Designing, validation, and feasibility of integrated yoga therapy module for chronic low back pain (original) (raw)
Abstract
Context:
Chronic low back pain (CLBP) is a significant public health problem that has reached epidemic proportions. Yoga therapy has emerged as one of the complementary and alternative therapies for CLBP.
Aim:
The present study reports the development, validation, and feasibility of an integrated yoga therapy module (IYTM) for CLBP.
Settings and Design:
This study was carried out at the SVYASA Yoga University, Bengaluru, South India. The IYTM for CLBP was designed, validated, and later tested for feasibility in patients with CLBP.
Materials and Methods:
In the first phase, IYTM for CLBP was designed based on the literature review of classical texts and recently published research studies. In the second phase, designed IYTM (26 yoga practices) was validated by thirty subject matter (yoga) experts. Content validity ratio (CVR) was analyzed using Lawshe's formula. In the third phase, the validated IYTM (20 yoga practices) was tested on 12 patients for pain, disability and perceived stress at baseline and after 1-month of this intervention.
Results:
A total of 20 yoga practices with CVR ≥0.33 were included, 6 yoga practices with CVR ≥0.33 were excluded from the designed IYTM. The feasibility study with validated IYTM showed significant reduction in numerical pain rating scale (P = 0.02), Oswestry disability scale (P = 0.02), and Perceived Stress Scale (P = 0.03).
Conclusion:
The designed IYTM was validated by thirty yoga experts and later evaluated on a small sample. This study has shown that the validated IYTM is feasible, had no adverse effects and was useful in alleviating pain, disability, and perceived stress in patients with CLBP. However, randomized control trials with larger sample are needed to strengthen the study.
Keywords: Chronic low back pain, content validity ratio, integrated yoga therapy module
INTRODUCTION
Chronic low back pain (CLBP) defined as back pain lasting >12 weeks. Low back pain (LBP) is a common and costly health problem; 70–80% of adults are afflicted by it at some point of time in their lives,[1,2] expenditures attributed to spine problems were $2580 per person. The CLBP 42% prevalence rate.[3] In addition to the pain, CLBP has also resulted in increased psychological distress,[4] increased disability, and reduced health-related quality of life.[5,6] LBP was identified by the Pan American Health Organization as one of the top three occupational health problems.[7] The complex nature of the CLBP demand multidimensional approach to treatment.[8] There is a wide variety of treatments available for CLBP. A pilot study by Eisenberg et al., showed that, multidisciplinary (integrated) approach, which includes conventional care, complementary, and alternative medicines (CAM) or both is promising in the treatment of patients with persistent LBP.[9]
In the recent past yoga has emerged as one of the evidence-based CAM in CLBP, which is widely used across the globe. According to national surveys, yoga practice has increased, with over 10 million Americans practicing yoga for health reasons in 2002 and over 13 million in 2007.[10,11] Popularity of yoga has led to several schools of yoga viz., Iyengar yoga, Viniyoga, Astanga yoga, Hatha yoga, Laughter yoga, Sudarshana kriya yoga, etc. Stress-related LBP seems to be an appropriate indication for yoga therapy as large number of literature supports the same.[12] Literature review reveals that, Viniyoga, Hatha yoga, Iyengar yoga, and Integrated yoga are the most commonly used forms to treat LBP.[13,14,15]
In a systematic review, Chou and Huffman found that, yoga therapy is effective for sub-acute or CLBP. In a large sample study of 6 weeks, Viniyoga was found to be superior to conventional exercise. In another review by Posadzki and Ernst which included four randomized controlled trials (RCTs) apart from Chou and Huffman's review, revealed that the intervention of Iyengar and Viniyoga for the period of 12–24 weeks were beneficial in CLBP.[14] Tekur et al., intervened CLBP patients with 7-day intensive residential integrated yoga and found it beneficial for pain, disability, anxiety, stress, and quality of life in patients with CLBP.[15,16,17] Another review of Cramer et al., found 12 studies meeting inclusion criteria, reported on Viniyoga, Iyengar yoga, and Hatha yoga interventions for CLBP. Ten of these studies were included in the meta-analysis, which strongly favored over control interventions for reducing pain and disability scores.[18]
Different schools of yoga have varying proportions of physical, breathing, and mind activities executed through varied practices. Most of these studies found a varied range of positive benefits on CLBP. These advances have given us a lead to develop a standardized module by extracting the best yoga practices out of different schools of yoga, as they had a common objective “_chitta vritti nirodhah_” (voluntary mastery over the modifications of the mind).[19] The present study report development, validation, and feasibility of validated integrated yoga therapy module (IYTM) for CLBP.
MATERIALS AND METHODS
The designing, validation, and feasibility of IYTM for CLBP [Figure 1] were carried out in the following steps:
Figure 1.

Depicts the steps in the development of the integrated yoga therapy module for chronic low back pain
First phase: Designing of integrated yoga therapy module for chronic low back pain
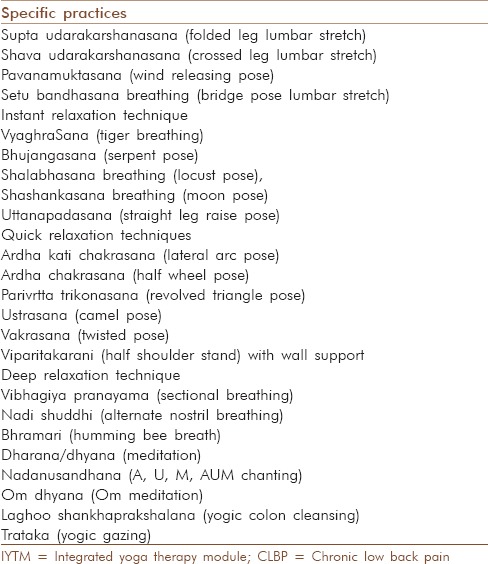
Designing the IYTM for CLBP was done by using classical texts,[19,20,21] recent books on back pain,[22,23,24,25,26,27] peer-reviewed research publications and other related sources for the development of IYTM for CLBP.[14,15,16,17,18,28,29,30] Underlying mechanism of the beneficial effects of each yoga practice yet to be explored. Twenty-six yoga practices were tabulated under designed IYTM, which had strong support for beneficial effects on CLBP [Table 1].
Table 1.
Designed IYTM for CLBP based on literature review
Second phase: Validation of integrated yoga therapy module for chronic low back pain
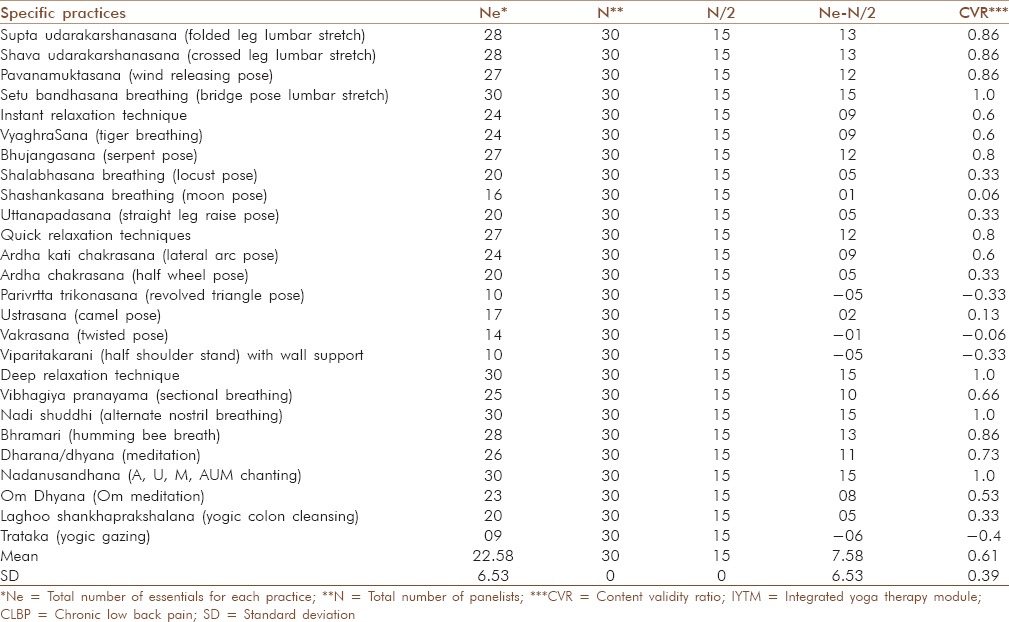
Validation of designed IYTM-26 yoga practices [Table 2] was done with the help of subject matter expert raters (SMEs)/experts, viz. Doctor of Medicine in Yoga, Doctorates in Yoga with minimum experience of 5 years in the field of yoga, and yoga therapists with a masters in Yoga having minimum experience of 7 years after post formal education. Thirty SMEs were consented to participate in the evaluation. They marked content validity on a three (0–2) point scale, viz. Not necessary - 0, Useful but not essential - 1, Essential - 2. After validation, data were analyzed using Lawshe's content validity ratio (CVR).[31]
Table 2.
Validated IYTM for CLBP with CVR as per Lawshe formula
Third phase: Feasibility study
Twelve patients (5 male and 7 female) with age 36.75 ± 3.79 having nonspecific CLBP who consented to participate in the study were recruited from SVYASA Yoga University, Bengaluru, India. The inclusion criteria were (a) History of CLBP of more than 12 weeks (b) pain in the lumbar spine with or without radiation to legs and (c) age between 18 and 45 years. Exclusion criteria were, (a) CLBP due to organic pathology in the spine, like malignancy (primary or secondary) or chronic infections investigated by X-ray of the lumbar spine.[32] The study was approved by the institutional review board and the ethical committee of the University. Signed informed consent was obtained from all patients. All the patients have come with X-ray/magnetic resonance imaging/computed tomography, none of them had sciatica. They were intervened with the validated IYTM [Table 3] for 1-month (1 h/day, 5 days a week). Assessed for pain, disability, and perceived stress by using the numerical rating scale (NRS), oswestry disability index (ODI), and perceived stress scale (PSS), respectively at baseline and after 1-month of the intervention. All the 12 patients completed the intervention. There were no adverse effects observed during the study period.
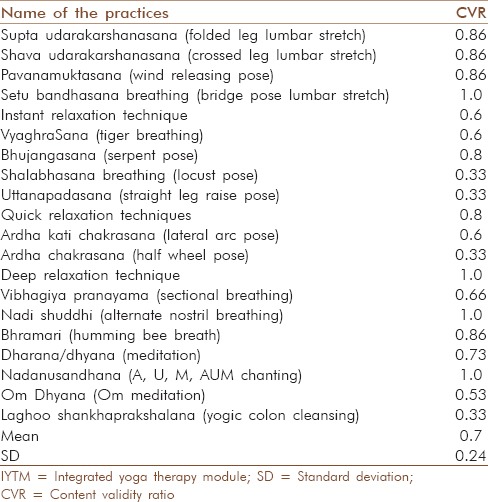
Table 3.
IYTM practices with CVR ≥0.33 need to be retained (validate IYTM)
RESULTS
Results: Content validity
30 SMEs validated all the 26 practices of designed IYTM for CLBP. Data were analyzed for content validity using Lawshe's CVR.[31] Lawshe's formula is CVR = (ne − N/2)/(N/2), where, CVR = Content validity ratio, ne = number of SME panelists indicating “essential,” N = Total number of SME panelists, SME. CVR was calculated for all the 26 practices and tabulated [Table 2]. Among them, 20 yoga practices [Table 3] with CVR ≥0.33 were included, 6 yoga practices [Table 4] with CVR ≤0.33 were excluded from designed IYTM. Mean CVR of validated IYTM was 0.7 ± 0.24. As per the Lawshe's CVR ratio the minimum value for 30 SMEs is 0.33, it means the CVR ratio achieved to evaluate the content validity of the IYTM is found to be significant and the validated IYTM is valid to be used as an intervention for CLBP patients.
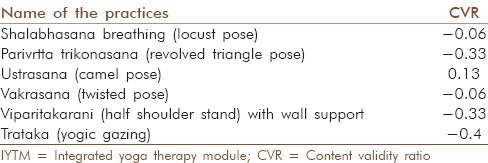
Table 4.
IYTM practices with CVR ≦0.33 need to be deleted/removed
Results: Feasibility study
Twelve CLBP patients, who consented to the study, were intervened with validated IYTM, which consisted of 20 practices with CVR ≥0.33. Assessments were done at baseline and after 1-month of intervention. All patients completed the intervention; no adverse effects were noticed during the study. Data were analyzed using Wilcox test, which showed a significant reduction in pain (P = 0.02), disability (P = 0.02), and perceived stress (P = 0.03).
DISCUSSION
This study was planned in three phases viz. (a) designing of IYTM for CLBP (b) validation of IYTM for CLBP by SMEs (c) feasibility study of validated IYTM.
- In the first phase, integrated yoga module for CLBP was designed based on literature reviews of traditional textual references, recent research publications, and advice from yoga experts. Our comprehensive search in traditional yogic texts did not yield any direct references for yogic practices with the ability of improving the CLBP. However, recent Hatha yogic texts[19,20] lay more emphasis on improving health through different yogic practices. In addition to that, recent findings of several schools of yoga in their research studies on CLBP were helped in formulating IYTM for CLBP
- Subject matter (Yoga) experts (SMEs) were involved in the validation process. CVR was calculated for all the 26 practices of designed IYTM. CVR was developed by C. H. Lawshe. It is essentially a method for gauging agreement among raters or judges regarding how essential a particular item is. Lawshe (1975) proposed that each of the SMEs on the judging panel responds to the following question for each item: “Is the skill or knowledge measured by this item “essential,” “useful, but not essential” or “not necessary.” According to Lawshe, if more than half of the panelists indicate that an item is essential, that item has at least some content validity. Greater levels of content validity exist as larger numbers of the panelists agree that a particular item is essential. Using these assumptions, Lawshe developed a formula termed the CVR: Lawshe's formula is CVR = (ne−N/2)/(N/2), where the CVR, number of SME panelists indicating “essential,” total number of SME panelists. This formula yields values, which range from +1 to −1; positive values indicate that at least half the SMEs rated the item as essential. The mean CVR across the items may be used as an indicator of overall.
Content validity ratio was calculated for all the 26 practices of designed IYTM. Among them, 20 practices with CVR ≥0. 33 included in the validated IYTM [Table 3]. Other six practices with CVR ≤0.33 viz., Sasankasana breathing (0.06), Parivritta trikonasana (−0.33), Ustrasana/Ardha ustrasana (0.13), Vakrasana/Ardhamastyendrasana (−0.06), Viparitakarani with wall support (−0.33), Trataka (−0.4). These practices were either complimentary poses for an important posture to align the body and mind level. Due to these reasons, most of the experts have not considered them as essential for CLBP. Apart from those 6 practices, all other 20 practices were considered to be essential for CLBP; this made the final CVR ratio satisfy the minimum value as per Lawshe's CVR ratio.
Twelve patients were intervened by validated IYTM (20 practices), and they were assessed pre- and post-intervention for pain (NRS), disability (ODI), and perceived stress (PSS). All three outcome measures, showed statistically significant (P < 0.005) positive impact of validated
IYTM on CLBP patients. All 12 patients completed the intervention, there were no adverse effects noticed during the study. In case of nonspecific CLBP, validated IYTM may use as complimentary intervention. However, RCT with larger samples are needed to validate its efficacy as a primary intervention.
CONCLUSION
Integrated yoga therapy module having 26 practices for CLBP, was designed on the basis of literature review, which was validated by 30 Yoga experts. Among 26 yoga practices, 20 were found to be essential (CVR ≥0.33) and 6 not essential (CVR ≤0.33) for CLBP. Feasibility study showed that validated IYTM was found to be beneficial for pain, disability, and perceived stress in patients with CLBP. The present validation brings greater acceptability and better therapy module for CLBP.
LIMITATIONS OF THE STUDY
In the present study, validated IYTM was only tested on a small sample of 12, however, RCTs with the larger sample can become a curtain raiser for future work.
ACKNOWLEDGMENT
We would like to thank the staff of SVYASA Yoga University, Bengaluru, India for their support throughout the study. We would like to thank Dr. Judu I. SVYASA University, Bengaluru for statistical analysis.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.McBeth J, Jones K. Epidemiology of chronic musculoskeletal pain. Best Pract Res Clin Rheumatol. 2007;21:403–25. doi: 10.1016/j.berh.2007.03.003. [DOI] [PubMed] [Google Scholar]
- 2.Breivik H, Borchgrevink PC, Allen SM, Rosseland LA, Romundstad L, Hals EK, et al. Assessment of pain. Br J Anaesth. 2008;101:17–24. doi: 10.1093/bja/aen103. [DOI] [PubMed] [Google Scholar]
- 3.Martin BI, Deyo RA, Mirza SK, Turner JA, Comstock BA, Hollingworth W, et al. Expenditures and health status among adults with back and neck problems. JAMA. 2008;299:656–64. doi: 10.1001/jama.299.6.656. [DOI] [PubMed] [Google Scholar]
- 4.Deyo RA, Mirza SK, Martin BI. Back pain prevalence and visit rates: Estimates from U.S. national surveys, 2002. Spine (Phila Pa 1976) 2006;31:2724–7. doi: 10.1097/01.brs.0000244618.06877.cd. [DOI] [PubMed] [Google Scholar]
- 5.Chou R, Qaseem A, Snow V, Casey D, Cross JT, Jr, Shekelle P, et al. Diagnosis and treatment of low back pain: A joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007;147:478–91. doi: 10.7326/0003-4819-147-7-200710020-00006. [DOI] [PubMed] [Google Scholar]
- 6.Currie SR, Wang J. Chronic back pain and major depression in the general Canadian population. Pain. 2004;107:54–60. doi: 10.1016/j.pain.2003.09.015. [DOI] [PubMed] [Google Scholar]
- 7.Cherkin DC, Deyo RA, Wheeler K, Ciol MA. Physician variation in diagnostic testing for low back pain. Who you see is what you get. Arthritis Rheum. 1994;37:15–22. doi: 10.1002/art.1780370104. [DOI] [PubMed] [Google Scholar]
- 8.Salzberg L. The physiology of low back pain. Prim Care. 2012;39:487–98. doi: 10.1016/j.pop.2012.06.014. [DOI] [PubMed] [Google Scholar]
- 9.Eisenberg DM, Buring JE, Hrbek AL, Davis RB, Connelly MT, Cherkin DC, et al. A model of integrative care for low-back pain. J Altern Complement Med. 2012;18:354–62. doi: 10.1089/acm.2011.0408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Shannahoff-Khalsa DS. Patient perspectives: Kundalini yoga meditation techniques for psycho-oncology and as potential therapies for cancer. Integr Cancer Ther. 2005;4:87–100. doi: 10.1177/1534735404273841. [DOI] [PubMed] [Google Scholar]
- 11.Moadel AB, Shah C, Wylie-Rosett J, Harris MS, Patel SR, Hall CB, et al. Randomized controlled trial of yoga among a multiethnic sample of breast cancer patients: Effects on quality of life. J Clin Oncol. 2007;25:4387–95. doi: 10.1200/JCO.2006.06.6027. [DOI] [PubMed] [Google Scholar]
- 12.Wren AA, Wright MA, Carson JW, Keefe FJ. Yoga for persistent pain: New findings and directions for an ancient practice. Pain. 2011;152:477–80. doi: 10.1016/j.pain.2010.11.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Verrastro G. Yoga as therapy: When is it helpful? J Fam Pract. 2014;63:E1–6. [PubMed] [Google Scholar]
- 14.Posadzki P, Ernst E. Yoga for low back pain: A systematic review of randomized clinical trials. Clin Rheumatol. 2011;30:1257–62. doi: 10.1007/s10067-011-1764-8. [DOI] [PubMed] [Google Scholar]
- 15.Tekur P, Singphow C, Nagendra HR, Raghuram N. Effect of short-term intensive yoga program on pain, functional disability and spinal flexibility in chronic low back pain: A randomized control study. J Altern Complement Med. 2008;14:637–44. doi: 10.1089/acm.2007.0815. [DOI] [PubMed] [Google Scholar]
- 16.Tekur P, Nagarathna R, Chametcha S, Hankey A, Nagendra HR. A comprehensive yoga programs improves pain, anxiety and depression in chronic low back pain patients more than exercise: An RCT. Complement Ther Med. 2012;20:107–18. doi: 10.1016/j.ctim.2011.12.009. [DOI] [PubMed] [Google Scholar]
- 17.Tekur P, Chametcha S, Hongasandra RN, Raghuram N. Effect of yoga on quality of life of CLBP patients: A randomized control study. Int J Yoga. 2010;3:10–7. doi: 10.4103/0973-6131.66773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Cramer H, Lauche R, Haller H, Dobos G. A systematic review and meta-analysis of yoga for low back pain. Clin J Pain. 2013;29:450–60. doi: 10.1097/AJP.0b013e31825e1492. [DOI] [PubMed] [Google Scholar]
- 19.Taimni IK. 5th ed. Illinois: Theosophical Publishing House; 1992. The Science of Yoga: A Commentary on the Yoga Sutras of Patanjali in the Light of Modern Thought. [Google Scholar]
- 20.Svatmarama . 4th ed. Madras: Adyar Library and Research Centre; 1994. Hatha Yoga Pradipika of Svatmarama. [Google Scholar]
- 21.Digambarji S, Gharote ML. 1st ed. Lonavala: Kaivalyadhama S.M.Y.M Samiti; 1978. Gheranda Samhita. [Google Scholar]
- 22.Nagendra HR, Nagarathna R. Bangalore: Swami Vivekananda Yoga Prakashana; 2008. Integrated approach of yoga therapy for positive health. [Google Scholar]
- 23.Nagarathna R, Nagendra HR. Bangalore: Swami Vivekananda Yoga Prakashana; 2007. Yoga for Back Pain. [Google Scholar]
- 24.Saraswati SS. Munger, Bihar: Yoga PublicationsTrust; 2005. Yoga Darshana. [Google Scholar]
- 25.Saraswati SS. Munger, Bihar: Yoga PublicationsTrust; 2004. Surya Namaskara. [Google Scholar]
- 26.Iyengar BK. London: Harper Collins Publishers; 1993. Light on Yoga. [Google Scholar]
- 27.Acharya I, Basavaraddi IV. New Delhi: Morarji Desai National Institute of Yoga; 2007. Yoga therapy series – Yogic Management of Diseases. [Google Scholar]
- 28.Sherman KJ, Cherkin DC, Erro J, Miglioretti DL, Deyo RA. Comparing yoga, exercise, and a self-care book for chronic low back pain: A randomized, controlled trial. Ann Intern Med. 2005;143:849–56. doi: 10.7326/0003-4819-143-12-200512200-00003. [DOI] [PubMed] [Google Scholar]
- 29.Sherman KJ, Cherkin DC, Wellman RD, Cook AJ, Hawkes RJ, Delaney K, et al. A randomized trial comparing yoga, stretching, and a self-care book for chronic low back pain. Arch Intern Med. 2011;171:2019–26. doi: 10.1001/archinternmed.2011.524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Chuang LH, Soares MO, Tilbrook H, Cox H, Hewitt CE, Aplin J, et al. A pragmatic multicentered randomized controlled trial of yoga for chronic low back pain: Economic evaluation. Spine (Phila Pa 1976) 2012;37:1593–601. doi: 10.1097/BRS.0b013e3182545937. [DOI] [PubMed] [Google Scholar]
- 31.Lawshe CH. A quantitative approach to content validity. Pers Psychol. 1975;28:563–75. [Google Scholar]
- 32.Spitzer WO, Leblanc FE, Dupis M. Scientific approach to the assessment and management of activity related spinal disorders: A monograph for clinicians. Spine. 1987;12:75. [PubMed] [Google Scholar]