Clinical evaluation of selected Yogic procedures in individuals with low back pain (original) (raw)
Abstract
The present study has been conducted to evaluate selected yogic procedures on individuals with low back pain. The understanding of back pain as one of the commonest clinical presentations during clinical practice made the path to the present study. It has also been calculated that more than three-quarters of the world's population experience back pain at some time in their lives. Twelve patients were selected and randomly divided into two groups, viz., group A yogic group and group B control group. Advice for life style and diet was given for all the patients. The effect of the therapy was assessed subjectively and objectively. Particular scores drawn for yogic group and control group were individually analyzed before and after treatment and the values were compared using standard statistical protocols. Yogic intervention revealed 79% relief in both subjective and objective parameters (i.e., 7 out of 14 parameters showed statistically highly significant P < 0.01 results, while 4 showed significant results P < 0.05). Comparative effect of yogic group and control group showed 79% relief in both subjective and objective parameters. (i.e., total 6 out of 14 parameters showed statistically highly significant (P < 0.01) results, while 5 showed significant results (P < 0.05).
Keywords: Asana, low back pain, pranayama, yoga
Introduction
History of practicing of yoga goes since time immemorial. Ancient sages had practiced yoga for the purpose of self-realization. They have realized the necessity of steady posture for a steady mind which is essential for spiritual uplift. The impossibility to disregard the greater benefits gained by the yoga practice for preserving the health has also been realized.[1]
Among the innumerable yogasanas, there are some which work specially on back. These asanas help in relaxing the tight muscles, reducing the tension and strengthening them. Yoga practices such asana and pranayama correct the vertebral curvatures, with respective angles and strengthen thoracic and abdominal cavities along with respiratory muscles supporting the maintenance of proper posture.
Aims and objectives
- To formulate a new feasible therapeutic approach in the management of low back pain using certain yogic practices.
- To evaluate the efficacy of the above formulated treatment plan in the management of low back pain patients and conduct a comparative study between yogic management group and control group.
Materials and Methods
- Patients attending the OPD of M.P.I.Y.N.E.R. and I.P.G.T. & R.A., Gujarat Ayurved University, Jamnagar, were selected for this study.
- Patients were questioned and examined on the basis of proforma and clinical tests such as straight leg raising test, femoral stretch test, etc.[2]
Criteria for selecting patients
Inclusion criteria
- Patients having back pain for more than 3 weeks were selected, irrespective of their religion, sex, occupation, caste and socioeconomic status.
- Age limit 30–60 years.
Exclusion criteria
- Patients suffering from any major concurrent illness which affects one or more systems of the body were excluded, e.g., ischemic heart disease, diabetes mellitus, tuberculosis, bone malignant tumors, etc.
- Patients having back pain due to non-spinal illnesses were excluded, e.g., Urinary tract infection (UTI), gastrointestinal GI diseases, uterine diseases.
- Patients having positive neurological signs were excluded.
- Patients of age below 30 years and above 60 years were excluded.
Plan of the study
Selected patients were randomly categorized into two groups:
Group A patients were treated as per the yogic treatment plan and
Group B patients were advised on proper diet and lifestyle.
Management of patients
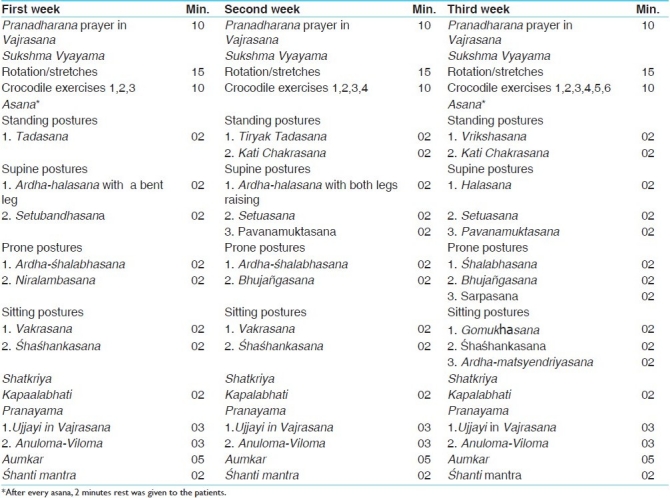
The yogic treatment plan is given in Table 1.
Table 1.
Group A: Yogic treatment plan[3–8]
Lifestyle and diet plan[9]
Patients of both the groups were advised to stick to the following lifestyle and diet plan.
- Morning: Wake-up, drinking a glass of lukewarm water
- Attend natural calls.
- Exercises and prayer.
- Breakfast - Daliya/pauva/sprouts/upma/oats/fresh fruits.
- Herbal tea/fruit juice/milk/butter milk. - Afternoon - Lunch - Roti, boiled vegetables, salad with raw vegetables, vegetable curry, small quantity of rice and dhal, fresh fruits, butter milk.
- After lunch, sit in Vajrasana for a few minutes. - Evening - Fruits/fruit juice/mamra/kakhra/milk/herbal tea.
- Night - Dinner - Khichadi/daliya, vegetable soup/mung soup, green leafy vegetables.
- After dinner walking for few minutes.
- Prayer in Vajrasana.
- Retire to bed.
Advice to the patients
Following advice was given regarding maintaining the correct posture, while bending, lifting objects, walking, standing, sitting and sleeping.
- Don’t lift by bending over. Instead, bend your hips and knees and then squat to pick up the object. Keep your back straight, and hold the object close to your body.
- Don’t twist your body while lifting.
- Push, rather than pull, when you must move heavy objects.
- If you must sit for long periods, take frequent breaks and stretch.
- Wear flat shoes or shoes with low heels.
- Exercise regularly. An inactive lifestyle contributes to lower back pain.
Clinical assessment and grade of total effect
The improvement in the patients was assessed mainly on the basis of relief in the cardinal symptoms of the disease. To assess the effect of therapy objectively, all the signs and symptoms were given scoring pattern depending upon their severity as below:
Subjective criteria
The subjective criteria for assessment of pain are as follows.[10]
- Pain Intensity
No pain: 0
Mild pain: 1
Moderate pain: 2
Severe pain: 3
Worst possible pain: 4 - Sleeping
Perfect sleep: 0
Mildly disturbed sleep: 1
Moderately disturbed sleep: 2
Highly disturbed sleep: 3
Totally disturbed sleep: 4 - Personal care (washing, dressing, etc.)
No pain; no restrictions: 0
Mild pain; no restrictions: 1
Moderate pain; needs to go slowly: 2
Moderate pain; needs some assistance: 3
Severe pain; needs 100% assistance: 4 - Travel (driving, etc.)
No pain on long trips: 0
Mild pain on long trips: 1
Moderate pain on long trips: 2
Moderate pain on short trips: 3
Severe pain on short trips: 4 - Work
Can do usual work plus unlimited extra work: 0
Can do usual work; no extra work: 1
Can do 50% of usual work: 2
Can do 25% of usual work: 3
Cannot work: 4 - Recreation
Can do all activities: 0
Can do most activities: 1
Can do some activities: 2
Can do a few activities: 3
Cannot do any activity: 4 - Frequency of pain
No pain: 0
Occasional pain; 25% of the day: 1
Intermittent pain; 50% of the day: 2
Frequent pain; 75% of the day: 3
Constant pain: 4 - Lifting
No pain with heavy weight: 0
Increased pain with heavy weight: 1
Increased pain with moderate weight: 2
Increased pain with light weight: 3
Increased pain with any weight: 4 - Walking
No pain till any distance: 0
Increased pain after 1 mile: 1
Increased pain after 1/2 mile: 2
Increased pain after 1/4 mile: 3
Increased pain with all walking: 4 - Standing
No pain after several hours: 0
Increased pain after several hours: 1
Increased pain after 1 hour: 2
Increased pain after 1/2 hour: 3
Increased pain with any standing: 4

Objective criteria
The objective criteria for assessment of pain are as follows.[8]
- Forward flexion: ...............cm
- Left lateral flexion: ...........cm
- Right lateral flexion: ........cm
General Observations
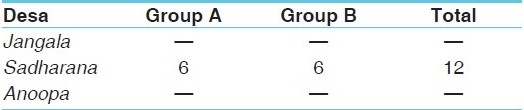
In this study, 12 individuals having low back pain were registered, irrespective of their socioeconomic status, gender, religion, etc. They were randomly divided into two groups. The distribution of patients according to various factors is given in Tables 2–19.
Table 2.
Distribution of registered individuals
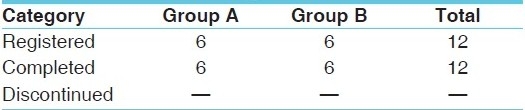
Table 19.
Chronicity wise distribution
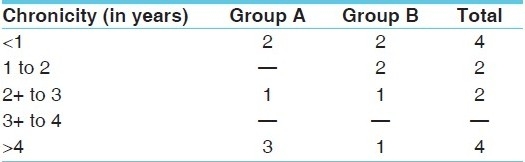
Table 3.
Age wise distribution
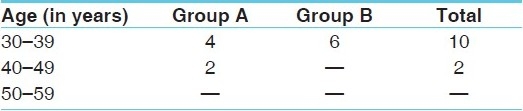
Table 4.
Gender wise distribution

Table 5.
Marital status wise distribution

Table 6.
Religion wise distribution
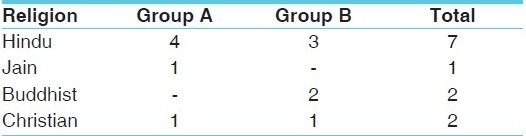
Table 7.
Occupation wise distribution
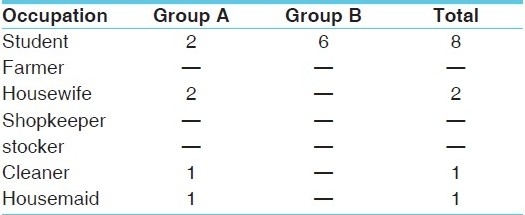
Table 8.
Education wise distribution
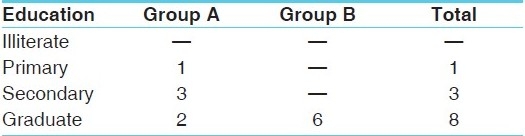
Table 9.
Socioeconomic status wise distribution
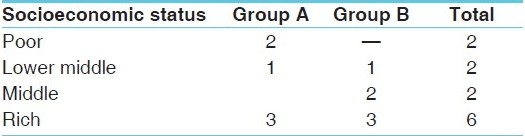
Table 10.
Diet wise distribution

Table 11.
Addiction wise distribution
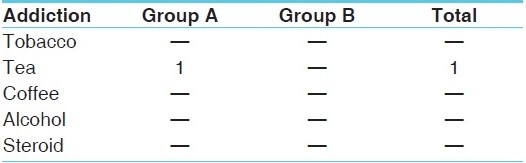
Table 12.
Deha Prakriti wise distribution
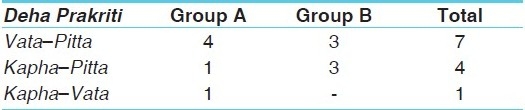
Table 13.
Agni wise distribution
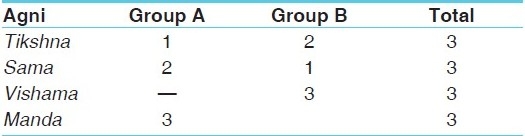
Table 14.
Kostha wise distribution
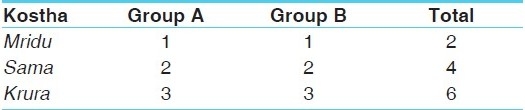
Table 15.
Habitat wise distribution

Table 16.
Family history wise distribution

Table 17.
Onset wise distribution

Table 18.
Desha wise distribution
Effects of the treatments
Subjective and objective parameters were used to assess the severity of the disease and its impact on the quality of life of the patients. Subjective parameters were evaluated by using a system of 10 individual scores and their total score, while objective parameters were assessed with a system of three individual scores. These subjective and objective categories were analyzed and compared using statistics. Particular scores drawn for yogic management group (Group A) and control group (group B) were individually analyzed before and after treatment and values of both the groups were compared using standard statistical protocols, such as paired and unpaired Student's _t_-test. The following details were drawn based on the results of statistical analysis and comparison.
In yogic management group, the following was found as the progress after the treatment [Table 20].
Table 20.
Results of yogic treatment group
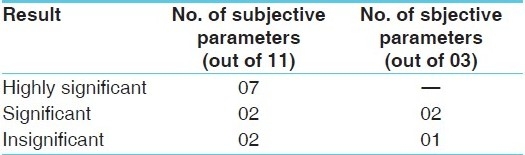
These results indicate the need for an improvement in those insignificant subjective and objective parameters such as sleeping, walking, and right lateral flexion.
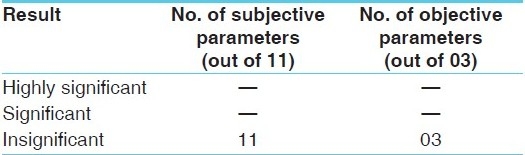
In control group, the following was extracted as statistical results [Table 21].
Table 21.
Results of control group
A comparison made between the yogic management group and the control group yielded the following results [Table 22].
Table 22.
Comparison between yogic management group and control group
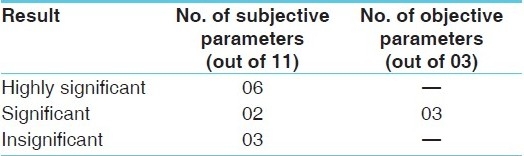
Once again, there is a point of caution here. Among the 11 subjective parameters, 3 are found to be statistically insignificant and they are sleeping, work and walking. It again confirms the previous result by being incapable to produce proper effect for the parameters of sleeping and walking.
Discussion
Disease (low back pain) occurrence was observed maximally at the age of 30–39 years. It may be due to more physical activity during this age and maintaining wrong body postures while working, sitting, standing, or sleeping. Furthermore, there may be fast food (wrong food combination) intake in this busy period of life, and lack of judiciously selected curative exercises can also be considered as causes of this disease. Highest incidence of low back pain was observed among female gender. This may be due to excessive household work, lack of rest and relaxation and also maintaining wrong body postures, especially while working. Students were mostly affected by this disease. When considering the students, they may be studying for long hours in one position due to extreme competition; moreover, they are not willing to spend time for physical exercises. This sitting position also may be incorrect. One of these facts or all factors together contribute in causing low back pain among students. Majority of patients were found from rich background. Two things can be taken into consideration here. Firstly, sedentary lifestyle and work-related stress of these people and, secondly, the institute being a self-financed one, the treatment was limited to patients who could afford. Obviously due to this reason it has restricted the people of low socioeconomic status, registering in this study.
Effect of the therapy
Overall effects of group A (yogic group)
Yogic treatment provided 79% relief in both subjective and objective parameters [i.e., 7 out of 14 parameters showed statistically highly significant (P < 0.01) results, while four showed significant results (P < 0.05)].
Comparative effect of group A (yogic group) and group B (control group)
Yogic treatment provided 79% relief in both subjective and objective parameters [i.e., 6 out of 14 parameters showed statistically highly significant (P < 0.01) results, while 5 showed significant results (P < 0.05)].
Conclusion
At the end of the study, the following points can be concluded on the basis of the observations drawn and the results achieved.
- Low back pain can be prevented in a majority of cases, provided maintaining of correct posture, regular and proper exercises, intake of proper selections of food and preserving proper mental health are all followed.
- Causes of back pain are understood as multifactorial. Highly successful management of multifactorial disease depends on multi-focus treatment approach. Since yoga is a holistic method, it is equipped with multi-target approaches. Hence, testified successful results have been obtained.
- Results of this study are encouraging but a trial should be conducted on a large sample in a long duration of time with clinical investigations for a final conclusion.
References
- 1.Haslett C, Chilvers ER, Hunter JA, Boon NA. Davidson's Principles and Practice of Medicine. 18th ed. New york : Churchill Livingstone; 1999. p. 815. [Google Scholar]
- 2.Munro J, Edwards C. Macleod's Clinical Examination. 9th ed. New york: Churchill Livingstone; 1999. pp. 274–90. [Google Scholar]
- 3.Saraswati SS. Asana Pranayama Mudra Bandha. India: Bihar School of Yoga; 1999. pp. 23–44. (54-5, 62-5, 109-10, 123-6, 139-42, 197-8, 202-7, 219, 225-6, 271-4, 291-2, 379-85, 392-93). [Google Scholar]
- 4.Vincente P. Yoga Mimansa. 1990 Apr;29(1) [Google Scholar]
- 5.Coulter DH. Anatomy of Hatha Yoga. Delhi: Motilal Banarsidass Publishers; 2006. pp. 82–4. (160-5, 251-3, 284-92, 296-300, 405-6). [Google Scholar]
- 6.Digambaraji S, Kokaje RS. Hatha Pradeepika of Svatmarama, Kaivalyadhama. 2nd ed. Pune: S.M.Y.M. Samiti; 1998. [Google Scholar]
- 7.Saraswati SS, Saraswati SN, Saraswati SM. A systematic course in the ancient tantrik techniques of yoga and kriya. Monghyr, India: Bihar School of Yoga; 2004. [Google Scholar]
- 8.Vasu R.B.S.C. The Gheranda Samhita. India: Sri Satguru Publications; 1996. [Google Scholar]
- 9.Lindlahr H. Practice of Natural Therapeutics. Pondichery: All India press; 2004. [Google Scholar]
- 10.Magee DJ. Orthopedic Physical Assessment. 4th Edition. Missouri: Saunders; 2006. pp. 450–451. [Google Scholar]