Walking abnormalities: MedlinePlus Medical Encyclopedia (original) (raw)
Walking abnormalities can be caused by many different types of problems. Problems with the joints, (such as arthritis), bones (such as deformities), circulation (such as peripheral vascular disease), or even pain can make it difficult to walk properly. Diseases or injuries to the nerves, muscles, brain, spinal cord, or inner ear can affect normal walking.
The pattern of how a person walks is called the gait. Different types of walking problems occur without a person's control. Most, but not all, are due to a physical condition.
Some walking abnormalities have been given names:
- Propulsive gait -- a stooped, stiff posture with the head and neck bent forward.
- Spastic gait -- a stiff, foot-dragging walk caused by a long muscle contraction on one side.
- Scissoring gait -- legs flexed slightly at the hips and knees like crouching, with the knees and thighs hitting or crossing in a scissors-like movement. A scissoring gait is often a more severe form of a spastic gait.
- Steppage gait -- foot drop where the foot hangs with the toes pointing down, causing the toes to scrape the ground while walking, requiring someone to lift the leg higher than normal when walking.
- Waddling gait -- a duck-like walk that may appear in childhood or later in life.
- Ataxic, or broad-based, gait -- feet wide apart with irregular, jerky, and weaving or slapping when trying to walk.
- Magnetic gait -- shuffling with feet feeling as if they stick to the ground.
- Antalgic gait -- when pain prevents the normal motion of the feet or legs.
- Shuffling gait -- when the feet don't lift normally and slide on the ground, often due to Parkinson disease.
Abnormal gait may be caused by diseases in different areas of the body.
General causes of abnormal gait may include:
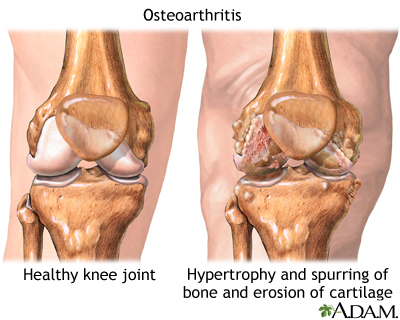
- Arthritis of the spine, hip, leg, or foot joints
- Conversion disorder (a mental disorder)
- Foot problems (such as a callus, corn, ingrown toenail, wart, pain, skin sore, swelling, or spasms)
- Broken bone
- Injections into muscles that causes soreness in the leg or buttocks
- Infection
- Injury
- Legs that are of different lengths
- Inflammation or swelling of the muscles (myositis)
- Shin splints
- Shoe problems
- Inflammation or swelling of the tendons (tendinitis)
- Torsion of the testis
- Brain, spinal cord, and peripheral nerve diseases
- Vision problems
- Inner ear problems
This list does not include all causes of abnormal gait.
CAUSES OF SPECIFIC GAITS
Propulsive gait:
- Carbon monoxide poisoning
- Manganese poisoning
- Parkinson disease
- Use of certain drugs, including phenothiazines, haloperidol, thiothixene, loxapine, and metoclopramide (usually, drug effects are temporary)
Spastic or scissoring gait:
- Autoimmune disorders such as systemic lupus
- Brain abscess
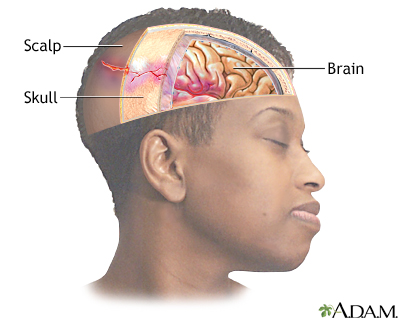
- Brain or head trauma
- Brain tumor
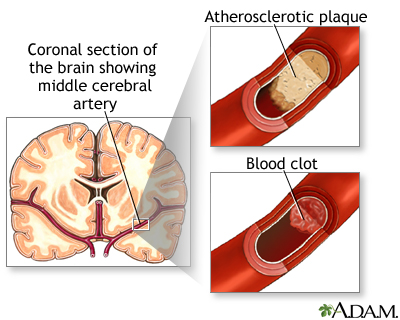
- Stroke
- Cerebral palsy
- Cervical spondylosis with myelopathy (a problem with the vertebrae in the neck)
- Infections such as Lyme disease, syphilis, HIV, and others
- Liver failure
- Multiple sclerosis (MS)
- Spinal cord trauma
- Spinal cord tumor
- Neurosyphilis (bacterial infection of the brain or spinal cord due to syphilis)
- Syringomyelia (collection of cerebrospinal fluid that forms in the spinal cord)
- Vitamin or mineral deficiency (low Vitamin B12, Vitamin E, or copper levels)
Steppage gait:
- Neuropathy such as Guillain-Barre syndrome and hereditary neuropathy
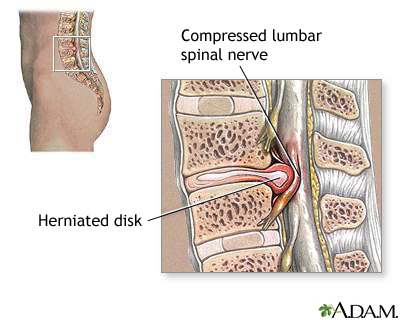
- Herniated lumbar disk
- Multiple sclerosis
- Muscle weakness of the tibia
- Peroneal neuropathy
- Polio
- Spinal cord injury
- Muscle diseases
The conditions that cause spastic or scissoring gait can also cause steppage gait.
Waddling gait:
- Congenital hip dysplasia
- Muscular dystrophy (group of inherited disorders that cause muscle weakness and loss of muscle tissue)
- Muscle disease (myopathy)
- Spinal muscle atrophy
Ataxic, or broad-based, gait:
- Cerebellar ataxia (uncoordinated muscle movement due to disease or injury to the cerebellum in the brain)
- Chiari or other malformation
- Alcohol intoxication
- Brain injury
- Progressive damage to nerve cells in the cerebellum of the brain (cerebellar degeneration)
- Medicines (phenytoin and other anti-seizure medicines)
- Polyneuropathy (damage to many nerves, as occurs with diabetes)
- Stroke or bleeding in the cerebellum
Magnetic gait:
- Disorders that affect the front part of the brain
- Hydrocephalus (increased fluid in the brain)
Treating the underlying cause often improves the gait. For example, gait abnormalities from trauma to part of the leg will improve as the leg heals.
Physical therapy almost always helps with short-term or long-term gait disorders. Therapy will reduce the risk for falls and other injuries.
For an abnormal gait that occurs with conversion disorder, counseling and support from family members are strongly recommended.
For any gait problem that is likely to be long term, reduce fall risk by modifying one's surroundings. Keep pathways well-lit and free of clutter like wires and other hazards. Remove loose rugs and install grab bars or railings.
For a propulsive gait:
- Encourage the person to be as independent as possible.
- Allow plenty of time for daily activities, especially walking. People with this problem are likely to fall because they have poor balance and are always trying to catch up.
- Provide walking assistance for safety reasons, especially on uneven ground.
- See a physical therapist for exercise therapy and walking retraining.
For a scissoring or spastic gait:
- People with a scissoring gait often lose skin sensation. Skin care should be used to avoid skin sores.
- Leg braces and in-shoe splints can help keep the foot in the right position for standing and walking. A physical therapist can supply these and provide exercise therapy, if needed.
- Exercises are encouraged.
- A cane or a walker is recommended for those with poor balance.
- Medicines (muscle relaxers, anti-spasticity medicines) can reduce the muscle overactivity.
For a steppage gait:
- Get enough rest. Fatigue can often cause a person to stub a toe and fall.
- Leg braces or orthoses and in-shoe splints can help keep the foot in the best position for standing and walking. A physical therapist can supply these and provide exercise therapy, if needed. For some, a high-top boot may be sufficient.
For a waddling gait, follow the treatment your health care provider prescribed. Bracing, canes and walkers can be of help.
For a magnetic gait due to hydrocephalus, walking may improve after the excess fluid is treated.
If there is any sign of uncontrollable and unexplained gait abnormalities, contact your provider.
The provider will take a medical history and perform a physical examination.
Medical history questions may include:
- Time pattern, such as when the problem started, and if it came on suddenly or gradually
- Type of gait disturbance, such as any of those mentioned above
- Other symptoms, such as pain and its location, paralysis, whether there's been a recent infection
- What medicines are being taken
- Injury history, such as leg, head, or spinal injury
- Other illnesses such as polio, tumors, stroke, or other blood vessel problems
- If there have been recent treatments such as vaccinations, surgery, chemotherapy, or radiation therapy
- Self and family history, such as birth defects, diseases of the nervous system, growth problems, problems of the spine
The physical examination will include muscle, bone, and nervous system examination. The provider will decide which tests to do based on the results of the physical examination.
Magee DJ, Manske RC. Assessment of gait. In: Magee DJ, Manske RC, eds. Orthopedic Physical Assessment. 7th ed. St Louis, MO: Elsevier; 2021:chap 14.
Thompson PD, Nutt JG. Gait disorders. In: Jankovic J, Mazziotta JC, Pomeroy SL, Newman NJ, eds. Bradley and Daroff's Neurology in Clinical Practice. 8th ed. Philadelphia, PA: Elsevier; 2022:chap 25.
Updated by: Joseph V. Campellone, MD, Department of Neurology, Cooper Medical School of Rowan University, Camden, NJ. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.