Eunice Kennedy Shriver National Institute of Child Health and Human Development (original) (raw)
About Menstruation
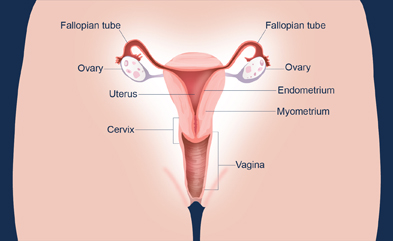
Menstruation (pronounced men-stroo-EY-shuhn) is normal discharge of blood and tissue from the uterine lining through the vagina (see diagram) that occurs as part of a woman's monthly menstrual cycle. Menstruation occurs between menarche (pronounced muh-NAHR-kee), a girl's first period, and menopause, when menstrual cycles end.1 The average menstruation time in normally menstruating women is about 5 days.2 In the United States, most girls start menstruating shortly after 12 years of age.3
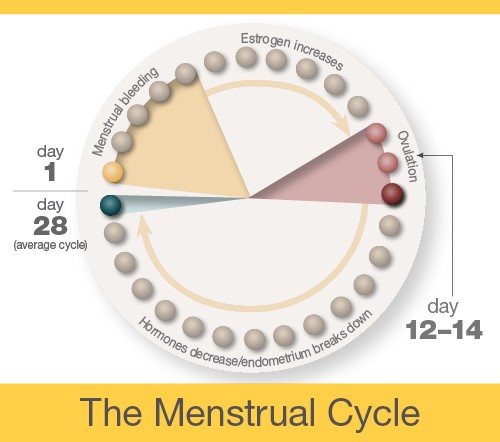
The menstrual cycle is the monthly process in which female hormones stimulate an ovary to release an egg, thicken the lining of the uterus to support a pregnancy, and then cause the uterus to shed this lining (through menstruation) if there is no pregnancy. The average menstrual cycle is 28 days, but this varies between women and from month to month. In teens, the menstrual cycle can range from 21 to 45 days, but for most women, it is 21 to 35 days.3
Day 1
The first day of bleeding is considered the first day of the menstrual cycle. After bleeding ends, usually around day 5, levels of the hormone estrogen begin to rise. The rise in estrogen causes the lining of the uterus to thicken as it prepares to hold a fertilized egg. At the same time, the changes in hormone levels cause follicles (the sacs in the ovary that contain eggs) to grow and mature, in preparation for one follicle to go through ovulation.
Ovulation
Around day 12 to 14 in an average 28-day cycle, the egg is released from a follicle on the ovary in a process called ovulation (pronounced ov-yu-LAY-shuhn). Ovulation can occur anywhere between 10 and 21 days after the first day of a woman's menstrual cycle. A woman can tell when she has begun ovulating using several methods, including at-home tests that measure levels of luteinizing hormone (LH) in the urine and keeping track of her body temperature, which typically rises slightly at ovulation. At mid-cycle, some women experience pain on one side of their pelvic area; this pain is called "Mittelschmerz"4 (meaning "middle pain," because it occurs in the middle of the cycle) and may be a signal of ovulation.
If a pregnancy does not occur, decreasing hormone levels signal for the lining of the uterus, called the endometrium, to be shed during menstruation.
The endometrium builds up and breaks down during the menstrual cycle. The endometrium is thickest halfway through the 28-day cycle. Then, if there is no pregnancy, it breaks down. This breakdown causes the bleeding of the menstrual phase. This diagram illustrates an average 28-day cycle.
Fertilization
After ovulation, the egg moves down the fallopian tube. The sperm can fertilize the egg at this point. After the sperm is ejaculated into the vagina, it moves into the cervix and through the uterus into the fallopian tube. Sperm can live up to 5 days in a woman's body.
If fertilization occurs, the newly formed embryo travels through the fallopian tube into the uterus, where it implants in the wall of the uterus. If fertilization does not occur, the egg naturally breaks down, and the uterine wall is lost in the form of menstrual bleeding.
Implantation
The embryo must successfully implant into the thickened wall of the uterus for the pregnancy to occur. The embryo first attaches to the wall of the uterus around 5 or 6 days after ovulation. It becomes more firmly implanted between 6 and 12 days after ovulation. Implantation causes a release of hCG—a hormone that signals the body to change to support the pregnancy. This hormone is what a pregnancy test detects.
Citations
- Sweet, M. G., Schmidt-Dalton, T. A., Weiss, P. M., & Madsen, K. P. (2012). Evaluation and management of abnormal uterine bleeding in premenopausal women. American Family Physician , 85, 35–43.
- Dasharathy, S. S., Mumford, S. L., Pollack, A. Z., Perkins, N. J., Mattison, D. R., Wactawski-Wende, J., & Schisterman, E. F. (2012). Menstrual bleeding patterns among regularly menstruating women. American Journal of Epidemiology, 175, 536–545.
- McDowell, M. A., Brody, D. J., & Hughes, J.P. (2007). Has age at menarche changed? Results from the National Health and Nutrition Examination Survey (NHANES) 1999-2004. Journal of Adolescent Health, 40, 227–231.
- Krohn, P. L. (1949). Intermenstrual pain (the "Mittelschmerz") and the time of ovulation. British Medical Journal, 1(4609), 803–805. Retrieved September 27, 2016, from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2049988/?page=1
What are the symptoms of menstruation?
The primary sign of menstruation is bleeding from the vagina. Additional symptoms include:
- Abdominal or pelvic cramping
- Lower back pain
- Bloating and sore breasts
- Food cravings
- Mood swings and irritability
- Headache
- Fatigue
What are menstrual irregularities?
For most women, a normal menstrual cycle ranges from 21 to 35 days.1 However, 14% to 25% of women have irregular menstrual cycles, meaning the cycles are shorter or longer than normal; are heavier or lighter than normal; or are experienced with other problems, like abdominal cramps.2 Irregular cycles can be ovulatory, meaning that ovulation occurs, or anovulatory, meaning ovulation does not occur.
The most common menstrual irregularities include:
- Amenorrhea (pronounced ey-men-uh-REE-uh) or absent menstrual periods:3,4,5,6 When a woman does not get her period by age 16, or when she stops getting her period for at least 3 months and is not pregnant.
- Oligomenorrhea (pronounced ol-i-goh-men-uh-REE-uh) or infrequent menstrual periods: Periods that occur more than 35 days apart.4
- Menorrhagia (pronounced men-uh-REY-jee-uh) or heavy menstrual periods:3,4,7 Also called excessive bleeding. Although anovulatory bleeding and menorrhagia are sometimes grouped together, they do not have the same cause and require different diagnostic testing.7
- Prolonged menstrual bleeding: Bleeding that exceeds 8 days in duration on a regular basis.4
- Dysmenorrhea (pronounced dis-men-uh-REE-uh): Painful periods that may include severe menstrual cramps.8
Additional menstrual irregularities include:
- Polymenorrhea (pronounced pol-ee-men-uh-REE-uh): Frequent menstrual periods occurring less than 21 days apart4
- Irregular menstrual periods with a cycle-to-cycle variation of more than 20 days4
- Shortened menstrual bleeding of less than 2 days in duration4
- Intermenstrual bleeding: Episodes of bleeding that occur between periods, also known as spotting4
Citations
- American College of Obstetricians and Gynecologists (ACOG). (2012). FAQ: Abnormal uterine bleeding. Retrieved on May 24, 2016, from http://www.acog.org/Patients/FAQs/Abnormal-Uterine-Bleeding
 (PDF 464 KB)
(PDF 464 KB) - Whitaker, L., & Critchley, H. O. D. (2016). Abnormal uterine bleeding. Best Practice & Research Clinical Obstetrics & Gynaecology, 34, 54–65. Retrieved June 23, 2016, from http://www.sciencedirect.com/science/article/pii/S1521693415002266
- Sweet, M. G., Schmidt-Dalton, T. A., Weiss, P. M., & Madsen, K. P. (2012). Evaluation and management of abnormal uterine bleeding in premenopausal women. American Family Physician , 85, 35–43.
- Munro, M. G., Critchley, H. O., & Fraser, I. S. (2012). The FIGO systems for nomenclature and classification of causes of abnormal uterine bleeding in the reproductive years: Who needs them? American Journal of Obstetrics and Gynecology, 207(4), 259–265.
- Master-Hunter, T., & Heiman, D. L. (2006). Amenorrhea: Evaluation and treatment. American Family Physician , 73, 1374–1382.
- Practice Committee of the American Society for Reproductive Medicine. (2008). Current evaluation of amenorrhea. Fertility and Sterility , 90, S219–S225. doi:10.1016/j.fertnstert.2008.08.038.
- Apgar, B. S., Kaufman, A. H., George-Nwogu, U., & Kittendorf, A. (2007). Treatment of menorrhagia. American Family Physician , 75, 1813–1819.
- French, L. (2005). Dysmenorrhea. American Family Physician , 71, 285–291.
How many women are affected by menstrual irregularities?
Menstrual irregularities occur in an estimated 14% to 25% of women of childbearing age.1
Estimates of the number of women with menstrual irregularities may differ by the cause or nature of the irregularity. For example, if a woman experiences severe cramps, she might be included in the tally of women with endometriosis rather than in the tally of women with menstrual irregularities.
Citations
- Whitaker, L., & Critchley, H. O. D. (2016). Abnormal uterine bleeding. Best Practice & Research Clinical Obstetrics & Gynaecology, 34, 54–65. Retrieved December 2, 2016, from http://www.sciencedirect.com/science/article/pii/S1521693415002266 .
What causes menstrual irregularities?
Menstrual irregularities can have a variety of causes, including pregnancy, hormonal imbalances, infections, diseases, trauma, and certain medications.1,2,3,4,5,6
Causes of irregular periods (generally light) include:2
 Perimenopause (generally in the late 40s and early 50s)
Perimenopause (generally in the late 40s and early 50s)- Primary ovarian insufficiency (POI)
- Eating disorders (anorexia nervosa or bulimia)
- Excessive exercise
- Thyroid dysfunction (too much or too little thyroid hormone)
- Elevated levels of the hormone prolactin, which is made by the pituitary gland to help the body produce milk
- Uncontrolled diabetes
- Cushing's syndrome (elevated levels of the hormone cortisol, used in the body's response to stress)
- Late-onset congenital adrenal hyperplasia (problem with the adrenal gland)
- Hormonal birth control (birth control pills, injections, or implants)
- Hormone-containing intrauterine devices (IUDs)
- Scarring within the uterine cavity (Asherman's syndrome)
- Medications, such as those to treat epilepsy or mental health problems
Common causes of heavy or prolonged menstrual bleeding include:2,7
- Adolescence (during which cycles may not be associated with ovulation)
- Polycystic ovary syndrome (PCOS) (bleeding irregular but heavy)
- Uterine fibroids (benign growths of uterine muscle)
- Endometrial polyps (benign overgrowth of the lining of the uterus)
- Adenomyosis (the presence of uterine lining in the wall of the uterus)
- Nonhormonal IUDs
- Bleeding disorders, such as leukemia, platelet disorders, clotting factor deficiencies, or (less common) von Willebrand disease
- Pregnancy complications (miscarriage)
Common causes of dysmenorrhea (menstrual pain) include:6,9
- Endometriosis (uterine lining grows outside the uterus)
- Uterine abnormalities (fibroids or adenomyosis)
- IUDs
- Pelvic scarring due to sexually transmitted infections, such as chlamydia or gonorrhea
- Heavy menstrual flow
Citations
- American College of Obstetricians and Gynecologists (ACOG). (2012). FAQ: Abnormal uterine bleeding. Retrieved on May 24, 2016, from http://www.acog.org/Patients/FAQs/Abnormal-Uterine-Bleeding (PDF 464 KB)
- Sweet, M. G., Schmidt-Dalton, T. A., Weiss, P. M., & Madsen, K. P. (2012). Evaluation and management of abnormal uterine bleeding in premenopausal women. American Family Physician , 85, 35–43.
- Master-Hunter, T., & Heiman, D. L. (2006). Amenorrhea: Evaluation and treatment. American Family Physician , 73, 1374–1382.
- Apgar, B. S., Kaufman, A. H., George-Nwogu, U., & Kittendorf, A. (2007). Treatment of menorrhagia. American Family Physician , 75, 1813–1819.
- Practice Committee of the American Society for Reproductive Medicine. (2008). Current evaluation of amenorrhea [Review]. Fertility and Sterility , 90, S219–S225.
- French, L. (2005). Dysmenorrhea. American Family Physician , 71, 285–291.
- Godfrey, E. M., Folger, S. G., Jeng, G., Jamieson, D. J., & Curtis, K. M. (2013). Treatment of bleeding irregularities in women with copper-containing IUDs: A systematic review. Contraception, 87(5), 549–566. Retrieved August 2, 2016, from http://www.contraceptionjournal.org/article/S0010-7824(12)00816-5/abstract
- Centers for Disease Control and Prevention. (2016). Chlamydia—CDC fact sheet. Retrieved on August 2, 2016, from http://www.cdc.gov/std/chlamydia/stdfact-chlamydia.htm
- American College of Obstetricians and Gynecologists. (2016). FAQ: Gonorrhea, chlamydia, and syphilis. Retrieved on August 2, 2016, from http://www.acog.org/Patients/FAQs/Gonorrhea-Chlamydia-and-Syphilis
How do health care providers diagnose menstrual irregularities?
A health care provider diagnoses menstrual irregularities using a combination of the following:1,2,3,4,5
- Medical history
- Physical examination
- Blood tests
- Ultrasound examination
- Endometrial biopsy—a small sample of the uterus's endometrial lining is taken to be examined under a microscope
- Hysteroscopy—a diagnostic scope that allows a health care provider to examine the inside of the uterus, typically done as an outpatient procedure
- Saline infusion sonohysterography—ultrasound imaging of the uterine cavity while it is filled with sterile saline solution
- Transvaginal ultrasonography—ultrasound imaging of the pelvic organs, including the ovaries and uterus, using an ultrasound transducer that is inserted into the vagina
Citations
- Sweet, M. G., Schmidt-Dalton, T. A., Weiss, P. M., & Madsen, K. P. (2012). Evaluation and management of abnormal uterine bleeding in premenopausal women. American Family Physician , 85, 35–43.
- French, L. (2005). Dysmenorrhea. American Family Physician , 71, 285–291.
- Master-Hunter, T., & Heiman, D. L. (2006). Amenorrhea: Evaluation and treatment. American Family Physician , 73, 1374–1382.
- Apgar, B. S., Kaufman, A. H., George-Nwogu, U., & Kittendorf, A. (2007). Treatment of menorrhagia. American Family Physician , 75, 1813–1819.
- Practice Committee of the American Society for Reproductive Medicine. (2008). Current evaluation of amenorrhea. Fertility and Sterility , 90, S219–S225.
What are the common treatments for menstrual irregularities?
Treatments for menstrual irregularities often vary based on the type of irregularity and certain lifestyle factors, such as whether a woman is planning to get pregnant.
Treatment for menstrual irregularities that are due to anovulatory bleeding (absent periods, infrequent periods, and irregular periods) include:1,2
- Oral contraceptives
- Cyclic progestin
- Treatments for an underlying disorder that is causing the menstrual problem, such as counseling and nutritional therapy for an eating disorder
Treatment for menstrual irregularities that are due to ovulatory bleeding (heavy or prolonged menstrual bleeding) include:1,3,4,5,6
- Insertion of a hormone-releasing intrauterine device
- Use of various medications (such as those containing progestin or tranexamic acid) or nonsteroidal anti-inflammatory medications
If the cause is structural or if medical management is ineffective, then the following may be considered:
- Surgical removal of polyps or uterine fibroids
- Uterine artery embolization, a procedure to block blood flow to the uterus
- Endometrial ablation, a procedure to cauterize (remove or close off by burning) blood vessels in the endometrial lining of the uterus
- Hysterectomy
Treatment for dysmenorrhea (painful periods) include:7
- Applying a heating pad to the abdomen
- Taking nonsteroidal anti-inflammatory medications
- Taking contraceptives, including injectable hormone therapy or birth control pills, using varied or less common treatment regimens
Citations
- ACOG Committee on Practice Bulletins—Gynecology, American College of Obstetricians and Gynecologists. (2013). Practice bulletin no. 136: Management of abnormal uterine bleeding associated with ovulatory dysfunction. Obstetrics and Gynecology, 122(1), 176–185. PMID: 23787936. Retrieved December 2, 2016, from https://www.guideline.gov/summaries/summary/47451
- Practice Committee of the American Society for Reproductive Medicine. (2008). Current evaluation of amenorrhea. Fertility and Sterility, 90 , S219–S225.
- Apgar, B. S., Kaufman, A. H., George-Nwogu, U., & Kittendorf, A. (2007). Treatment of menorrhagia. American Family Physician , 75, 1813–1819.
- Lethaby, A., Irvine, G., & Cameron, I. (1998). Cyclical progestogens for heavy menstrual bleeding. Cochrane Database of Systematic Reviews, 4, CD001016.
- Lethaby, A. E., Cooke, I., & Rees, M. (2005). Progesterone/progestogen releasing intrauterine systems versus either placebo or any other medication for heavy menstrual bleeding. Cochrane Database of Systematic Reviews, 4, CD002126.
- Lethaby, A., Shepperd, S., Cooke, I., & Farquhar, C. (1999). Endometrial resection and ablation versus hysterectomy for heavy menstrual bleeding. Cochrane Database of Systematic Reviews, 2, CD000329.
- Proctor, M. L., & Farquhar, C. M. (2007). Dysmenorrhoea. Clinical Evidence , pii, 0813.
NICHD Menstruation Research Goals
Understanding and maximizing women’s health has been part of the NICHD mission since the Institute was founded. Research on menstruation and menstrual irregularities is an important part of addressing this mission.
Fertility status is viewed as an important marker of overall health in that irregularities in the menstrual cycle, including those that affect fertility, may signal a larger health problem. As a result, NICHD research on menstruation and menstrual irregularities falls into multiple disciplines, such as reproductive endocrinology, infertility/fertility research, and reproductive and regenerative medicine, as well as specific studies of gynecological disorders that affect menstruation, such as endometriosis, uterine fibroids, and polycystic ovary syndrome.
In addition, the NICHD-funded Reproductive Medicine Network conducts large, multicenter clinical trials of diagnostic and therapeutic interventions for infertility and reproductive diseases and disorders to help advance treatment options for women affected by these conditions.
Menstruation Research Activities and Advances
NICHD conducts and supports research to learn more about normal menstruation and menstrual irregularities.
The following organizational units address issues related to menstruation and the causes and effects of menstrual irregularities:
- The Division of Population Health Research (DiPHR) is interested in statistical methodology, comparative etiologies, and the health endpoints needed to identify mechanisms, at-risk groups, and interventions. Some of these activities include:
- Gaining a better understanding of the intricate relationship between hormone levels (estrogen, progesterone, luteinizing hormone, etc.) and oxidative stress during the menstrual cycle. Oxidative stress may be associated with the risk of infertility in both males and females. Data from the BioCycle Study are helping researchers examine the intracycle variation of oxidative stress, reproductive hormones, inflammation, and metabolic biomarkers; the relation between hormone levels and oxidative stress during the menstrual cycle in premenopausal women; and the influence of external factors (such as dietary intake, cigarette smoking, alcohol consumption, and exercise) on oxidative stress and hormone levels.
- Developing various approaches to modeling menstrual cycle function. The menstrual cycle is a complex process that involves multiple hormones regulated by feedback mechanisms. To describe the factors associated with menstrual cycle function and inform women's health research, the DIPHR is developing statistical models to answer questions like:
* What is the "typical" menstrual cycle pattern in a population of women?
* How do lifestyle factors that vary between women (e.g., dietary intake, physical activity, stress) affect a typical menstrual cycle?
* How does the variation in menstrual cycle function differ between women and across consecutive cycles on the same woman?
* What is the inter-relationship between multiple hormones across the menstrual cycle? - Determining the relationships between endometriosis and environmental chemicals, lifestyle, and medical history. The Endometriosis: Natural History, Diagnosis, and Outcomes (ENDO) Study is following 625 women undergoing surgery for this disorder, which often involves irregular, painful menstruation. The study compares these women's medical findings, life characteristics, and other factors to those of women of similar age and location who don't have endometriosis.
- Various components of the Division of Intramural Research study aspects of menstruation and menstrual irregularities. For example:
- The Section on Reproductive Endocrinology works on endometrial physiology and endometriosis pathologies. The section has published studies on the endometrium, localization of lesions in endometriosis, characterizing receptors, and the use of raloxifene as a treatment for endometriosis. This section also published a landmark article on the hypothalamic-pituitary-adrenal (HPA) axis during pregnancy.
- The Unit on Reproductive and Regenerative Medicine conducts research on disorders that affect reproduction. The section is interested in endometrial stem cells and disorders that affect the endometrium. These disorders can result in scarring of the uterine cavity, abnormal bleeding, endometriosis, infertility due to implantation failures, and recurrent pregnancy loss.
- The Unit on Reproductive Endocrinology and Infertility is studying the relationship between the BRX gene complex and uterine fibroid generation. The laboratory also is studying gene regulation and growth factors involved in uterine fibroid development.
- The Unit on Genetics of Puberty and Reproduction conducts research on the genetic basis of sexual maturation. In particular, researchers are examining the ways in which mutations in genes linked to pubertal development can lead to disorders of puberty and reproduction.
- Components of the Division of Extramural Research also support studies on normal menstruation and conditions related to menstrual irregularities.
- Fertility and Infertility (FI) Branch projects include work examining hormonal and neuroendocrine control of normal menstrual cycling, which can help provide insights into conditions where these normal processes are disrupted.
- A Pediatric Growth and Nutrition Branch project is investigating the relationship of amenorrhea to bone loss in adolescent and young adult athletes by examining the bone metabolism and body composition of young athletes.
- The Gynecologic Health and Disease Branch (GHDB) studies normal menstruation as well as diseases that cause menstrual irregularities, such as uterine fibroids, endometriosis, and polycystic ovary syndrome, to name a few. Projects include:
* Central pain mechanisms in primary dysmenorrhea: This project will examine how the nervous system and psychological factors play a role in the experience of dysmenorrhea.
* Neurophysiological diagnostics for menstrual pain: This study aims to determine whether involuntary muscle movements/reflexes (called visceral motor reflexes or VMRs) can be measured to evaluate the pain experienced by women with different types of pelvic pain. The study will compare these VMRs in women with primary dysmenorrhea and women with chronic pelvic pain to determine which nerve pathways are responsible for the pain experienced and to potentially identify targets for treatment.
- The Uterine Fibroids and Women’s Health fact sheet describes NICHD research on uterine fibroids and women's health, and reviews recent advances in understanding, diagnosing, and treating them.
- The Polycystic Ovary Syndrome (PCOS) and Women's Health fact sheet describes NICHD research on PCOS and women's health. It highlights recent projects and findings related to PCOS causes, symptoms, and treatments.
- The Endometriosis and Women’s Health fact sheet describes NICHD’s support of research on this common gynecologic condition and highlights some recent findings and advances from NICHD-funded projects.
- Through the FI Branch, NICHD supports the following research networks and centers programs that contribute to understanding menstrual irregularities within the context of fertility and infertility:
- Reproductive Medicine Network (RMN)
- Reproductive Scientist Development Program (RSDP)
- National Centers for Translational Research in Reproduction and Infertility (NCTRI) (Formerly the Specialized Cooperative Centers Program in Reproduction and Infertility Research [SCCPIR])
- The GHDB supports the Women's Reproductive Health Research (WRHR) Career Development Program, which allows obstetricians/gynecologists who have recently completed clinical training to enhance their education and experience with basic, translational, and clinical research on women's health topics, including normal menstruation and menstrual irregularities.