Using a business model approach and marketing techniques for recruitment to clinical trials (original) (raw)
Randomised controlled trials (RCTs) are widely accepted as the gold standard for evaluating health care interventions [1, 2]. Several factors contribute to the success of a RCT, including a research question that is relevant to those at whom the trial results are aimed [3, 4], a design that is both scientifically rigorous and which fits in with clinical practice [5], obtaining the appropriate legislative approvals [6], the active participation and commitment [[7](/article/10.1186/1745-6215-12-74#ref-CR7 "Sackett DL: Why randomized controlled trials fail but needn't: 1. Failure to gain "coal-face" commitment and to use the uncertainty principle. CMAJ. 2000, 1311-14.")] of clinical sites/practices, appropriate analysis and/or reporting and of course the willingness of individuals to take part. Each of these stages can individually or collectively be barriers to the successful delivery of a trial.
One of the most common problems, however, is with recruitment. Many studies fail to meet their recruitment targets, or fail to meet them without extending the length of the trials. McDonald et al [8], for example, found that of 114 trials, only 38 (31%) achieved their original recruitment target and 65 (53%) were extended.
The reasons why certain trials recruit well while others do not remain unclear [5]. Several potential limiting factors have been identified in the literature including constraints on clinician time [9.10], lack of available staff [11], impact on clinician autonomy, complexity of trial procedures [12], overestimating the number of patients available for study participation [13] and the perceived relevance of the research question to the clinicians [4]. Barriers to patients' involvement include lack of knowledge and trust in trials and unacceptability of randomisation [14].
A recent systematic review of interventions to improve recruitment to randomised controlled trials identified 27 eligible healthcare trials, including over 26,604 participants [15]. There were 24 studies involving interventions aimed directly at trial participants, while three evaluated interventions aimed at those recruiting participants. Many studies looked at recruitment to hypothetical trials and it is unclear how applicable these results are to real trials. Some interventions were effective in increasing recruitment: telephone reminders to non-respondents following a written invitation to take part in a trial (RR 2.66 95% CI 1.37 to 5.18), use of opt-out, rather than opt-in, procedures for contacting potential trial participants (RR 1.39 95% CI 1.06 to 1.84) and open designs where participants know which treatment they are receiving in the trial (RR1.25 95% CI 1.18 to 1.34).
An earlier systematic review with slightly different inclusion criteria [16] came to similar conclusions, although it also reported monetary incentives and culturally sensitive trial materials to be effective. Both reviews found the literature on the effect of recruitment interventions to be both sparse and often of poor methodological quality.
There are a number of proposals to increase recruitment to trials. Campbell et al [17] agreed that, to be successful, trialists should base their design on respecting the needs of patients and clinical professionals. Sackett [[7](/article/10.1186/1745-6215-12-74#ref-CR7 "Sackett DL: Why randomized controlled trials fail but needn't: 1. Failure to gain "coal-face" commitment and to use the uncertainty principle. CMAJ. 2000, 1311-14.")] also described how, in multi-centre RCTs, a responsibility of each site should be to involve and train those who will be recruiting and following-up trial participants. He stated that such action would enable collaborators to 'buy-in' to the trial and develop both ownership and commitment, terms more familiar in the business world than in health research.
One proposed solution to improving recruitment and retention is to adopt methodology from the business world to inform and structure trial management techniques [18]. Francis et al [18] developed a reference model (developed from marketing theory), which could be used for improving trial processes and as such, potentially improve recruitment to trials. However, whether this approach is useful in practice remains unclear.
This paper, therefore, seeks to a) describe the proposed business approach to trials and b) discuss the implementation of a business approach using insights gained from three case studies.
A business approach
Francis et al [18] first discussed whether clinical trials could be regarded as businesses and suggested that dimensions of running a successful trial include 'marketing', 'sales' and 'ongoing client management' which require a range of effective management techniques paralleling those for running a successful business. Francis et al used multiple methods to develop a reference model using insights from marketing theory, which could be used for ongoing assessment of the sales and marketing capability of a trial. The model has four domains: (1) Building Brand Values (2) Product and Market Planning (3) Making the Sale and (4) Maintaining Engagement. Each of the four domains has three components (see Figure 1). The twelve components are considered as links in a chain; if one link is underdeveloped then the whole chain is weakened. Table 1 includes our translation of the model into language that trialists are more familiar with.
Figure 1
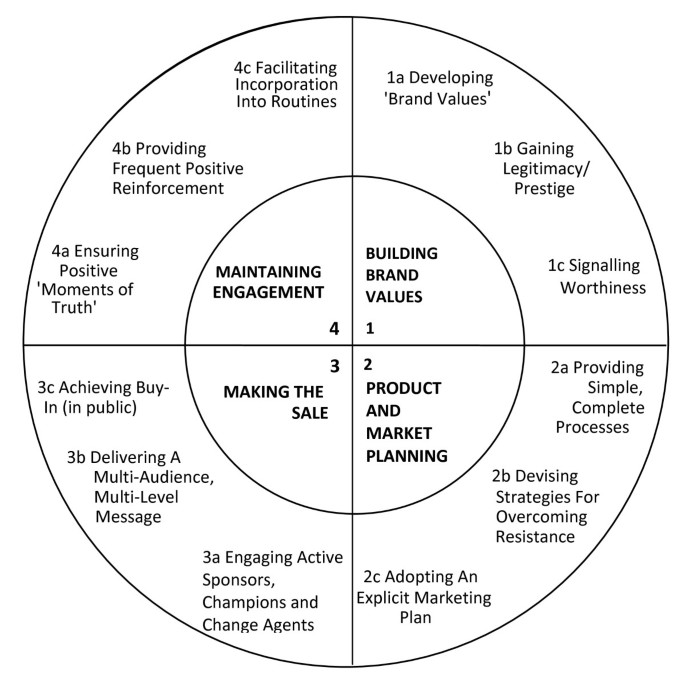
The business model. Illustrates the four domains of the model and the three components of each domain (from Francis et al [18]).
Table 1 Translation of business model components
Francis et al proposed that the model could be used in a variety of ways to help the conduct of clinical trials. These included: (1) to guide development of a recruitment plan, (2) as a diagnostic tool if trials have difficulties (and hence as a basis for deciding what type of remedial action to take), and (3) for auditing the progress of trials (to enable early identification of weaker managerial components and allow initiatives to strengthen them to be developed). As the model was developed from a theory-building process and only from a single trial, it was proposed as a tentative framework, and thus evidence is required from a range of trials to validate its findings.
To that end, we present below three case studies where the model was applied (these case studies represent trials known to the authors that had used the model). Each case study represents a slightly different use of the model, highlighting its versatility in the trials arena.
Implementation of the business model
Case study 1: the CRASH-2 trial (using the model to develop trial processes)
CRASH-2 is a large multinational randomised placebo controlled trial among trauma patients with, or at risk of, significant haemorrhage, to investigate the effects of antifibrinolytic treatment on death and transfusion requirement [19]. Recruitment commenced in May 2005 and was completed successfully in January 2010. In the set up phase of this trial, which aimed to recruit 20,000 trauma patients within 4.5 years, the business model developed by Francis et al [18] was applied to plan the overall trial management. Below we illustrate in detail how the twelve components of the model were used to guide the management of the trial.
Developing brand values
The 'CRASH' brand was already established with some patient organisations and several hundred emergency and critical care doctors worldwide following the successful delivery of the CRASH trial [20]. At the end of the CRASH trial 50 key collaborators were asked about the reasons they took part in the trial and what aspects of the trial coordinating centre's performance they would like to see improved. This information allowed the CRASH-2 coordinating team (the same team as ran the CRASH trial) to identify both the positive aspects and weaknesses of the CRASH 'brand'. Overall, the collaborators viewed their association with the CRASH trial as a very positive and worthwhile experience. Therefore, continued use of the original 'CRASH' theme in the logo and acronym for the CRASH-2 trial was considered useful to build on the positive image already established.
Gaining legitimacy and prestige
Factors which were identified by CRASH trial collaborators as giving the trial legitimacy and prestige were enshrined into the CRASH-2 trial. These factors included trial coordination by an academic institution, funding by a non-commercial organisation and management and overview by respected individuals in the relevant clinical and academic fields. Obtaining approval from all relevant ethics and regulatory agencies is required legally but this was also important for assuring collaborators about the ethical aspects of the trial and its compliance with relevant local legal requirements. In addition, approval for the trial was obtained from the World Health Organisation Ethics Committee as this was considered a positive 'tag' from a relevant prestigious organisation when marketing the trial globally. It was important to consider who the collaborating investigators viewed as 'prestigious' individuals and institutions' and engagement of these was maintained throughout the course of the trial.
Signalling worthiness
Recognising that even the simplest of trials would increase the workload for clinicians and their teams, the CRASH-2 trial utilised a simple pragmatic design and the trial-related procedures were kept to a minimum. CRASH-2 also emphasised the values that would appeal to individual collaborators, such as the importance of the trial question, contribution of the trial to advancing medical knowledge, how the trial might potentially influence patients' chances of survival in the future, positive aspects of being part of a global network with a common focus, potential for authorship or being named in the publication, potential to improve career prospects through being part of a research collaboration and 'hands-on' experience on how a trial is organised and conducted.
Providing simple, complete processes
The CRASH-2 trial identified and minimised those tasks which could only be done by the collaborators at recruiting sites (recruitment and follow-up of participants) and maximised those which could be done by the trial coordinating centre (TCC). For example, the TCC took responsibility for completing and assembling documents for ethics and regulatory application, liaising with ethics committees as much as possible, responding to any comments made and ensuring that reporting requirements were fulfilled. Randomisation methods also took into consideration local needs. For example, if international telephone lines were not available, an alternative randomisation method was made available. Multiple methods for data collection were also implemented taking into consideration the availability of fax machines, internet connection and computer software. Collaborators could choose a data collection method most suitable for their situation. All guidance on trial processes were made simple, translated into local languages where required and were easily accessible in the site study file and on the trial collaborators website. Without simplicity and complete processes, the trial team recognised that buy in was likely to be lower and the possibility of dropout from the trial would be increased.
Strategies for overcoming resistance
Factors were identified that might cause a potential collaborator to reject the CRASH-2 trial or undertake it with less than full commitment; for example colleagues not being supportive of the trial, anxieties about putting patients into a research trial, anxieties about how to explain the trial to relatives, the amount of paperwork involved, the lack of incentives for junior staff to recruit and not remembering to recruit. In a concerted attempt to address these issues directly, the TCC made training presentations and responses to frequently asked questions available to collaborators.
Adopting an explicit marketing plan
A formal marketing plan was developed that included a definition of target market segments i.e. groups that needed to buy-in to the trial. The CRASH-2 trial needed to engage a wide variety of people and organisations including funders, academics, clinicians, nurses, administrators, ethics committees, regulatory agencies, participants and their relatives, patient organisations, academic press and drug manufacturers. Each person/group had varying levels of interest but involvement by each was required for the success of the trial. The uninformed needed to be told about the trial and this was done primarily by providing simple information using a variety of means including personal contacts, email, post, journal articles and advertising in the scientific press such as the Lancet website. Those who still had concerns after reading the information were contacted personally by someone from the TCC or another individual likely to be viewed as having legitimacy and prestige. Those who were interested but slow to act were supported and encouraged by the TCC and other collaborators (for example a local national coordinator). Collaborators who were recruiting well were highlighted in, for example, trial newsletters and on the trial website. A number of key collaborators were identified as being vital for the success of the trial. For CRASH-2, they were the ones who demonstrated that they could recruit a large number of the patient population required for the trial and were able to ensure that data collection was of the highest quality. Many of these were engaged as national coordinators for their countries and assisted in engaging others to join the collaboration. They shared their experience of the trial and its processes so others could learn from them.
Engaging active sponsors, champions and change agents
In addition to clinical trialists understanding that a sponsor is the person/institution taking responsibility for the initiation, management and financing (or arranging the financing) of a trial [21], sponsors can also be considered as public advocates, champions as activists and change agents as facilitators of research [18]. It is also known that persuasion is more likely to occur if the advocate is respected and known personally to the prospective participant. For CRASH-2, this involved engaging and maintaining the support of multiple groups such as disease specific networks or societies, experts in the disease area (e.g. local lead clinicians who can promote the study in their area), patients and their representatives. As an international trial, engaging people within a country was required to ensure the message was relevant to that country and sensitive to their needs.
Delivering a multi-audience, multi-level message
For the CRASH-2 trial, multi-audience referred to the different interest groups involved and multi-level referred to that which "would appeal to the heart and the head". CRASH-2 needed to communicate in the language of the persons being targeted. For example, doctors in general needed to be convinced by the science of the trial and information on the scientific evidence to support the conduct of the trial was crucial. However, many nurses wanted to know more about the potential benefits for patients to convince them to collaborate. Although the same information was being presented, at collaborators meetings for example, the key messages needed to use language which addressed both sets of concerns.
Achieving buy-in (in public)
The trial team recognised that the trial impacted on more people at each site than solely the trial team. As such, the TCC advised local collaborators to ensure that local teams not directly involved in the trial, but who may be involved in the care of a trial participant, were aware of the trial, for example physiotherapists and pharmacists. To ensure that there was commitment to the trial, where possible (for example at collaborators meetings), collaborators were asked to state their commitment at the meeting because once someone states in public that they are willing to undertake an action, they are much more likely to actually do it [18].
Ensuring positive 'moments of truth'
When collaborators needed to make contact, the CRASH-2 team attempted to make all dealings with the TCC positive. To enable this, the CRASH-2 trial developed systems such as dedicated email accounts, frequently asked questions (FAQs) on the trial website, ensured prompt response to queries and developed in-house procedures to ensure all communications were handled efficiently within set time frames. However, there were times when TCC procedures failed and in those circumstances an honest response, with an apology and a clear plan to resolve the problem, was given. The TCC believed that this was likely to be viewed more positively than trying to pretend nothing was wrong.
Providing frequent positive reinforcement
Many of the doctors and nurses in the local trial team were involved in recruiting patients and completing the necessary paperwork for the trial. Recognising and rewarding these acts were seen as vital for them to continue to be motivated to deliver these tasks. Recognition included issuing certificates of participation, sending small tokens from the TCC after they recruited each patient and sending personalised text messages to thank them for their work. Also opportunities for networking, social interaction and the sharing of experiences at collaborators meetings were necessary.
Facilitating incorporation into routines
CRASH-2 attempted to incorporate as many trial procedures as possible within local routine. For example, trial participants generally needed to have cross-matching for blood transfusions; attaching a CRASH-2 trial label/logo to all blood transfusion forms assisted the doctors/nurses to remember the trial as part of their standard care routine.
Case study 2: the TXT2STOP trial (using the model as a diagnostic tool)
TXT2STOP is a trial of smoking cessation support via text (sms) messages http://www.txt2stop.org/. The trial had been informed by a pilot study which had successfully recruited 200 participants in 17 days. By the time of recruitment to the full trial, however, the external environment had changed dramatically with the introduction of the "no-smoking in public places" policy introduced in the UK and concurrent large-scale stop smoking multi-media campaigns being run by the UK National Health Service (NHS). This resulted in only 1056 participants being recruited to the trial in the first eight and a half months (instead of the expected 2000 participants). At this time (June 2008), the business model was used as a framework for understanding approaches to increasing trial recruitment.
The model resulted in a new conceptualisation of recruitment. According to the model the trial was being promoted to three distinct groups (market segments) - directly to smokers, primary care teams and smoking cessation services. The trial team carried out a review of the existing literature and spoke with members of each group to identify what people in each of the selected market segments would "value" (ie what would encourage them to 'sign-up') and to identify anything that put them off joining or recruiting to the trial. Text messages and letters to potential participants were developed focussing on the potential benefits of participation and the factors that have been reported to encourage participants to join trials [22–27]. To ensure that the benefits of involvement were not outweighed by costs to the GPs, appropriate funding was secured via service support costs (attributed to the UK NHS) [[28](/article/10.1186/1745-6215-12-74#ref-CR28 "Attributing revenue costs of externally-funded non-commercial research in the NHS (ARCO). http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_4125282.pdf
")]. Letters were written directly to smokers on GP lists so that the trial was not reliant on GP or nurse clinical time telling patients about the study. The value of the trial was endorsed by stating University links in the letters. The trial team engaged active sponsors and the trial was promoted on the NHS smoking cessation websites in England, Wales and Scotland. All promotion activities and adverts were monitored to evaluate their time and monetary costs and effectiveness. Cost-effective strategies were repeated and less effective strategies abandoned or revised.
The use of these new processes resulted in a further 4744 participants being recruited in the following 10 months and resulted in the trial being completed ahead of schedule. The proportion of eligible participants joining the trial also increased from 33% to 57%.
Case study 3: the LIFELAX trial - use of the model as an audit tool
LIFELAX is a trial of diet and lifestyle vs laxatives in the management of constipation in older people [29]. From the outset, the trial team attempted to consider the trial in business terms. The coordinating team identified potential gains and benefits that would accrue from participation in the trial and conveyed messages tuned to the distinctive needs of target groups (nursing staff, administrators etc) through presentations and training materials. A marketing plan was developed and adopted, which included the trial's unique selling points. Recognising there would be no direct material benefit for primary care doctors (general practitioners) in taking part, the marketing strategy was targeted towards identifying all potential gains and benefits that would accrue from participating in the trial. Despite this approach, the trial failed to recruit to target. In response to this the LIFELAX coordinating team used the model as an audit tool to retrospectively assess the recruitment strategies adopted within the trial and to learn lessons for future trials.
Using the model, the trial team identified that they had failed in their early attempts to recruit public advocates for the trial. It also identified that patient representative activities were limited to involvement in the Trial Steering Committee (TSC) only and would have benefitted from wider involvement throughout the trial processes. The team also believed that if they had adopted techniques to increase awareness of the participating general practices this would have resulted in greater support and commitment, eg through regular publication of lists of participating practices.
Salient lessons from all three case studies are summarised in Table 2.
Table 2 Implementation of the business model