Do research papers provide enough information on design and material used in ankle foot orthoses for children with cerebral palsy? A systematic review (original) (raw)
Abstract
Objectives
The purpose of this article is to determine how many of the current peer-reviewed studies of ankle foot or-thoses (AFOs) on children with cerebral palsy (CP) have included adequate details of the design and material of the AFO, to enable the study to be reproduced and outcomes clearly understood.
Methods
A thorough search of studies published in English was conducted in March 2015, with no restriction on dates, within all major databases using relevant phrases. These searches were then supplemented by tracking all key references from the appropriate articles identified.
Study selection
The inclusion criteria were as follows: (1) population - children with CP; (2) intervention - AFOs; and (3) outcome measure. One reviewer extracted data regarding the characteristics of the included studies, with the extracted data checked for accuracy and completeness by a second reviewer.
None of the studies reviewed gave adequate details of the AFOs. Only 3.6% (n = 2) of papers tested the stiffness. Many studies (54.5%) did not describe the material used nor the material thickness (72.7 %). None of them gave any clinical justification for the chosen design of AFO.
Conclusions
There is a clear paucity of detail regarding the design and material used in AFOs on studies involving children with CP. Such a lack of detail has the potential to affect the validity of the reported outcomes, the ability to reproduce the studies and may misinform clinical practice.
Keywords: orthotic devices; cerebral palsy; AFO, orthoses; materials testing; clinical outcomes
Introduction
Patients with cerebral palsy (CP) are the most commonly observed participants in gait laboratories.1 CP is thought to be the most common cause of serious physical disability in childhood, although it only affects two to three per 1000 live births.2 CP is primarily characterised by central nervous system abnormalities, such as loss of selective motor control and abnormal muscle tone. As a result of growth, these primary characteristics often lead to secondary deficits, including bony deformities, muscle contractures and gait abnormalities.3 In addition to surgical and therapeutic interventions, orthoses play an important role in the management of the child with CP.
An orthosis is defined by the International Standards Organisation as ‘an externally applied device used to modify the structural and functional characteristics of the neuromuscular and skeletal system’.4 Ankle foot orthoses (AFOs) are commonly prescribed to children with CP in an attempt to improve their gait; they are defined as ‘ortho-ses that encompass the ankle joint and the whole or part of the foot’.5 AFOs are intended to control motion, correct deformity and/or compensate for weakness.6
There are a wide variety of AFOs used in clinical practice, which are characterised by their design, the material used and the stiffness of that material. Changing any of these three components will alter the control the AFO has on the patient’s gait.7 The inherent rigidity of an AFO has been demonstrated to play an important role in determining its biomechanical function and needs to be optimal to positively influence pathological gait.8,9 The rigidity of an AFO may be determined by a number of factors, such as the mechanical properties of the material, the trim lines, the material thickness and the shape of the superstructure.10-13 Lunsford14 reported that the variation in the material properties used in the manufacturer of an AFO may influence the flexibility at the ankle and metatarsophalangeal joints (MTPJs) of these ‘rigid’ devices and it is documented in the current literature that differences in mechanical properties of the AFO occur as a consequence of relatively minor variations in AFO design.15-18
Limitations relating to AFO design and inappropriate prescription to facilitate for an individual’s movement pattern can hinder the effectiveness of AFOs.19 By the same reasoning, inappropriate design and prescription of AFOs can have substantial influence on research results.
If changing the design, material and stiffness alters the control the AFO has on the individual’s gait, then it stands to reason that a detailed description of the AFO used in research studies is imperative, along with a justification of why the AFO was designed with each particular characteristic and what the aim of the design is. For example, if one uses a 3-mm natural polypropylene AFO with trim lines behind the MTPJs, with an ankle of the angle in the AFO (AAAFO) of 90°, on a person who weighs 14 stone (196 pounds) with fixed pronation of the foot and excessive knee flexion during stance phase and a plantar flexion contracture, one is likely to conclude that the AFO was an unsuccessful intervention in controlling this patient’s gait when the actual conclusion should be the AFO design was inappropriate. The AFO would be inappropriate on the basis that 3-mm natural polypropylene would not be strong enough to control the gait deviations of a patient who weighed 14 stone/196 pounds, a lack of a lateral flange past the fifth met head would allow the foot to move off the footplate and offer no control to the forefoot abduction caused by pronation. The third rocker would not be blocked and the true length of gastrocnemius would not be accommodated in a 90° AFO, thus increasing knee flexion further and preventing knee extension at terminal stance.
There are wide ranging studies in the current literature which have studied a variety of outcomes with regards to the use of AFOs on children with CP, including spatiotemporal parameters, energy expenditure, joint kinetics and kinematics, sit-to-stand transfers and walking ability. A detailed description of the variation and efficacy of AFOs is beyond the scope of this article but is described widely within the published literature.20-23 There is variability regarding the efficacy of AFOs on the gait of children with CP; this may partially be due to inappropriate AFO design to match the presentation of the patient. The evidence base for the use of AFOs in children with CP has been repeatedly described as low quality.21-24
Previous papers22,25 have recommended reporting guidelines for AFO interventions to enable the quality of the AFO intervention to be more accurately assessed. Recommendations include: the movements prevented, assisted and permitted by the AFO; foot plate length and flexibility; trim-line position; materials; method of manufacture; and testing of mechanical stiffness of the AFO; concluding ‘Transparent reporting permits replication of the study, and makes it possible to understand the variables that may affect intervention outcomes’.25
The aim of this paper is to perform a systematic review on the current literature pertaining to studies on AFOs in children with CP, with emphasis on the detail of the design and material of the AFO offered in each paper. A secondary aim is to analyse the outcome measures used in each study. The authors recognise that there are numerous other essential aspects of reporting regarding AFO research, e.g. the shank vertical angle, the footwear combination, the tuning process and the physical presentation of the child; these have been described in the current literature25-29 and will not be detailed in this paper.
Methods
Data sources
This systematic review of databases was performed in March 2015. The following 14 databases were searched: Web of Science, Medline, PubMed, CINAHL Plus, EMBASE, SCOPUS, Rehabdata, PsycInfo, ERIC, Education Research Complete, Business Source Complete, IEEE, NIHR and CEA Registry The search used the following key words: ‘AFO’, ‘ankle foot orthoses’, ‘cerebral palsy’ and ‘CP’. No language restriction was applied to the search. Searches were adapted for each database and were completed between 10 and 20 March 2015.
Study selection
Inclusion/exclusion criteria
Two reviewers independently screened the search results.
Inclusion criteria:
- Papers which studied AFO/s on children (aged 18 years and under) with a primary diagnosis of CP.
- Studies which measured an outcome, excluding patient perception studies.
- Studies which were in English.
- Full studies which were located in a peer-reviewed journal.
Exclusion criteria:
- Expert opinion articles; letters to the editor; commentaries, abstracts and systematic reviews.
- Studies involving participants aged over 18 years.
- Studies which involved participants who did not have a diagnosis of CP.
Data extraction and methodological quality appraisal
One reviewer extracted data regarding the characteristics of the included studies, with the extracted data checked for accuracy and completeness by a second reviewer. For the extracted data checklist see Table 1.
Table 1.
Extraction data.
| AFO design | Choose response |
|---|---|
| Is the type of AFO described? | Type of AFO/Incomplete/- |
| Is the AFO bespoke or stock? | Bespoke/Stock/- |
| Is the AAAFO described? | Yes/- |
| Is the manufacturer of the AFO identified? | Complete/- |
| Are the trim lines of the ankle described? | Complete/Incomplete/- |
| Are the trim lines of the foot plate described? | Complete/Incomplete/- |
| Is the height of the AFO described? | Complete/Incomplete/- |
| Is the strapping system described? | Complete/Incomplete/- |
| Is there detail of the stiffness of the AFO in stance phase? | Complete/Incomplete/- |
| If hinges are stipulated are these described? | Complete/Incomplete/- |
| Is there a justification for choosing the AFO design? | Complete/Incomplete/- |
| AFO material | |
| Is the material described? | Material/- |
| Is the thickness of the material described? | Thickness/- |
| Is there a justification for choosing the material and thickness? | Complete/incomplete/- |
| Has stiffness testing been carried out? | Yes/- |
Results
The electronic database search identified 947 articles pertaining to the study of AFOs. Following the application of the inclusion criteria, 55 papers met the criteria imposed by this review. Appendix 1 outlines the extracted data from various included studies. See Table 2 for grouped data per question.
Table 2.
Data extraction grouped per question.
| | Data Extracted: | | | ----------------------------------------------------------------------------------------------------- | ----------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------- | | Is the type of AFO described? | See Fig. 1 | | Is the AFO bespoke or stock/off the shelf? | 32 papers reportedly used bespoke AFOs 1 paper reportedly used bespoke and stock 1 paper used stock 21 papers did not state | | Is the AAAFO described? | 15 papers described the AAAFO 10 papers gave incomplete details 30 Papers did not state | | Is the manufacturer of the AFOs described? | 6 papers detailed the manufacturer 1 paper gave incomplete details 48 papers did not state | | Are the trim lines of the ankle described? | 10 Papers detailed the trim lines at the ankle 7 papers gave incomplete details 38 papers did not state | | Is the full design of the footplate described, including length, stiffness and medio-lateral borders? | 0 papers gave a full description of the footplate 21 papers gave an incomplete description of the footplate 34 papers did not state any description of the footplate | | Is the height of the AFO described? | 14 papers described the height of the AFO 4 papers gave an incomplete description 37 papers did not describe the height of the AFO | | Is the strapping system described? | 9 papers described the strapping system 5 papers gave an incomplete description 31 papers did not describe the strapping system | | Is the stiffness of the AFO in the stance phase described? | 9 papers described the stiffness of the AFO in stance phase 6 papers gave an incomplete description 40 papers did not state | | If hinges are stipulated, are these described? | 9 papers described the hinges on the AFO 2 papers gave an incomplete description 21 papers did not state 23 papers were N/A | | Is the material described? | 24 papers described the material used 31 papers did not state the material used 20 papers used polypropylene 2 papers used copolymer 1 paper used homopolymer 1 paper used graphite 1 papers used carbon fibre 1 paper gave an incomplete description | | Is the thickness of the material described? | 40 papers did not state the material thickness 1 paper stated 6 mm 1 paper stated 5 mm 4 papers stated 4.8 mm 1 paper stated 4.5 mm 4 papers stated 4 mm 1 paper stated 3.2 mm 7 papers stated 3 mm 1 paper stated 2.4 mm | | Is there a justification for choosing the material and thickness? | 2 papers gave a justification for material and or thickness choice 1 paper gave an incomplete description 52 papers did not state | | Has stiffness testing been carried out? | 2 paper carried out stiffness testing 53 did not state | | What was the outcome measure of the study? | 25 papers measured lower limb kinetics and kinematics of gait and temporal spatial parameters 10 papers measured energy expenditure 5 papers measured standing balance 4 papers measured functional motor skills 2 papers measured sit to stand transfers 2 papers measured stair locomotion 2 papers measured trunk posture 2 papers measured EMG 3 papers measured knee extension 1 paper measured level walking 1 paper measured ankle function 1 paper measured skin tissue pressure mobility 1 paper measured ankle range of motion 1 paper measured hamstring length 1 paper measured functional balance 1 paper measured ambulation 1 paper measured static foot alignment 1 paper measured lower limb intersegmental co-ordination 2 paper measured gross motor function 1 paper measured pelvis, thorax and arm kinematics |
The main results of this review show that the most commonly tested AFO is a bespoke (58.2%), hinged AFO (21%). The AFO material most commonly used of those who stated material used (43.6%) was polypropylene (83.3%) in 3-mm thickness (n = 7). The outcome most commonly measured was lower limb kinetics, kinematics and temporal spatial parameters during gait (n = 25).
Only 3.6% of the papers reviewed carried out stiffness testing on the AFO intervention they used; 61.8% of papers failed to give any description of the footplate, the trim lines at the ankle (69%), the height of the AFO (67.3%), the material thickness (72.7%) and the ankle of the angle in the AFO (AAAFO) (54.5%).
Discussion
The research included within this study examined the effect of AFO use on a range of outcome measures in children with CP. As stated in previous reviews,21,22,25,30 there was considerable variety in both the level and quality of the details reported. The results show that none of the papers reviewed adequately described the design and material of the AFO being studied. In all of the papers reviewed, AFOs were the main intervention from which the outcome was measured. Thus, it is inconceivable that such a lack of detail on the main intervention should be provided. In many cases this lack of detail limits any assessment of intervention quality and the impact that this may have on the confidence of findings. This variability also means that it is not possible to analyse or pool the data in a structured way to conduct some sort of meta-analyses which can summarise results across studies to provide substantial evidence for treatment practices.
The paucity of detail regarding AFO design and justification in the current literature may be responsible for producing variation in reported outcome measures, e.g. temporal-spatial parameters,31,32 ankle kinematics32-34,35 and knee kinematics.36 Van Gestal et al reported ‘when reading (recent) literature, the researcher is often confronted with contradictions in reported effects of certain AFOs on gait’;37 however, this paper failed to report full details of the material used in all AFOs studied, the footplate design and flexibility, the material thickness, ankle trim lines and the AAAFO. Similarly, Davand et al reported ‘The importance of the choice of appropriate AFOs in improvements of standing and walking in these children are quite critical. When an orthotic is given correctly, the participant will perform activities of daily living (ADLs) better and more independently.’38 However, Dalvand et al failed to include the full details of the AFOs issued to their participants, including trim lines at the ankle, type of hinged used, strapping system, footplate design, stiffness of the material used and the justification of the chosen AFO design.38
Furthermore, there is a lack of standardisation for the terminology used to describe each type of AFO. Thus, there is no clear definition on what constitutes a ‘solid’ AFO. The term is often used to describe an AFO with trim lines anterior to the malleolus but made from a material which allows deformation at the ankle joint during gait. Others will use the term ‘solid’ to denote a rigid AFO with anterior trim lines and no movement at the ankle during stance phase.
Thus, stating that an AFO is ‘solid’ in design is not enough to determine its potential effects on gait or ensure that a study is reproducible and its outcomes correctly evaluated. Although the literature reports several different types of AFOs, it is often not clear which type of AFO is being used for the intervention. For example, five of the papers reviewed termed their AFO as ‘rigid’, six used the term ‘fixed’ and 19 used ‘solid’ (Fig. 1). Due to the aforementioned lack of standardisation of terminology, it is unclear whether these papers are all using the same style of AFO. Hinged AFOs (n = 20) were the most common intervention in the studies reviewed. It is critical to ensure that the length of gastrocnemius can be accommodated in a hinged AFO; a failure to do so will result in compensations at the knee and hip.26-29 Without sufficient details regarding the prescription and clinical reasoning for the provision of a hinged AFO, it is difficult to summarise its effectiveness.
Fig. 1.
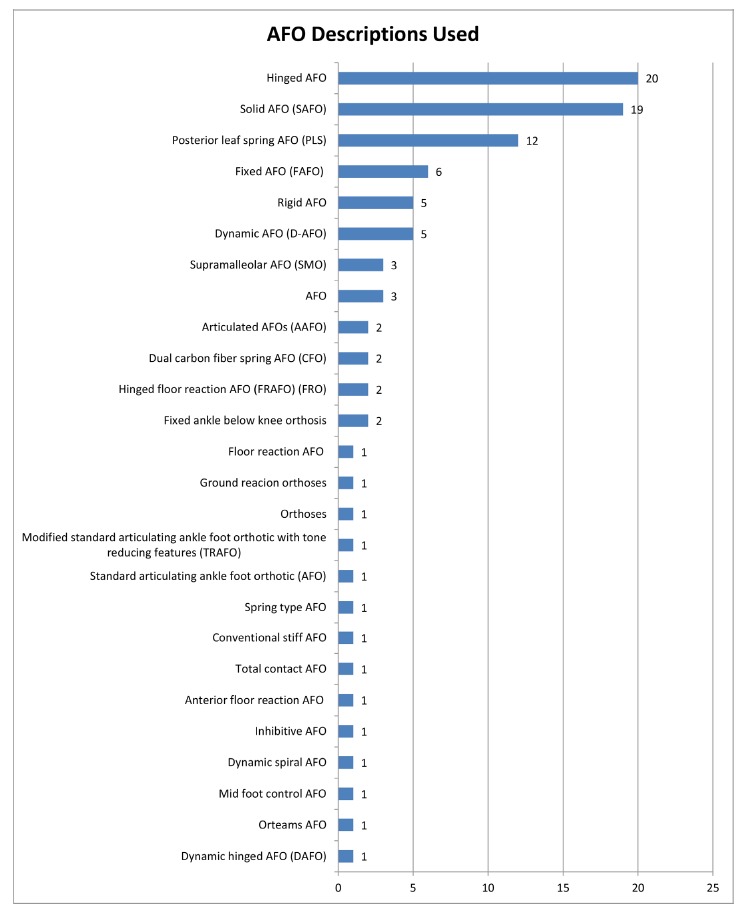
The type of ankle foot orthoses (AFO) design reported in each study.
Dursan et al,39 Olama et al,40 Kott and Held41 and Mossberg et al42 do not state which type of AFO has been used and offer no other details of the AFO design. This means that the results published are of little value. Partially, as the validity of the papers and repeatability are poor and therefore the results have limited clinical value, one is unable to draw conclusions from the results.
The 32 papers used bespoke AFOs and one paper used both stock/off-the-shelf and bespoke AFOs; however, 21 (38.2%) papers have not stated whether the AFOs were stock or bespoke. For this reason, it is difficult to surmise whether the AFO used fits the participant appropriately and whether fit issues could have had an effect on the results. Only six papers stated the manufacturer used for the AFO; thus, there is a possibility that the experience of the technician may have had an impact on AFO effectiveness.
Differences in the mechanical properties of the AFO can arise from small variations in AFO design such as trim-line position and choice of materials.25 A method of measuring the stiffness and neutral angle around the ankle and MTPJs has been demonstrated as clinically applicable.16,43 However, only two (3.6%) papers demonstrated the stiffness of the AFO during stance phase, which means that the control given by the AFO is only known within these two papers. Thus, whether the AFO had adequate control is unknown, potentially affecting the results of these studies.
The 31 (56.4%) papers did not state the material used in the AFO. Of the 24 papers which did state the material, the majority (83.3%) used polypropylene. However, when stating polypropylene, researchers did not given details on the type of polypropylene used, e.g. natural or homo polypropylene, both of which have different characteristics. Furthermore, 72.7% of researchers did not state material thickness. The current literature has indicated that both the material used and thickness have an effect on the rigidity and flexibility of the AFO; the fact that researchers are not stating this means the reader is unable to tell if the results of the study are from the AFO being an inappropriate material or thickness, or whether AFO intervention was unsuccessful. Of those papers who did state material thickness, the most common thickness used was 3 mm (n = 7). Only two papers justified the reasons for giving the AFO material and thickness.44,45
The 21 papers (38.2%) gave a partial description of the footplate design and 34 papers (61.8%) failed to give any description of the footplate design. None of the papers included within this review offered a full description of the footplate design. The height of the AFO was described by 14 papers (25.5%) with only ten papers (18.2%) fully describing the trim lines of the AFO at the ankle and six papers (10.9%) detailing a partial description of trim lines at the ankle. As trim lines have such a significant impact of the rigidity and function of an AFO, omitting the details of the trim lines of an AFO, means it is difficult to know the function of the AFO and how appropriate the design of the AFO was in trying to produce the desired outcome.
There was a failure in all studies reviewed to give a clinical justification for the AFO design used. Thus, the chosen AFO prescription and desired function is unclear. Gage46 reports the selection of the proper orthotic design should be based on an understanding of the primary gait deviations of the patient. Therefore, it is difficult to assess how the AFO design impacted the results, or whether the design was inappropriately chosen for the participant, and whether this had a detrimental effect on the results.
Only 15 (27.3%) papers detailed the AAAFO, the choice of which depends on clinical measures such as the passive and dynamic gastrocnemius muscle length and tri-planar foot stability. If there is severe spasticity or contracture in this muscle it must be accommodated within the AAAFO to avoid limiting maximum knee extension or compromising the tri-planar stability of the foot.47 If the passive gastrocnemius length is also reported in addition to the AAAFO, the reader can confirm that prescription is appropriate. Furthermore, if a paper is reporting on a hinged AFO which allows free dorsiflexion (one could refer free dorsiflexion to a hinge with no dorsiflexion stop) and such a device is being used on a participant with a plantar flexion contracture, the reader will be able to deduce that such a device will detrimentally effect knee extension and/ or foot position.
The CP consensus conference (the aim of which was to determine the evidence to support the efficacy of lower limb orthoses used for children with CP) in 1994 concluded that: ‘The existing body of literature on the effects of orthotic intervention in cerebral palsy is, for the most part, seriously scientifically and experimentally flawed’.24 Unfortunately, in terms of description of device used, the situation appears to have changed very little in the last 20 years.
A full analysis of the papers included in this systematic review is available in the appendix.48-85
Based on the systematic appraisal of the current literature, future studies should include the following recommendations:
- The material of the AFO used as an intervention in a research study should be detailed, including type, thickness and any reinforcements.
- The full design of the AFO should be described, including trim lines at the ankle, footplate design, length, medial and lateral flanges and flexibility, strapping arrangement and reinforcements.
- The stiffness of the AFO in stance phase should be described.
- The type of AFO used should be described and a justification of the choice of design should be detailed.
- The AAAFO should be detailed along with a justification of the chosen AAAFO.
Transparent reporting permits replication of the study and makes it possible to understand the variables that may affect intervention outcomes.25 It is therefore recommended that journals reviewing future research on AFOs should reject papers which do not include the full details of the AFO intervention as outlined above
Limitations
One of the perceived limitations of this study could be that it did not assign quality scores or rank studies, or look at the sample sizes or method outside of the materials and AFO design. With this in mind, one could argue that the scope of this study is limited, However, the reported results clearly indicate that there is a substantial lack of structured information within the published research papers which needs to be addressed.
Future research
Further research is needed on AFO prescription protocols. The AFO prescription process is largely empirical, resulting in confusing results regarding treatment efficacy. Development of prescription protocols will help ensure the design of AFOs in future research can be better compared and outcome measures validated, thus leading to improved clinical practice, based on evidence-based AFO provision. An agreed consensus on outcome measures will allow researchers to cross-reference research and enable validated meta-analyses to be performed. Terminology used to describe AFOs needs to be standardised to ensure studies can be reproduced and readily compared and evaluated.
Appendix
An appendix showing the data extracted from all papers is available online with this paper.
Compliance with Ethical Standards
Funding Statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Ethical Statement
No funding was received for this study.
References
- 1.Armand S, Watelain E, Mercier M, Lensel G, Lepoutre FX. Identification and classification of toe-walkers based on ankle kinematics, using a data-mining method. Gait Posture 2006;23:240-248. [DOI] [PubMed] [Google Scholar]
- 2.No authors listed. Prevalence and characteristics of children with cerebral palsy in Europe. Dev Med Child Neurol 2002;44:633-640. [PubMed] [Google Scholar]
- 3.Gage JR, Novacheck TF. An update on the treatment of gait problems in cerebral palsy. J Pediatr Orthop B 2001;10:265-274. [PubMed] [Google Scholar]
- 4.No authors listed. International Organization for Standardization. ISO 8549-1:1989 prosthetics and orthotics – vocabulary. General terms for external limb prostheses and external orthoses. https://www.iso.org/standard/15800.html (date last accessed 15 May 2017).
- 5.British Standard. BS7313. Prosthetics and orthotics. Terminology. Glossary of general terms relating to external limb prostheses and external orthoses. London: British Standards Institute; 1990. [Google Scholar]
- 6.Michael JW. Lower limb orthoses. In: Hsu JD, Michael JW, Fisk JR, eds. AAOS Atlas of orthoses and assistive devices. Fourth ed. Philadelphia, PA: Mosby Elsevier, 2008:343-355. [Google Scholar]
- 7.Singerman R, Hoy DJ, Mansour JM. Design changes in ankle foot orthoses intended to alter stiffness also alters orthosis kinematics. J Prosthet Orthot 1999;11:48-56. [Google Scholar]
- 8.Condie DN, Meadows CB. Some biomechanical considerations in the design of ankle-foot orthoses. Orthot Prosthet 1977;31:45-52. [Google Scholar]
- 9.DeToro WW. Plantarflexion resistance of selected ankle-foot orthoses: A pilot study of commonly prescribed prefabricated and custom-moulded alternatives. J Prosthet Orthot 2001;13:39-44. [Google Scholar]
- 10.Golay W, Lunsford T, Lunsford BR, Greenfield J. The effect of malleolar prominence on polypropylene AFO rigidity and buckling. J Prosthet Orthot 1989;1:231-242. [Google Scholar]
- 11.Nagaya M. Shoehorn-type ankle-foot orthoses: prediction of flexibility. Arch Phys Med Rehabil 1997;78:82-84. [DOI] [PubMed] [Google Scholar]
- 12.Novacheck TF, Beattie CB, Rozumalski A, Gent G, Kroll G. Quantifying the spring-like properties of ankle-foot orthoses (AFOs). J Prosthet Orthot 2007;19:98-103. [Google Scholar]
- 13.Polliack AA, Swanson C, Landsberger SE, McNeal DR. Development of a testing apparatus for structural stiffness evaluation of ankle-foot orthoses. J Prosthet Orthot 2001;13:74-82. [Google Scholar]
- 14.Lunsford TR, Contoyannis B. Materials Science. In: Hsu JD, Michael JW, Fisk JR, eds. AAOS Atlas of orthoses and assistive devices. Fourth ed. Philadelphia: Mosby Elsevier, 2008:15-52. [Google Scholar]
- 15.Wilson H, Haideri N, Song K, Telford D. Ankle-foot orthoses for preambulatory children with spastic diplegia. J Pediatr Orthop 1997;17:370-376. [PubMed] [Google Scholar]
- 16.Bregman DJJ, Rozumalski A, Koops D, et al. A new method for evaluating ankle foot orthosis characteristics: BRUCE. Gait Posture 2009;30:144-149. [DOI] [PubMed] [Google Scholar]
- 17.Sumiya T, Suzuki Y, Kasahara T. Stiffness control in posterior-type plastic ankle-foot orthoses: effect of ankle trimline. Part 1: A device for measuring ankle moment. Prosthet Orthot Int 1996;20:129-131. [DOI] [PubMed] [Google Scholar]
- 18.Major RE, Hewart PJ, MacDonald AM. A new structural concept in moulded fixed ankle foot orthoses and comparison of the bending stiffness of four constructions. Prosthet Orthot Int 2004;28:44-48. [DOI] [PubMed] [Google Scholar]
- 19.Ounpuu S, Bell KJ, Davis RB III, DeLuca PA. An evaluation of the posterior leaf spring orthosis using joint kinematics and kinetics. J Pediatr Orthop 1996;16: 378-384. [DOI] [PubMed] [Google Scholar]
- 20.Condie DN, Meadows CB. Report on a consensus conference on the lower limb orthotic management of cerebral palsy. Copenhagen: International Society for Prosthetics and Orthotics; 1995. [Google Scholar]
- 21.Morris C. A review of the efficacy of lower-limb orthoses used for cerebral palsy. Dev Med Child Neurol 2002;44:205-211. [DOI] [PubMed] [Google Scholar]
- 22.Bowers R, Ross K. A review of the effectiveness of lower limb orthoses used in cerebral palsy. In: Morris C, Condie D, eds. Recent developments in healthcare for cerebral palsy: implications and opportunities for orthotics. Copenhagen: International Society for Prosthetics and Orthotics, 2009:235-297. [Google Scholar]
- 23.Ries AJ, Novacheck TF, Schwartz MH. The efficacy of ankle-foot orthoses on improving the gait of children with diplegic cerebral palsy: a multiple outcome analysis. PM R 2015;7:922-929. [DOI] [PubMed] [Google Scholar]
- 24.Morris C, Condie D. Recent developments in healthcare for cerebral palsy: Implications and opportunities for orthotics. Copenhagen: International Society for Prosthetics and Orthotics, 2009. [Google Scholar]
- 25.Ridgewell E, Dobson F, Bach T and Baker R. A systematic review to determine best practice reporting guidelines for AFO interventions in studies involving children with cerebral palsy. Prosthet Orthot Int 2010;34:129-145 [DOI] [PubMed] [Google Scholar]
- 26.Eddison N, Chockalingam N. The effect of tuning ankle foot orthoses-footwear combination on the gait parameters of children with cerebral palsy. Prosthet Orthot Int 2013;37:95-107. [DOI] [PubMed] [Google Scholar]
- 27.Owen E. Tuning of ankle foot orthosis footwear combinations for children with cerebral palsy, spina bifida and other conditions. In: Proceedings of the European Society of Movement Analysis in Adults and Children. (ESMAC) seminars, Warsaw, Poland, 23-25 September 2004. [Google Scholar]
- 28.Owen E. Shank angle to floor measures and tuning of ankle foot orthosis footwear combinations for children with cerebral palsy, spina bifida and other conditions. MSc Thesis. Glasgow: University of Strathclyde, 2004. [Google Scholar]
- 29.Owen E, Bowers RJ, Meadows CB. Tuning of AFO-footwear combinations for neurological disorders. In: International Society for Prosthetics and Orthotics (ISPO) 11th world congress. Hong Kong, China: ISPO, 2004:278-279. [Google Scholar]
- 30.Figueiredo EM, Ferreira GB, Maia Moreira RC, Kirkwood RN, Fetters L. Efficacy of ankle-foot orthoses on gait of children with cerebral palsy: systematic review of literature. Pediatr Phys Ther 2008;20:207-223. [DOI] [PubMed] [Google Scholar]
- 31.Brunner R, Meier G, Ruepp T. Comparison of a stiff and a spring-type ankle-foot orthosis to improve gait in spastic hemiplegic children. J Pediatr Orthop 1998;18:719-726. [PubMed] [Google Scholar]
- 32.Buckon CE, Thomas SS, Jakobson-Huston S, et al. Comparison of three ankle-foot orthosis configurations for children with spastic diplegia. Dev Med Child Neurol 2004;46:590-598. [DOI] [PubMed] [Google Scholar]
- 33.Rethlefsen S, Kay R, Dennis S, Forstein M, Tolo V. The effects of fixed and articulated ankle-foot orthoses on gait patterns in subjects with cerebral palsy. J Pediatr Orthop 1999;19:470-474. [DOI] [PubMed] [Google Scholar]
- 34.Desloovere K, Molenaers G, Van Gestel L, et al. How can push-off be preserved during use of an ankle foot orthosis in children with hemiplegia? A prospective controlled study. Gait Posture 2006;24:142-151. [DOI] [PubMed] [Google Scholar]
- 35.Radtka SA, Skinner SR, Dixon DM, Johanson ME. A comparison of gait with solid, dynamic, and no ankle-foot orthoses in children with spastic cerebral palsy. Phys Ther 1997;77:395-409. [DOI] [PubMed] [Google Scholar]
- 36.Buckon CE, Thomas SS, Jakobson-Huston S, Sussman M, Aiona M. Comparison of three ankle-foot orthosis configurations for children with spastic hemiplegia. Dev Med Child Neurol 2001;43:371-378. [DOI] [PubMed] [Google Scholar]
- 37.Van Gestel L, Molenaers G, Huenaerts C, Seyler J, Desloovere K. Effect of dynamic orthoses on gait: a retrospective control study in children with hemiplegia. Dev Med Child Neurol 2008;50:63-67. [DOI] [PubMed] [Google Scholar]
- 38.Dalvand H, Dehghan L, Feizi A, Hosseini SA, Amirsalari S. The impacts of hinged and solid ankle-foot orthoses on standing and walking in children with spastic diplegia. Iran J Child Neurol 2013;7:12-19. [PMC free article] [PubMed] [Google Scholar]
- 39.Dursun E, Dursun N, Alican D. Ankle-foot orthoses: effect on gait in children with cerebral palsy. Disabil Rehabil 2002;24:345-347. [DOI] [PubMed] [Google Scholar]
- 40.Olama KA, El-Din SMN, Ibrahem MB. Role of three side support ankle–foot orthosis in improving the balance in children with spastic diplegic cerebral palsy. Egypt J Med Hum Genet 2013;14:77-85. [Google Scholar]
- 41.Kott KM, Held SL. Effects of orthoses on upright functional skills of children and adolescents with cerebral palsy. Pediatr Phys Ther 2002;14:199-207. [DOI] [PubMed] [Google Scholar]
- 42.Mossberg KA, Linton KA, Friske K. Ankle-foot orthoses: effect on energy expenditure of gait in spastic diplegic children. Arch Phys Med Rehabil 1990;71:490-494. [PubMed] [Google Scholar]
- 43.Papi E, Maclean J, Bowers RJ, Solomonidis SE. Determination of loads carried by polypropylene ankle-foot orthoses: A preliminary study. Proc Inst Mech Eng H 2015;229:40-51 [DOI] [PubMed] [Google Scholar]
- 44.Kerkum YL, Harlaar J, Buizer AI, et al. Optimising Ankle Foot Orthoses for children with cerebral palsy walking with excessive knee flexion to improve their mobility and participation; protocol of the AFO-CP study. BMC Pediatr 2013;13:17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Jagadamma KC, Coutts FJ, Mercer TH, et al. Optimising the effects of rigid ankle foot orthoses on the gait of children with cerebral palsy (CP)–an exploratory trial. Disabil Rehabil Assist Technol 2014;10:445-451. [DOI] [PubMed] [Google Scholar]
- 46.Gage JR. Gait analysis in cerebral palsy. London: Mac Keith Press, 1991. [Google Scholar]
- 47.Meadows B, Bowers RJ, Owen E. Biomechanics of the hip, knee, and ankle. In: Hsu JD, Michael JW, Fisk JR, eds. AAOS Atlas of orthoses and assistive devices. Fourth ed. Philadelphia: Mosby Elsevier, 2008:299-310. [Google Scholar]
- 48.Rosenthal RK, Deutsch SD, Miller W, Schumann W, Hall JE. A fixed ankle below the knee orthosis fo the management of Genu recurvatum in spastic cerebral palsy. J Bone Joint Surg [Am] 1975;57-A:545-547. [PubMed] [Google Scholar]
- 49.Simon SR, Deutsch SD, Nuzzo RM, et al. Genu recurvatum in spastic cerebral palsy. Report on findings by gait analysis. J Bone Joint Surg [Am] 1978;60-A:882-894. [PubMed] [Google Scholar]
- 50.Harrington ED, Lin RS, Gage JR. Use of the anterior floor reaction orthosis in patients with cerebral palsy. Orthotics and Prosthetics 1984;37:34-42. [Google Scholar]
- 51.Harris SR, Riffle K. Effects of inhibitive ankle-foot orthoses on standing balance in a child with cerebral palsy. A single-subject design. Phys Ther 1986;66:663-667. [DOI] [PubMed] [Google Scholar]
- 52.Middleton EA, Hurley GRB, McIlwain JS. The role of rigid and hinged polypropylene ankle-foot-orthoses in the management of cerebral palsy: a case study. Prosthet Orthot Int 1988;12:129-135. [DOI] [PubMed] [Google Scholar]
- 53.Butler PB, Thompson N, Major RE. Improvement in walking performance of children with cerebral palsy: preliminary results. Dev Med Child Neurol 1992;34:567-576. [DOI] [PubMed] [Google Scholar]
- 54.Hainsworth F, Harrison MJ, Sheldon TA, Roussounis SH. A preliminary evaluation of ankle orthoses in the management of children with cerebral palsy. Dev Med Child Neurol 1997;39:243-247. [DOI] [PubMed] [Google Scholar]
- 55.Carlson WE, Vaughan CL, Damiano DL, Abel MF. Orthotic management of gait in spastic diplegia. Am J Phys Med Rehabil 1997;76:219-225. [DOI] [PubMed] [Google Scholar]
- 56.Abel MF, Juhl GA, Vaughan CL, Damiano DL. Gait assessment of fixed ankle-foot orthoses in children with spastic diplegia. Arch Phys Med Rehabil 1998;79:126-133. [DOI] [PubMed] [Google Scholar]
- 57.Burtner PA, Woollacott MH, Qualls C. Stance balance control with orthoses in a group of children with spastic cerebral palsy. Dev Med Child Neurol 1999;41: 748-757. [DOI] [PubMed] [Google Scholar]
- 58.Suzuki N, Shinohara T, Kimizuka M, Yamaguchi K, Mita K. Energy expenditure of diplegic ambulation using flexible plastic ankle foot orthoses. Bull Hosp Jt Dis 2000;59:76-80. [PubMed] [Google Scholar]
- 59.Crenshaw S, Herzog R, Castagno P, et al. The efficacy of tone-reducing features in orthotics on the gait of children with spastic diplegic cerebral palsy. J Pediatr Orthop 2000;20:210-216. [PubMed] [Google Scholar]
- 60.Bill M, McIntosh R, Myers P. A series of case studies on the effect of a midfoot control ankle foot orthosis in the prevention of unresolved pressure areas in children with cerebral palsy. Prosthet Orthot Int 2001;25:246-250. [DOI] [PubMed] [Google Scholar]
- 61.Maltais D, Bar-Or O, Galea V, Pierrynowski M. Use of orthoses lowers the O(2) cost of walking in children with spastic cerebral palsy. Med Sci Sports Exerc 2001;33:320-325. [DOI] [PubMed] [Google Scholar]
- 62.Beals RB. Resident’s forum. The possible effects of solid ankle-foot orthoses on trunk posture in the nonambulatory cerebral palsy population: A preliminary evaluation. J Prosthet Orthot 2001;13:34-38. [Google Scholar]
- 63.White H, Jenkins J, Neace WP, Tylkowski C, Walker J. Clinically prescribed orthoses demonstrate an increase in velocity of gait in children with cerebral palsy: a retrospective study. Dev Med Child Neurol 2002;44:227-232. [DOI] [PubMed] [Google Scholar]
- 64.Romkes J, Brunner R. Comparison of a dynamic and a hinged ankle-foot orthosis by gait analysis in patients with hemiplegic cerebral palsy. Gait Posture 2002;15: 18-24. [DOI] [PubMed] [Google Scholar]
- 65.Thompson NS, Taylor TC, McCarthy KR, Cosgrove AP, Baker RJ. Effect of a rigid ankle-foot orthosis on hamstring length in children with hemiplegia. Dev Med Child Neurol 2002;44:51-57. [DOI] [PubMed] [Google Scholar]
- 66.Sienko Thomas S, Buckon CE, Jakobson-Huston S, Sussman MD, Aiona MD. Stair locomotion in children with spastic hemiplegia: the impact of three different ankle foot orthosis (AFOs) configurations. Gait Posture 2002;16:180-187. [DOI] [PubMed] [Google Scholar]
- 67.Smiley SJ, Jacobsen FS, Mielke C, et al. A comparison of the effects of solid, articulated, and posterior leaf-spring ankle-foot orthoses and shoes alone on gait and energy expenditure in children with spastic diplegic cerebral palsy. Orthopedics 2002;25:411-415. [DOI] [PubMed] [Google Scholar]
- 68.Wesdock KA, Edge AM. Effects of wedged shoes and ankle-foot orthoses on standing balance and knee extension in children with cerebral palsy who crouch. Pediatr Phys Ther 2003;15:221-231. [DOI] [PubMed] [Google Scholar]
- 69.Park ES, Park CI, Chang HJ, Choi JE, Lee DS. The effect of hinged ankle-foot orthoses on sit-to-stand transfer in children with spastic cerebral palsy. Arch Phys Med Rehabil 2004;85:2053-2057. [DOI] [PubMed] [Google Scholar]
- 70.Radtka SA, Skinner SR, Johanson ME. A comparison of gait with solid and hinged ankle-foot orthoses in children with spastic diplegic cerebral palsy. Gait Posture 2005;21:303-310. [DOI] [PubMed] [Google Scholar]
- 71.Lam WK, Leong JCY, Li YH, Hu Y, Lu WW. Biomechanical and electromyographic evaluation of ankle foot orthosis and dynamic ankle foot orthosis in spastic cerebral palsy. Gait Posture 2005;22:189-197. [DOI] [PubMed] [Google Scholar]
- 72.Romkes J, Hell AK, Brunner R. Changes in muscle activity in children with hemiplegic cerebral palsy while walking with and without ankle-foot orthoses. Gait Posture 2006;24:467-474. [DOI] [PubMed] [Google Scholar]
- 73.Bjornson KF, Schmale GA, Adamczyk-Foster A, McLaughlin J. The effect of dynamic ankle foot orthoses on function in children with cerebral palsy. J Pediatr Orthop 2006;26:773-776. [DOI] [PubMed] [Google Scholar]
- 74.Lucareli PR, Lima MdeO, Lucarelli JG, Lima FP. Changes in joint kinematics in children with cerebral palsy while walking with and without a floor reaction ankle-foot orthosis. Clinics (Sao Paulo) 2007;62:63-68. [DOI] [PubMed] [Google Scholar]
- 75.Balaban B, Yasar E, Dal U, et al. The effect of hinged ankle-foot orthosis on gait and energy expenditure in spastic hemiplegic cerebral palsy. Disabil Rehabil 2007;29:139-144. [DOI] [PubMed] [Google Scholar]
- 76.Butler PB, Farmer SE, Stewart C, Jones PW, Forward M. The effect of fixed ankle foot orthoses in children with cerebral palsy. Disabil Rehabil Assist Technol 2007;2:51-58. [DOI] [PubMed] [Google Scholar]
- 77.Westberry DE, Davids JR, Shaver JC, et al. Impact of ankle-foot orthoses on static foot alignment in children with cerebral palsy. J Bone Joint Surg [Am] 2007;89-A:806-813. [DOI] [PubMed] [Google Scholar]
- 78.Brehm MA, Harlaar J, Schwartz M. Effect of ankle-foot orthoses on walking efficiency and gait in children with cerebral palsy. J Rehabil Med 2008;40:529-534. [DOI] [PubMed] [Google Scholar]
- 79.Jagadamma KC, Coutts FJ, Mercer HL, et al. Effects of tuning of ankle foot orthoses-footwear combination using wedges on stance phase knee hyperextension in children with cerebral palsy - preliminary results. Disabil Rehabil Assist Technol 2009;4:406-413. [DOI] [PubMed] [Google Scholar]
- 80.Rogozinski BM, Davids JR, Davis RB III, Jameson GG, Blackhurst DW. The efficacy of the floor-reaction ankle-foot orthosis in children with cerebral palsy. J Bone Joint Surg [Am] 2009;91-A:2440-2447. [DOI] [PubMed] [Google Scholar]
- 81.Rha DW, Kim DJ, Park ES. Effect of hinged ankle-foot orthoses on standing balance control in children with bilateral spastic cerebral palsy. Yonsei Med J 2010;51:746-752. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Degelean M, De Borre L, Salvia P, et al. Effect of ankle-foot orthoses on trunk sway and lower limb intersegmental coordination in children with bilateral cerebral palsy. J Pediatr Rehabil Med 2012;5:171-179. [DOI] [PubMed] [Google Scholar]
- 83.Bennett BC, Russell SD, Abel MF. The effects of ankle foot orthoses on energy recovery and work during gait in children with cerebral palsy. Clin Biomech (Bristol, Avon) 2012;27:287-291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Liu XC, Embrey D, Tassone C, et al. Foot and ankle joint movements inside orthoses for children with spastic CP. J Orthop Res 2014;32:531-536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Schweizer K, Brunner R, Romkes J. Upper body movements in children with hemiplegic cerebral palsy walking with and without an ankle-foot orthosis. Clin Biomech (Bristol, Avon) 2014;29:387-394. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.