Medicine, Wayne State University School of Medicine, St John's Hospital and Medical Centers
Samer A Bleibel, MD is a member of the following medical societies: American College of Physicians
Disclosure: Nothing to disclose.
Asher A Chanan-Khan, MD Assistant Professor, Department of Medicine, Division of Lymphoma and Bone Marrow Transplantation, Roswell Park Cancer Institute, State University of New York at Buffalo
Asher A Chanan-Khan, MD is a member of the following medical societies: American College of Physicians, American Medical Association, and American Society of Hematology
Disclosure: Nothing to disclose.
Hanxian Huang, MD, PhD Staff Physician, Department of Internal Medicine, Leesburg Regional Medical Center, The Villages Regional Hospital
Hanxian Huang, MD, PhD is a member of the following medical societies: American College of Physicians-American Society of Internal Medicine
Disclosure: Nothing to disclose.
Anand B Karnad, MBBS Program Director, Fellowship Programs in Hematology-Oncology, Professor of Medicine, Division of Medical Oncology, Department of Medicine, University of Texas Health Sciences Center, San Antonio
Anand B Karnad, MBBS is a member of the following medical societies: Alpha Omega Alpha, American College of Physicians, American Osler Society, American Society of Hematology, Assocation of Subspecialty Professors, and Massachusetts Medical Society
Disclosure: Nothing to disclose.
Olga Kozyreva, MD Attending Physician, Division of Hematology-Oncology, St Elizabeth's Medical Center; Assistant Professor, Tufts University School of Medicine
Disclosure: Nothing to disclose.
Sarah K May, MD Consulting Staff, Department of Hematology-Oncology, Caritas Carney Hospital, Commonwealth Hematology-Oncology PC
Disclosure: Nothing to disclose.
from Memorial Sloan-Kettering - Philip Schulman, MD Chief, Medical Oncology, Department of Medicine, Memorial Sloan-Kettering Cancer Center; Clinical Professor, Department of Medicine, New York University School of Medicine
Philip Schulman, MD is a member of the following medical societies: American Association for Cancer Research, American College of Physicians, American Society of Hematology, and Medical Society of the State of New York
Disclosure: Nothing to disclose.
Karen Seiter, MD Professor, Department of Internal Medicine, Division of Oncology/Hematology, New York Medical College
Karen Seiter, MD is a member of the following medical societies: American Association for Cancer Research, American College of Physicians, and American Society of Hematology
Disclosure: Novartis Honoraria Speaking and teaching; Schering Honoraria Speaking and teaching; Cephalon Honoraria Speaking and teaching; Celgene Honoraria Speaking and teaching
Francisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical Center College of Pharmacy; Editor-in-Chief, Medscape Drug Reference
Disclosure: Medscape Salary Employment
Yubao Wang, MD, PhD Fellow, Division of Hematology/Medical Oncology, University of Texas Health Science Center, San Antonio
Yubao Wang, MD, PhD is a member of the following medical societies: American College of Physicians, American Society of Clinical Oncology, and American Society of Hematology
Disclosure: Nothing to disclose.