Pediatric Type 1 Diabetes Mellitus: Practice Essentials, Background, Pathophysiology (original) (raw)
Practice Essentials
Type 1 diabetes is a chronic illness characterized by the body’s inability to produce insulin due to the autoimmune destruction of the beta cells in the pancreas. Most pediatric patients with diabetes have type 1 and a lifetime dependence on exogenous insulin. [1] The image below depicts the effects of insulin deficiency.

The effects of insulin deficiency.
Signs and symptoms
Signs and symptoms of type 1 diabetes in children include the following:
- Hyperglycemia
- Glycosuria
- Polydipsia
- Unexplained weight loss
- Nonspecific malaise
- Symptoms of ketoacidosis
See Clinical Presentation for more detail.
Diagnosis
Blood glucose
Blood glucose tests using capillary blood samples, reagent sticks, and blood glucose meters are the usual methods for monitoring day-to-day diabetes control.
Diagnostic criteria by the American Diabetes Association (ADA) include the following [2] :
- A fasting plasma glucose (FPG) level ≥126 mg/dL (7.0 mmol/L), or
- A 2-hour plasma glucose level ≥200 mg/dL (11.1 mmol/L) during a 75-g oral glucose tolerance test (OGTT), or
- A random plasma glucose ≥200 mg/dL (11.1 mmol/L) in a patient with classic symptoms of hyperglycemia or hyperglycemic crisis
Glycated hemoglobin
Measurement of HbA1c levels is the best method for medium-term to long-term diabetic control monitoring. An international expert committee composed of appointed representatives of the American Diabetes Association, the European Association for the Study of Diabetes, and others recommended HbA1c assay for diagnosing diabetes mellitus. [3]
See Workup for more detail.
Management
Glycemic control
The ADA recommends using patient age as one consideration in the establishment of glycemic goals, with different targets for preprandial, bedtime/overnight, and hemoglobin A1c (HbA1c) levels in patients aged 0-6, 6-12, and 13-19 years. [4] Benefits of tight glycemic control include not only continued reductions in the rates of microvascular complications but also significant differences in cardiovascular events and overall mortality.
Insulin therapy
All children with type 1 diabetes mellitus require insulin therapy. Most require 2 or more injections of insulin daily, with doses adjusted on the basis of self-monitoring of blood glucose levels. Insulin replacement is accomplished by giving a basal insulin and a preprandial (premeal) insulin. The basal insulin is either long-acting (glargine or detemir) or intermediate-acting (NPH). The preprandial insulin is either rapid-acting (lispro, aspart, or glulisine) or short-acting (regular).
Diet and activity
The aim of dietary management is to balance the child's food intake with insulin dose and activity and to keep blood glucose concentrations as close as possible to reference ranges, avoiding extremes of hyperglycemia and hypoglycemia.
The following are among the most recent dietary consensus recommendations (although they should be viewed in the context of the patient’s culture) [5] :
- Carbohydrates - Should provide 50-55% of daily energy intake; no more than 10% of carbohydrates should be from sucrose or other refined carbohydrates
- Fat - Should provide 30-35% of daily energy intake
- Protein - Should provide 10-15% of daily energy intake
Exercise is also an important aspect of diabetes management. It has real benefits for a child with diabetes. Patients should be encouraged to exercise regularly.
See Treatment and Medication for more detail.
![]()
Background
Most pediatric patients with diabetes have type 1 diabetes mellitus (T1DM) and a lifetime dependence on exogenous insulin. Diabetes mellitus (DM) is a chronic metabolic disorder caused by an absolute or relative deficiency of insulin, an anabolic hormone. Insulin is produced by the beta cells of the islets of Langerhans located in the pancreas, and the absence, destruction, or other loss of these cells results in type 1 diabetes (insulin-dependent diabetes mellitus [IDDM]). A possible mechanism for the development of type 1 diabetes is shown in the image below. (See Etiology.)
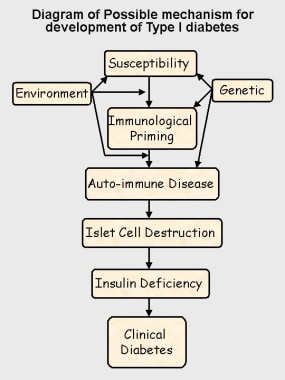
Possible mechanism for development of type 1 diabetes.
Type 2 diabetes mellitus (non–insulin-dependent diabetes mellitus [NIDDM]) is a heterogeneous disorder. Most patients with type 2 diabetes mellitus have insulin resistance, and their beta cells lack the ability to overcome this resistance. [6] Although this form of diabetes was previously uncommon in children, in some countries, 20% or more of new patients with diabetes in childhood and adolescence have type 2 diabetes mellitus, a change associated with increased rates of obesity. Other patients may have inherited disorders of insulin release, leading to maturity onset diabetes of the young (MODY) or congenital diabetes. [7, 8, 9] This topic addresses only type 1 diabetes mellitus. (See Etiology and Epidemiology.)
Hypoglycemia
Hypoglycemia is probably the most disliked and feared complication of diabetes, from the point of view of the child and the family. Children hate the symptoms of a hypoglycemic episode and the loss of personal control it may cause. (See Pathophysiology and Clinical.) [10]
Manage mild hypoglycemia by giving rapidly absorbed oral carbohydrate or glucose; for a comatose patient, administer an intramuscular injection of the hormone glucagon, which stimulates the release of liver glycogen and releases glucose into the circulation. Where appropriate, an alternative therapy is intravenous glucose (preferably no more than a 10% glucose solution). All treatments for hypoglycemia provide recovery in approximately 10 minutes. (See Treatment.)
Occasionally, a child with hypoglycemic coma may not recover within 10 minutes, despite appropriate therapy. Under no circumstances should further treatment be given, especially intravenous glucose, until the blood glucose level is checked and still found to be subnormal. Overtreatment of hypoglycemia can lead to cerebral edema and death. If coma persists, seek other causes.
Hypoglycemia was a particular concern in children younger than 4 years because the condition was thought to lead to possible intellectual impairment later in life. Persistent hyperglycemia is now believed to be more damaging.
Hyperglycemia
In an otherwise healthy individual, blood glucose levels usually do not rise above 180 mg/dL (9 mmol/L). In a child with diabetes, blood sugar levels rise if insulin is insufficient for a given glucose load. The renal threshold for glucose reabsorption is exceeded when blood glucose levels exceed 180 mg/dL (10 mmol/L), causing glycosuria with the typical symptoms of polyuria and polydipsia. (See Pathophysiology, Clinical, and Treatment.)
All children with diabetes experience episodes of hyperglycemia, but persistent hyperglycemia in very young children (age < 4 y) may lead to later intellectual impairment. [11, 12]
Diabetic ketoacidosis
Diabetic ketoacidosis (DKA) is much less common than hypoglycemia but is potentially far more serious, creating a life-threatening medical emergency. [13] Ketosis usually does not occur when insulin is present. In the absence of insulin, however, severe hyperglycemia, dehydration, and ketone production contribute to the development of DKA. The most serious complication of DKA is the development of cerebral edema, which increases the risk of death and long-term morbidity. Very young children at the time of first diagnosis are most likely to develop cerebral edema.
DKA usually follows increasing hyperglycemia and symptoms of osmotic diuresis. Users of insulin pumps, by virtue of absent reservoirs of subcutaneous insulin, may present with ketosis and more normal blood glucose levels. They are more likely to present with nausea, vomiting, and abdominal pain, symptoms similar to food poisoning. DKA may manifest as respiratory distress.
Injection-site hypertrophy
If children persistently inject their insulin into the same area, subcutaneous tissue swelling may develop, causing unsightly lumps and adversely affecting insulin absorption. Rotating the injection sites resolves the condition.
Fat atrophy can also occur, possibly in association with insulin antibodies. This condition is much less common but is more disfiguring.
Diabetic retinopathy
The most common cause of acquired blindness in many developed nations, diabetic retinopathy is rare in the prepubertal child or within 5 years of onset of diabetes. The prevalence and severity of retinopathy increase with age and are greatest in patients whose diabetic control is poor. [14] Prevalence rates seem to be declining, yet an estimated 80% of people with type 1 diabetes mellitus develop retinopathy. [15]
Diabetic nephropathy and hypertension
The exact mechanism of diabetic nephropathy is unknown. Peak incidence is in postadolescents, 10-15 years after diagnosis, and it may occur in as many as 30% of people with type 1 diabetes mellitus. [16]
In a patient with nephropathy, the albumin excretion rate (AER) increases until frank proteinuria develops, and this may progress to renal failure. Blood pressure rises with increased AER, and hypertension accelerates the progression to renal failure. Having diabetic nephropathy also increases the risk of significant diabetic retinopathy.
Progression may be delayed or halted by improved diabetes control, administration of angiotensin-converting enzyme inhibitors (ACE inhibitors), and aggressive blood pressure control. Regular urine screening for microalbuminuria provides opportunities for early identification and treatment to prevent renal failure.
A child younger than 15 years with persistent proteinuria may have a nondiabetic cause and should be referred to a pediatric nephrologist for further assessment.
Peripheral and autonomic neuropathy
The peripheral and autonomic nerves are affected in type 1 diabetes mellitus. [17] Hyperglycemic effects on axons and microvascular changes in endoneural capillaries are amongst the proposed mechanisms. (In adults, peripheral neuropathy usually occurs as a distal sensory loss.)
Autonomic changes involving cardiovascular control (eg, heart rate, postural responses) have been described in as many as 40% of children with diabetes. Cardiovascular control changes become more likely with increasing duration and worsening control. [18] In a study by 253 patients with type 1 diabetes (mean age at baseline 14.4 y), Cho et al reported that the prevalence of cardiac autonomic dysfunction increases in association with higher body mass index and central adiposity. [19]
Gastroparesis is another complication, and it which may be caused by autonomic dysfunction. Gastric emptying is significantly delayed, leading to problems of bloating and unpredictable excursions of blood glucose levels.
Macrovascular disease
Although this complication is not seen in pediatric patients, it is a significant cause of morbidity and premature mortality in adults with diabetes. People with type 1 diabetes mellitus have twice the risk of fatal myocardial infarction (MI) and stroke that people unaffected with diabetes do; in women, the MI risk is 4 times greater. People with type 1 diabetes mellitus also have 4 times greater risk for atherosclerosis.
The combination of peripheral vascular disease and peripheral neuropathy can cause serious foot pathology. Smoking, hypertension, hyperlipidemia, and poor diabetic control greatly increase the risk of vascular disease. Smoking, in particular, may increase the risk of myocardial infarction by a factor of 10.
Autoimmune diseases
Hypothyroidism affects 2-5% of children with diabetes. [20] Hyperthyroidism affects 1% of children with diabetes; the condition is usually discovered at the time of diabetes diagnosis.
Although Addison disease is uncommon, affecting less than 1% of children with diabetes, it is a life-threatening condition that is easily missed. Addison disease may reduce the insulin requirement and increase the frequency of hypoglycemia. (These effects may also be the result of unrecognized hypothyroidism.)
Celiac disease, associated with an abnormal sensitivity to gluten in wheat products, is probably a form of autoimmune disease and may occur in as many as 5% of children with type 1 diabetes mellitus. [21]
Necrobiosis lipoidica is probably another form of autoimmune disease. This condition is usually, but not exclusively, found in patients with type 1 diabetes. Necrobiosis lipoidica affects 1-2% of children and may be more common in children with poor diabetic control.
Limited joint mobility
Limited joint mobility (primarily affecting the hands and feet) is believed to be associated with poor diabetic control. [22]
Originally described in approximately 30% of patients with type 1 diabetes mellitus, limited joint mobility occurs in 50% of patients older than age 10 years who have had diabetes for longer than 5 years. The condition restricts joint extension, making it difficult to press the hands flat against each other. The skin of patients with severe joint involvement has a thickened and waxy appearance.
Limited joint mobility is associated with increased risks for diabetic retinopathy and nephropathy. Improved diabetes control over the past several years appears to have reduced the frequency of these additional complications by a factor of approximately 4. Patients have also markedly fewer severe joint mobility limitations.
![]()
Pathophysiology
Insulin is essential to process carbohydrates, fat, and protein. Insulin reduces blood glucose levels by allowing glucose to enter muscle cells and by stimulating the conversion of glucose to glycogen (glycogenesis) as a carbohydrate store. Insulin also inhibits the release of stored glucose from liver glycogen (glycogenolysis) and slows the breakdown of fat to triglycerides, free fatty acids, and ketones. It also stimulates fat storage. Additionally, insulin inhibits the breakdown of protein and fat for glucose production (gluconeogenesis) in the liver and kidneys.
Hyperglycemia
Hyperglycemia (ie, random blood glucose concentration of more than 200 mg/dL or 11 mmol/L) results when insulin deficiency leads to uninhibited gluconeogenesis and prevents the use and storage of circulating glucose. The kidneys cannot reabsorb the excess glucose load, causing glycosuria, osmotic diuresis, thirst, and dehydration. Increased fat and protein breakdown leads to ketone production and weight loss. Without insulin, a child with type 1 diabetes mellitus wastes away and eventually dies due to DKA. The effects of insulin deficiency are shown in the image below.
The effects of insulin deficiency.
Hypoglycemia
Insulin inhibits glucogenesis and glycogenolysis, while stimulating glucose uptake. In nondiabetic individuals, insulin production by the pancreatic islet cells is suppressed when blood glucose levels fall below 83 mg/dL (4.6 mmol/L). If insulin is injected into a treated child with diabetes who has not eaten adequate amounts of carbohydrates, blood glucose levels progressively fall.
The brain depends on glucose as a fuel. As glucose levels drop below 65 mg/dL (3.2 mmol/L) counterregulatory hormones (eg, glucagon, cortisol, epinephrine) are released, and symptoms of hypoglycemia develop. These symptoms include sweatiness, shaking, confusion, behavioral changes, and, eventually, coma when blood glucose levels fall below 30-40 mg/dL.
The glucose level at which symptoms develop varies greatly from individual to individual (and from time to time in the same individual), depending in part on the duration of diabetes, the frequency of hypoglycemic episodes, the rate of fall of glycemia, and overall control. (Glucose is also the sole energy source for erythrocytes and the kidney medulla.)
A study by Chan et al indicated that in pediatric patients with type 1 diabetes, the presence of hypoglycemia is a sign of decreased insulin sensitivity, while hyperglycemia in these patients, especially overnight, signals improved sensitivity to insulin. In contrast, the investigators found evidence that in pediatric patients with type 2 diabetes, markers of metabolic syndrome and hyperglycemia are associated with reduced insulin sensitivity. Patients in the study were between ages 12 and 19 years. [23]
![]()
Etiology
Most cases (95%) of type 1 diabetes mellitus are the result of environmental factors interacting with a genetically susceptible person. This interaction leads to the development of autoimmune disease directed at the insulin-producing cells of the pancreatic islets of Langerhans. These cells are progressively destroyed, with insulin deficiency usually developing after the destruction of 90% of islet cells.
Genetic issues
Clear evidence suggests a genetic component in type 1 diabetes mellitus. Monozygotic twins have a 60% lifetime concordance for developing type 1 diabetes mellitus, although only 30% do so within 10 years after the first twin is diagnosed. In contrast, dizygotic twins have only an 8% risk of concordance, which is similar to the risk among other siblings.
The frequency of diabetes development in children with a mother who has diabetes is 2-3%; this figure increases to 5-6% for children with a father who has type 1 diabetes mellitus. The risk to children rises to almost 30% if both parents are diabetic.
Human leukocyte antigen (HLA) class II molecules DR3 and DR4 are associated strongly with type 1 diabetes mellitus. More than 90% of whites with type 1 diabetes mellitus express 1 or both of these molecules, compared with 50-60% of the general population.
Patients expressing DR3 are also at risk for developing other autoimmune endocrinopathies and celiac disease. These patients are more likely to develop diabetes at a later age, to have positive islet cell antibodies, and to appear to have a longer period of residual islet cell function.
Patients expressing DR4 are usually younger at diagnosis and more likely to have positive insulin antibodies, yet they are unlikely to have other autoimmune endocrinopathies. The expression of both DR3 and DR4 carries the greatest risk of type 1 diabetes mellitus; these patients have characteristics of both the DR3 and DR4 groups.
Neonatal diabetes, including diagnosis in infants younger than age 6 months, is most likely due to an inherited defect of the iKir6.2 subunit potassium channel of the islet beta cells, and genetic screening is indicated. [24] This is particularly important, because these children respond well to sulphonylurea therapy.
Environmental factors
Environmental factors are important, because even identical twins have only a 30-60% concordance for type 1 diabetes mellitus and because incidence rates vary in genetically similar populations under different living conditions. [25] No single factor has been identified, but infections and diet are considered the 2 most likely environmental candidates.
Viral infections may be the most important environmental factor in the development of type 1 diabetes mellitus, [26] probably by initiating or modifying an autoimmune process. Instances have been reported of a direct toxic effect of infection in congenital rubella. One survey suggests enteroviral infection during pregnancy carries an increased risk of type 1 diabetes mellitus in the offspring. Paradoxically, type 1 diabetes mellitus incidence is higher in areas where the overall burden of infectious disease is lower.
A study from the US Centers for Disease Control and Prevention (CDC) indicates that infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes coronavirus disease 2019 (COVID-19), increases the likelihood of diabetes developing in children under age 18 years, more than 30 days post infection. The investigators, using two US health claims databases, reported that pediatric patients with COVID-19 in the HealthVerity database were 31% percent more likely than other youth to receive a new diabetes diagnosis, while those in the IQVIA database were 166% more likely. The study could not specify the type or types of diabetes specifically related to COVID-19, with the report saying that the disease could be causing both type 1 and type 2 diabetes but through differing mechanisms. The researchers suggested, however, that COVID-19 may induce diabetes by directly attacking pancreatic cells that express ACE2 receptors, that it may give rise to diabetes “through stress hyperglycemia resulting from the cytokine storm and alterations in glucose metabolism caused by infection,” or that COVID-19 may cause diabetes via the conversion of prediabetes to diabetes. Whether the diabetes is transient or chronic was also unknown. [27, 28]
A study by Kendall et al found that compared with pediatric subjects with a non–SARS-CoV-2 respiratory infection, the proportion of children who were diagnosed with new-onset type 1 diabetes mellitus within 6 months after a SARS-CoV-2 infection was 72% greater. According to the investigators, who looked at patients aged 18 years or younger, the rate of new-onset type 1 diabetes mellitus among the two groups was 0.025% and 0.043%, respectively, at 6 months. [29]
However, a study by Cromer et al looked at adult patients with newly diagnosed diabetes mellitus at the time of hospital admission for COVID-19, finding that a number of them subsequently regressed to a state of normoglycemia or prediabetes. The investigators reported that out of 64 survivors in the study with newly diagnosed diabetes (62 of whom had type 2 diabetes), 26 (40.6%) were known to undergo such regression (median 323-day follow-up). [30]
Dietary factors are also relevant. Breastfed infants have a lower risk for type 1 diabetes, and a direct relationship is observed between per capita cow's milk consumption and the incidence of diabetes. Some cow's milk proteins (eg, bovine serum albumin) have antigenic similarities to an islet cell antigen.
Nitrosamines, chemicals found in smoked foods and some water supplies, are known to cause type 1 diabetes mellitus in animal models; however, no definite link has been made with humans.
The known association of increasing incidence of type 1 diabetes mellitus with distance from the equator may now have an explanation. Reduced exposure to ultraviolet (UV) light and lower vitamin D levels, both of which are more likely found in the higher latitudes, are associated with an increased risk of type 1 diabetes mellitus. [31]
Chemical causes
Streptozotocin and RH-787, a rat poison, selectively damages islet cells and can cause type 1 diabetes mellitus.
Other causes
Additional factors in the development of type 1 diabetes mellitus include the following:
- Congenital absence of the pancreas or islet cells
- Pancreatectomy
- Wolfram syndrome (diabetes insipidus, diabetes mellitus, optic atrophy, deafness [DIDMOAD])
![]()
Epidemiology
Occurrence in the United States
The overall annual incidence of diabetes mellitus is about 24.3 cases per 100,000 person-years. Although most new diabetes cases are type 1 (approximately 15,000 annually), increasing numbers of older children are being diagnosed with type 2 diabetes mellitus, especially among minority groups (3700 annually). [32]
A study by Mayer-Davis et al indicated that between 2002 and 2012, the incidence of type 1 and type 2 diabetes mellitus saw a significant rise among youths in the United States. According to the report, after the figures were adjusted for age, sex, and race or ethnic group, the incidence of type 1 (in patients aged 0-19 years) and type 2 diabetes mellitus (in patients aged 10-19 years) during this period underwent a relative annual increase of 1.8% and 4.8%, respectively. The greatest increases occurred among minority youths. [33]
International occurrence
Type 1 diabetes mellitus has wide geographic variation in incidence and prevalence. [34] Annual incidence varies from 0.61 cases per 100,000 population in China to 41.4 cases per 100,000 population in Finland. Substantial variations are observed between nearby countries with differing lifestyles, such as Estonia and Finland, and between genetically similar populations, such as those in Iceland and Norway.
Also striking are the differences in incidence between mainland Italy (8.4 cases per 100,000 population) and the Island of Sardinia (36.9 cases per 100,000 population). These variations strongly support the importance of environmental factors in the development of type 1 diabetes mellitus. Most countries report that incidence rates have at least doubled in the last 20 years. Incidence appears to increase with distance from the equator. [35]
Race-related demographics
Different environmental effects on type 1 diabetes mellitus development complicate the influence of race, but racial differences are evident. Whites have the highest reported incidence, whereas Chinese individuals have the lowest. Type 1 diabetes mellitus is 1.5 times more likely to develop in American whites than in American blacks or Hispanics. Current evidence suggests that when immigrants from an area with low incidence move to an area with higher incidence, their rates of type 1 diabetes mellitus tend to increase toward the higher level.
Sex-related demographics
The influence of sex varies with the overall incidence rates. Males are at greater risk in regions of high incidence, particularly older males, whose incidence rates often show seasonal variation. Females appear to be at a greater risk in low-incidence regions.
Age-related demographics
Type 1 diabetes mellitus can occur at any age, but incidence rates generally increase with age until midpuberty and then decline. [36] Onset in the first year of life, although unusual, can occur, so type 1 diabetes mellitus must be considered in any infant or toddler, because these children have the greatest risk for mortality if diagnosis is delayed. (Because diabetes is easily missed in an infant or preschool-aged child, if in doubt, check the urine for glucose.) Symptoms in infants and toddlers may include the following:
- Severe monilial diaper/napkin rash
- Unexplained malaise
- Poor weight gain or weight loss
- Increased thirst
- Vomiting and dehydration, with a constantly wet napkin/diaper
In areas with high prevalence rates, a bimodal variation of incidence has been reported that shows a definite peak in early childhood (ie, ages 4-6 y) and a second, much greater peak of incidence during early puberty (ie, ages 10-14 y). [37]
![]()
Prognosis
Apart from severe DKA or hypoglycemia, type 1 diabetes mellitus has little immediate morbidity. The risk of complications relates to diabetic control. With good management, patients can expect to lead full, normal, and healthy lives. Nevertheless, the average life expectancy of a child diagnosed with type 1 diabetes mellitus has been variously suggested to be reduced by 13-19 years, compared with their nondiabetic peers. [38]
Morbidity and mortality
Information on mortality rates for type 1 diabetes mellitus is difficult to ascertain without complete national registers of childhood diabetes, although age-specific mortality is probably double that of the general population. [39, 40] Children aged 1-4 years are particularly at risk and may die due to DKA at the time of diagnosis. Adolescents are also a high-risk group. Most deaths result from delayed diagnosis or neglected treatment and subsequent cerebral edema during treatment for DKA, although untreated hypoglycemia also causes some deaths. Unexplained death during sleep may also occur and appears more likely to affect young males. [41]
A population-based, nationwide cohort study in Finland examined the short -and long-term time trends in mortality among patients with early-onset and late-onset type 1 diabetes. The results suggest that in those with early-onset type 1 diabetes (age 0-14 y), survival has improved over time. Survival of those with late-onset type 1 diabetes (15-29 y) has deteriorated since the 1980s, and the ratio of deaths caused by acute complications has increased in this group. Overall, alcohol was noted as an important cause of death in patients with type 1 diabetes; women had higher standardized mortality ratios than did men in both groups. [42]
The complications of type 1 diabetes mellitus can be divided into 3 major categories: acute complications, long-term complications, and complications caused by associated autoimmune diseases.
Acute complications, which include hypoglycemia, hyperglycemia, and DKA, reflect the difficulties of maintaining a balance between insulin therapy, dietary intake, and exercise.
Long-term complications arise from the damaging effects of prolonged hyperglycemia and other metabolic consequences of insulin deficiency on various tissues. Although long-term complications are rare in childhood, maintaining good control of diabetes is important to prevent complications from developing in later life. [43] The likelihood of developing complications appears to depend on the interaction of factors such as metabolic control, genetic susceptibility, lifestyle (eg, smoking, diet, exercise), pubertal status, and gender. [44, 45] Long-term complications include the following:
- Retinopathy
- Cataracts
- Gastroparesis
- Progressive renal failure
- Early coronary artery disease
- Peripheral vascular disease
- Peripheral and autonomic neuropathy
- Increased risk of infection
Associated autoimmune diseases are common in type 1 diabetes mellitus, particularly in children who have HLA-DR3. Some conditions may precede the development of diabetes, and others may develop later. As many as 20% of children with diabetes have thyroid autoantibodies. [46]
Type 1 diabetes in pediatric patients has been linked to changes in cognition and brain structure, with a study by Siller et al finding lower volume in the left temporal-parietal-occipital cortex in young patients with type 1 diabetes than in controls. The study also indicated that in pediatric patients, higher severity of type 1 diabetes presentation correlates with greater structural differences in the brain at about 3 months following diagnosis. The investigators found that among study patients with type 1 diabetes, an association existed between the presence of diabetic ketoacidosis at presentation and reduced radial, axial, and mean diffusivity in the major white matter tracts on magnetic resonance imaging (MRI). In those with higher glycated hemoglobin (HbA1c) levels, hippocampal, thalamic, and cerebellar white matter volumes were lower, as was right posterior parietal cortical thickness, while right occipital cortical thickness was greater. Patients in the study were aged 7-17 years. [47]
A study by Dabelea et al found that in teenagers and young adults in whom diabetes mellitus had been diagnosed during childhood or adolescence, diabetes-related complications and comorbidities—including diabetic kidney disease, retinopathy, and peripheral neuropathy (but not arterial stiffness or hypertension)—were more prevalent in those with type 2 diabetes than in those with type 1 disease. [48]
COVID-19
A study indicated that children with type 1 diabetes mellitus who have an HbA1c level of 9% or above are at greater risk of mortality, intubation, and sepsis due to coronavirus disease 2019 (COVID-19) than are children without type 1 diabetes. However, the report also found evidence that such risk is not greater in children with an HbA1c level at or below 7%. The investigators found the COVID-19 mortality rates in children without type 1 diabetes, those with type 1 diabetes, and those with type 1 diabetes with an HbA1c of 7% or lower to be 0.047%, 0.328%, and 0%, respectively. [49]
![]()
Patient Education
Education is a continuing process involving the child, family, and all members of the diabetes team. [50, 51] (See the videos below.) The following strategies may be used:
- Formal education sessions in a clinic setting
- Opportunistic teaching at clinics or at home in response to crises or difficulties such as acute illness
- Therapeutic camping or other organized events
- Patient-organized meetings
Taking Diabetes Back to School.
Carbs for Kids-Count Them In: The Constant Carbohydrates Diet.
Diabetes-related organizations and patient resources include the following: [52]
![]()
- Katsarou A, Gudbjornsdottir S, Rawshani A, et al. Type 1 diabetes mellitus. Nat Rev Dis Primers. 2017 Mar 30. 3:17016. [QxMD MEDLINE Link]. [Full Text].
- Diagnosis and classification of diabetes mellitus. Diabetes Care. 2010 Jan. 33 Suppl 1:S62-9. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] International Expert Committee Report on the Role of the A1C Assay in the Diagnosis of Diabetes. Diabetes Care. 2009 Jun 5. [QxMD MEDLINE Link]. [Full Text].
- Standards of medical care in diabetes--2011. Diabetes Care. 2011 Jan. 34 Suppl 1:S11-61. [QxMD MEDLINE Link]. [Full Text].
- Pihoker C, Forsander G, Wolfsdorf J, Klingensmith GJ. The delivery of ambulatory diabetes care to children and adolescents with diabetes. Pediatr Diabetes. 2009 Sep. 10 Suppl 12:58-70. [QxMD MEDLINE Link].
- Rosenbloom AL, Silverstein JH, Amemiya S, Zeitler P, Klingensmith GJ. Type 2 diabetes in children and adolescents. Pediatr Diabetes. 2009 Sep. 10 Suppl 12:17-32. [QxMD MEDLINE Link].
- Porter JR, Barrett TG. Acquired non-type 1 diabetes in childhood: subtypes, diagnosis, and management. Arch Dis Child. 2004 Dec. 89(12):1138-44. [QxMD MEDLINE Link]. [Full Text].
- Barrett TG. Differential diagnosis of type 1 diabetes: which genetic syndromes need to be considered?. Pediatr Diabetes. 2007 Oct. 8 Suppl 6:15-23. [QxMD MEDLINE Link].
- Hattersley A, Bruining J, Shield J, Njolstad P, Donaghue KC. The diagnosis and management of monogenic diabetes in children and adolescents. Pediatr Diabetes. 2009 Sep. 10 Suppl 12:33-42. [QxMD MEDLINE Link].
- Clarke W, Jones T, Rewers A, Dunger D, Klingensmith GJ. Assessment and management of hypoglycemia in children and adolescents with diabetes. Pediatr Diabetes. 2009 Sep. 10 Suppl 12:134-45. [QxMD MEDLINE Link].
- Hershey T, Perantie DC, Warren SL, et al. Frequency and timing of severe hypoglycemia affects spatial memory in children with type 1 diabetes. Diabetes Care. 2005 Oct. 28(10):2372-7. [QxMD MEDLINE Link]. [Full Text].
- Patiño-Fernández AM, Delamater AM, Applegate EB, et al. Neurocognitive functioning in preschool-age children with type 1 diabetes mellitus. Pediatr Diabetes. 2010 Sep. 11(6):424-30. [QxMD MEDLINE Link]. [Full Text].
- Nakhla M, Rahme E, Simard M, Larocque I, Legault L, Li P. Risk of ketoacidosis in children at the time of diabetes mellitus diagnosis by primary caregiver status: a population-based retrospective cohort study. CMAJ. 2018 Apr 9. 190 (14):E416-21. [QxMD MEDLINE Link]. [Full Text].
- Andreasson R, Ekelund C, Landin-Olsson M, Nilsson C. HbA1c levels in children with type 1 diabetes and correlation to diabetic retinopathy. J Pediatr Endocrinol Metab. 2018 Mar 28. 31 (4):369-74. [QxMD MEDLINE Link].
- d'Annunzio G, Malvezzi F, Vitali L, Barone C, Giacchero R, Klersy C, et al. A 3-19-year follow-up study on diabetic retinopathy in patients diagnosed in childhood and treated with conventional therapy. Diabet Med. 1997 Nov. 14(11):951-8. [QxMD MEDLINE Link].
- Jones CA, Leese GP, Kerr S, et al. Development and progression of microalbuminuria in a clinic sample of patients with insulin dependent diabetes mellitus. Arch Dis Child. 1998 Jun. 78(6):518-23. [QxMD MEDLINE Link]. [Full Text].
- Walter-Holiner I, Barbarini DS, Lutschg J, et al. High Prevalence and Incidence of Diabetic Peripheral Neuropathy in Children and Adolescents With Type 1 Diabetes Mellitus: Results From a Five-Year Prospective Cohort Study. Pediatr Neurol. 2018 Mar. 80:51-60. [QxMD MEDLINE Link].
- Barkai L, Madacsy L. Cardiovascular autonomic dysfunction in diabetes mellitus. Arch Dis Child. 1995 Dec. 73(6):515-8. [QxMD MEDLINE Link].
- Cho YH, Craig ME, Jopling T, Chan A, Donaghue KC. Higher body mass index predicts cardiac autonomic dysfunction: a longitudinal study in adolescent type 1 diabetes. Pediatr Diabetes. 2018 Jan 31. [QxMD MEDLINE Link].
- Mohn A, Di Michele S, Di Luzio R, et al. The effect of subclinical hypothyroidism on metabolic control in children andadolescents with Type 1 diabetes mellitus. Diabet Med. 2002 Jan. 19(1):70-3. [QxMD MEDLINE Link].
- Barera G, Bonfanti R, Viscardi M, et al. Occurrence of celiac disease after onset of type 1 diabetes: a 6-year prospectivelongitudinal study. Pediatrics. 2002 May. 109(5):833-8. [QxMD MEDLINE Link]. [Full Text].
- Infante JR, Rosenbloom AL, Silverstein JH, et al. Changes in frequency and severity of limited joint mobility in children withtype 1 diabetes mellitus between 1976-78 and 1998. J Pediatr. 2001 Jan. 138(1):33-7. [QxMD MEDLINE Link].
- Chan CL, Pyle L, Morehead R, Baumgartner A, Cree-Green M, Nadeau KJ. The role of glycemia in insulin resistance in youth with type 1 and type 2 diabetes. Pediatr Diabetes. 2016 Aug 9. [QxMD MEDLINE Link].
- Gloyn AL, Pearson ER, Antcliff JF, Proks P, Bruining GJ, Slingerland AS. Activating mutations in the gene encoding the ATP-sensitive potassium-channel subunit Kir6.2 and permanent neonatal diabetes. N Engl J Med. 2004 Apr 29. 350(18):1838-49. [QxMD MEDLINE Link].
- Patterson CC, Carson DJ, Hadden DR. Epidemiology of childhood IDDM in Northern Ireland 1989-1994: low incidence in areas with highest population density and most household crowding. Northern Ireland Diabetes Study Group. Diabetologia. 1996 Sep. 39(9):1063-9. [QxMD MEDLINE Link].
- Hyoty H, Hiltunen M, Knip M, et al. A prospective study of the role of coxsackie B and other enterovirus infections in the pathogenesis of IDDM. Childhood Diabetes in Finland (DiMe) Study Group. Diabetes. 1995 Jun. 44(6):652-7. [QxMD MEDLINE Link].
- Barrett CE, Koyama AK, Alvarez P, et al. Risk for Newly Diagnosed Diabetes >30 Days After SARS-CoV-2 Infection Among Persons Aged MMWR Morb Mortal Wkly Rep. 2022 Jan 7. 71:[Full Text].
- Tucker ME. COVID-19 Associated With Increased Diabetes Risk in Youth. Medscape Medical News. 2022 Jan 10. [Full Text].
- Kendall EK, Olaker VR, Kaelber DC, Xu R, Davis PB. Association of SARS-CoV-2 Infection With New-Onset Type 1 Diabetes Among Pediatric Patients From 2020 to 2021. JAMA Netw Open. 2022 Sep 1. 5 (9):e2233014. [QxMD MEDLINE Link]. [Full Text].
- Cromer SJ, Colling C, Schatoff D, et al. Newly diagnosed diabetes vs. pre-existing diabetes upon admission for COVID-19: Associated factors, short-term outcomes, and long-term glycemic phenotypes. J Diabetes Complications. 2022 Feb 4. 108145. [QxMD MEDLINE Link]. [Full Text].
- Mohr SB, Garland CF, Gorham ED, Garland FC. The association between ultraviolet B irradiance, vitamin D status and incidence rates of type 1 diabetes in 51 regions worldwide. Diabetologia. 2008 Aug. 51(8):1391-8. [QxMD MEDLINE Link].
- Dabelea D, Bell RA, D'Agostino RB Jr, Imperatore G, Johansen JM. Incidence of diabetes in youth in the United States. JAMA. 2007 Jun 27. 297(24):2716-24. [QxMD MEDLINE Link].
- Mayer-Davis EJ, Lawrence JM, Dabelea D, et al. Incidence Trends of Type 1 and Type 2 Diabetes among Youths, 2002-2012. N Engl J Med. 2017 Apr 13. 376 (15):1419-29. [QxMD MEDLINE Link].
- Silink M. Childhood diabetes: a global perspective. Horm Res. 2002. 57 Suppl 1:1-5. [QxMD MEDLINE Link].
- Soltesz G, Patterson CC, Dahlquist G. Worldwide childhood type 1 diabetes incidence--what can we learn from epidemiology?. Pediatr Diabetes. 2007 Oct. 8 Suppl 6:6-14. [QxMD MEDLINE Link].
- Craig ME, Hattersley A, Donaghue KC. Definition, epidemiology and classification of diabetes in children and adolescents. Pediatr Diabetes. 2009 Sep. 10 Suppl 12:3-12. [QxMD MEDLINE Link].
- Felner EI, Klitz W, Ham M, Lazaro AM, Stastny P, Dupont B. Genetic interaction among three genomic regions creates distinct contributions to early- and late-onset type 1 diabetes mellitus. Pediatr Diabetes. 2005 Dec. 6(4):213-20. [QxMD MEDLINE Link].
- DiLiberti JH, Lorenz RA. Long-term trends in childhood diabetes mortality: 1968-1998. Diabetes Care. 2001 Aug. 24(8):1348-52. [QxMD MEDLINE Link].
- Dahlquist G, Kallen B. Mortality in childhood-onset type 1 diabetes: a population-based study. Diabetes Care. 2005 Oct. 28(10):2384-7. [QxMD MEDLINE Link].
- Edge JA, Ford-Adams ME, Dunger DB. Causes of death in children with insulin dependent diabetes 1990-96. Arch Dis Child. 1999 Oct. 81(4):318-23. [QxMD MEDLINE Link]. [Full Text].
- Koltin D, Daneman D. Dead-in-bed syndrome - a diabetes nightmare. Pediatr Diabetes. 2008 Oct. 9(5):504-7. [QxMD MEDLINE Link].
- Harjutsalo V, Forsblom C, Groop PH. Time trends in mortality in patients with type 1 diabetes: nationwide population based cohort study. BMJ. 2011 Sep 8. 343:d5364. [QxMD MEDLINE Link]. [Full Text].
- DCCT Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Engl J Med. 1993 Sep 30. 329(14):977-86. [QxMD MEDLINE Link].
- Gallego PH, Wiltshire E, Donaghue KC. Identifying children at particular risk of long-term diabetes complications. Pediatr Diabetes. 2007 Oct. 8 Suppl 6:40-8. [QxMD MEDLINE Link].
- Donaghue KC, Chiarelli F, Trotta D, Allgrove J, Dahl-Jorgensen K. Microvascular and macrovascular complications associated with diabetes in children and adolescents. Pediatr Diabetes. 2009 Sep. 10 Suppl 12:195-203. [QxMD MEDLINE Link].
- Kordonouri O, Maguire AM, Knip M, et al. Other complications and associated conditions with diabetes in children and adolescents. Pediatr Diabetes. 2009 Sep. 10 Suppl 12:204-10. [QxMD MEDLINE Link].
- Siller AF, Lugar H, Rutlin J, et al. Severity of clinical presentation in youth with type 1 diabetes is associated with differences in brain structure. Pediatr Diabetes. 2016 Aug 2. [QxMD MEDLINE Link].
- Dabelea D, Stafford JM, Mayer-Davis EJ, et al. Association of Type 1 Diabetes vs Type 2 Diabetes Diagnosed During Childhood and Adolescence With Complications During Teenage Years and Young Adulthood. JAMA. 2017 Feb 28. 317 (8):825-35. [QxMD MEDLINE Link].
- Tucker ME. Type 1 Diabetes Raises COVID-19 Risk in Kids if A1c Is High. Medscape Medical News. 2021 Mar 22. [Full Text].
- Swift PG. Diabetes education in children and adolescents. Pediatr Diabetes. 2009 Sep. 10 Suppl 12:51-7. [QxMD MEDLINE Link].
- Brink S, Laffel L, Likitmaskul S, et al. Sick day management in children and adolescents with diabetes. Pediatr Diabetes. 2009 Sep. 10 Suppl 12:146-53. [QxMD MEDLINE Link].
- CDC. National Diabetes Fact Sheet. United States. Centers for Disease Control and Prevention. Available at https://www.cdc.gov/diabetes/pubs/pdf/ndfs_2003.pdf.
- [Guideline] Mosca A, Goodall I, Hoshino T, et al. Global standardization of glycated hemoglobin measurement: the position of the IFCC Working Group. Clin Chem Lab Med. 2007. 45(8):1077-80. [QxMD MEDLINE Link].
- Nansel TR, Iannotti RJ, Liu A. Clinic-integrated behavioral intervention for families of youth with type 1 diabetes: randomized clinical trial. Pediatrics. 2012 Apr. 129(4):e866-73. [QxMD MEDLINE Link]. [Full Text].
- Clar C, Waugh N, Thomas S. Routine hospital admission versus out-patient or home care in children at diagnosisof type 1 diabetes mellitus. Cochrane Database Syst Rev. 2003. CD004099. [QxMD MEDLINE Link].
- Uusitalo U, Liu X, Yang J, et al, for the TEDDY Study Group. Probiotic use in infancy and islet autoimmunity in The Environmental Determinants of Diabetes in the Young (TEDDY) study [abstract 170]. Presented at: European Association for the Study of Diabetes 2014 Meeting; Vienna, Austria; September 18, 2014. [Full Text].
- McCall B. Probiotics cut autoimmunity 33% in infants at risk for diabetes. Medscape Medical News. September 19, 2014. [Full Text].
- Smart C, Aslander-van Vliet E, Waldron S. Nutritional management in children and adolescents with diabetes. Pediatr Diabetes. 2009 Sep. 10 Suppl 12:100-17. [QxMD MEDLINE Link].
- Robertson K, Adolfsson P, Scheiner G, Hanas R, Riddell MC. Exercise in children and adolescents with diabetes. Pediatr Diabetes. 2009 Sep. 10 Suppl 12:154-68. [QxMD MEDLINE Link].
- Kaufman FR, Halvorson M, Carpenter S. Association between diabetes control and visits to a multidisciplinary pediatric diabetes clinic. Pediatrics. 1999 May. 103(5 Pt 1):948-51. [QxMD MEDLINE Link]. [Full Text].
- Silverstein J, Klingensmith G, Copeland K, et al. Care of children and adolescents with type 1 diabetes: a statement of the AmericanDiabetes Association. Diabetes Care. 2005 Jan. 28(1):186-212. [QxMD MEDLINE Link]. [Full Text].
- Pihoker C, Forsander G, Wolfsdorf J, Klingensmith GJ. The delivery of ambulatory diabetes care: structures, processes, and outcomes of ambulatory diabetes care. Pediatr Diabetes. 2008 Dec. 9(6):609-20. [QxMD MEDLINE Link].
- [Guideline] American Diabetes Association Professional Practice Committee. Summary of Revisions: Standards of Care in Diabetes-2024. Diabetes Care. 2024 Jan 1. 47 (Supplement_1):S5-S10. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] American Diabetes Association Professional Practice Committee. 14. Children and Adolescents: Standards of Care in Diabetes-2024. Diabetes Care. 2024 Jan 1. 47 (Suppl 1):S258-81. [QxMD MEDLINE Link]. [Full Text].
- Garg SK, Voelmle MK, Beatson CR, et al. Use of continuous glucose monitoring in subjects with type 1 diabetes on multiple daily injections versus continuous subcutaneous insulin infusion therapy: a prospective 6-month study. Diabetes Care. 2011 Mar. 34 (3):574-9. [QxMD MEDLINE Link]. [Full Text].
- Health Quality Ontario . Continuous Monitoring of Glucose for Type 1 Diabetes: A Health Technology Assessment. Ont Health Technol Assess Ser. 2018. 18 (2):1-160. [QxMD MEDLINE Link]. [Full Text].
- Battelino T, Phillip M, Bratina N, Nimri R, Oskarsson P, Bolinder J. Effect of continuous glucose monitoring on hypoglycemia in type 1 diabetes. Diabetes Care. 2011 Apr. 34 (4):795-800. [QxMD MEDLINE Link]. [Full Text].
- What is the pancreas? What is an artificial pancreas device system?. FDA. Available at https://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/HomeHealthandConsumer/ConsumerProducts/ArtificialPancreas/ucm259548.htm. Dec 17, 2017; Accessed: Jun 25, 2018.
- FDA approves first automated insulin delivery device for type 1 diabetes. FDA. Available at https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm522974.htm. Sep 28, 2016; Accessed: Jun 25, 2018.
- Busko M. FDA Approves Artificial Pancreas for Children With Type 1 Diabetes. Medscape Medical News. 2018 Jun 22. [Full Text].
- Schiaffini R, Lumaca A, Martino M, et al. Time In Tight Range in children and adolescents with type 1 diabetes: A cross-sectional observational single centre study evaluating efficacy of new advanced technologies. Diabetes Metab Res Rev. 2024 Jul. 40 (5):e3826. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] Tucker ME. ADA Issues New Guidance on Type 1 Diabetes in Youth. Medscape Medical News. 2018 Aug 10. [Full Text].
- [Guideline] Chiang JL, Maahs DM, Garvey KC, et al. Type 1 Diabetes in Children and Adolescents: A Position Statement by the American Diabetes Association. Diabetes Care. 2018 Sep. 41 (9):2026-44. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] American Diabetes Association. 12. Children and Adolescents: Standards of Medical Care in Diabetes-2018. Diabetes Care. 2018 Jan. 41 (Suppl 1):S126-36. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] Donaghue KC, Marcovecchio ML, Wadwa RP, et al. ISPAD Clinical Practice Consensus Guidelines 2018: microvascular and macrovascular complications in children and adolescents. Pediatr Diabetes. 2018 Oct. 19 Suppl 27:262-74. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] Bjornstad P, Dart A, Donaghue KC, et al. ISPAD Clinical Practice Consensus Guidelines 2022: Microvascular and macrovascular complications in children and adolescents with diabetes. Pediatr Diabetes. 2022 Dec. 23 (8):1432-50. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] DiMeglio LA, Acerini CL, Codner E, et al. ISPAD Clinical Practice Consensus Guidelines 2018: glycemic control targets and glucose monitoring for children, adolescents, and young adults with diabetes. Pediatr Diabetes. 2018 Oct. 19 Suppl 27:105-14. [QxMD MEDLINE Link]. [Full Text].
- Bangstad HJ, Danne T, Deeb L, Jarosz-Chobot P, Urakami T, Hanas R. Insulin treatment in children and adolescents with diabetes. Pediatr Diabetes. 2009 Sep. 10 Suppl 12:82-99. [QxMD MEDLINE Link].
- Danne T, Deiss D, Hopfenmuller W, et al. Experience with insulin analogues in children. Horm Res. 2002. 57 Suppl 1:46-53. [QxMD MEDLINE Link].
- Siebenhofer A, Plank J, Berghold A, et al. Short acting insulin analogues versus regular human insulin in patients withdiabetes mellitus. Cochrane Database Syst Rev. 2004. CD003287. [QxMD MEDLINE Link].
- Willi SM, Planton J, Egede L, Schwarz S. Benefits of continuous subcutaneous insulin infusion in children with type1 diabetes. J Pediatr. 2003 Dec. 143(6):796-801. [QxMD MEDLINE Link].
- Mortensen HB, Hougaard P. Comparison of metabolic control in a cross-sectional study of 2,873 children and adolescents with IDDM from 18 countries. The Hvidore Study Group on Childhood Diabetes [published erratum appears in Diabetes Care 1997 Jul;20(7):1216]. Diabetes Care. 1997 May. 20(5):714-20. [QxMD MEDLINE Link].
- Danne T, Mortensen HB, Hougaard P, et al. Persistent differences among centers over 3 years in glycemic control and hypoglycemiain a study of 3,805 children and adolescents with type 1 diabetes from the Hvidøre Study Group. Diabetes Care. 2001 Aug. 24(8):1342-7. [QxMD MEDLINE Link]. [Full Text].
- Herold KC, Bundy BN, Long SA, and the, Type 1 Diabetes TrialNet Study Group. An Anti-CD3 Antibody, Teplizumab, in Relatives at Risk for Type 1 Diabetes. N Engl J Med. 2019 Aug 15. 381 (7):603-13. [QxMD MEDLINE Link]. [Full Text].
- Sims EK, Bundy BN, Stier K, and the, Type 1 Diabetes TrialNet Study Group. Teplizumab improves and stabilizes beta cell function in antibody-positive high-risk individuals. Sci Transl Med. 2021 Mar 3. 13 (583):[QxMD MEDLINE Link]. [Full Text].