Mixed Viral-Bacterial Infections and Their Effects on Gut Microbiota and Clinical Illnesses in Children (original) (raw)
Introduction
The human gastrointestinal tract (GIT) is a reservoir of the largest community of commensals in the body, and hence, recent research has studied gut microbiome extensively[1](/articles/s41598-018-37162-w#ref-CR1 "Arora, S. K., Dewan, P. & Gupta, P. Microbiome: Paediatricians’ perspective. Indian J Med Res 142, 515–524, https://doi.org/10.4103/0971-5916.171275
(2015)."),[2](/articles/s41598-018-37162-w#ref-CR2 "Althani, A. A. et al. Human Microbiome and its Association With Health and Diseases. Journal of cellular physiology 231, 1688–1694,
https://doi.org/10.1002/jcp.25284
(2016)."). Gut microflora plays a crucial role in health and disease through maintaining several physiological processes such as food digestion, immunity and metabolism[3](#ref-CR3 "Bermon, S. et al. The microbiota: an exercise immunology perspective. Exerc Immunol Rev 21, 70–79 (2015)."),[4](#ref-CR4 "Flint, H. J., Scott, K. P., Louis, P. & Duncan, S. H. The role of the gut microbiota in nutrition and health. Nat Rev Gastroenterol Hepatol 9, 577–589,
https://doi.org/10.1038/nrgastro.2012.156
(2012)."),[5](#ref-CR5 "Nieuwdorp, M., Gilijamse, P. W., Pai, N. & Kaplan, L. M. Role of the microbiome in energy regulation and metabolism. Gastroenterology 146, 1525–1533,
https://doi.org/10.1053/j.gastro.2014.02.008
(2014)."),[6](/articles/s41598-018-37162-w#ref-CR6 "Reinhardt, C. et al. Tissue factor and PAR1 promote microbiota-induced intestinal vascular remodelling. Nature 483, 627–631,
https://doi.org/10.1038/nature10893
(2012)."). Consequently, alteration of the structure and function of gut microflora has been linked to several human complications including colonization of pathogenic bacteria, susceptibility to autoimmune disorders, obesity, and gastrointestinal disorders such as inflammatory bowel disease[1](/articles/s41598-018-37162-w#ref-CR1 "Arora, S. K., Dewan, P. & Gupta, P. Microbiome: Paediatricians’ perspective. Indian J Med Res 142, 515–524,
https://doi.org/10.4103/0971-5916.171275
(2015)."),[7](#ref-CR7 "Maruvada, P., Leone, V., Kaplan, L. M. & Chang, E. B. The Human Microbiome and Obesity: Moving beyond Associations. Cell Host Microbe 22, 589–599,
https://doi.org/10.1016/j.chom.2017.10.005
(2017)."),[8](#ref-CR8 "Reeves, A. E. et al. The interplay between microbiome dynamics and pathogen dynamics in a murine model of Clostridium difficile Infection. Gut Microbes 2, 145–158 (2011)."),[9](/articles/s41598-018-37162-w#ref-CR9 "Giongo, A. et al. Toward defining the autoimmune microbiome for type 1 diabetes. ISME J 5, 82–91,
https://doi.org/10.1038/ismej.2010.92
(2011).").Healthy children gut microbiota is dynamic and undergoes rapid changes, which is affected by multiple factors including mode of birth delivery, aging process, diet, and use of antibiotics[10](/articles/s41598-018-37162-w#ref-CR10 "Hollister, E. B. et al. Structure and function of the healthy pre-adolescent pediatric gut microbiome. Microbiome 3, 36, https://doi.org/10.1186/s40168-015-0101-x
(2015)."). GIT microbiome in children is largely colonized by bacteria belonging to Bacteroidetes, Firmicutes and Proteobacteria phyla[11](/articles/s41598-018-37162-w#ref-CR11 "Palmer, C., Bik, E. M., DiGiulio, D. B., Relman, D. A. & Brown, P. O. Development of the human infant intestinal microbiota. PLoS Biol 5, e177,
https://doi.org/10.1371/journal.pbio.0050177
(2007)."). Facultative bacteria such as _Escherichia coli_ (_E_. _coli_), _Enterococcus_, α-hemolytic _Streptococci_, and _Staphylococcus_ species have been found to colonize the anaerobic GIT of infants during their first days after birth, followed by colonization of anaerobic bacteria including _Bacteroides_, _Bifidobacterium_, and _Clostridium_ species, due to the presence of anaerobic conditions and human milk oligosaccharides[12](/articles/s41598-018-37162-w#ref-CR12 "Johnson, C. L. & Versalovic, J. The human microbiome and its potential importance to pediatrics. Pediatrics 129, 950–960,
https://doi.org/10.1542/peds.2011-2736
(2012)."). Typically, the healthy gut microbiota is composed of only a minor proportion of Proteobacteria phylum, and thus, high abundance of these bacteria is often a sign of imbalanced microbiome[13](/articles/s41598-018-37162-w#ref-CR13 "Karmali, M. A. Infection by verocytotoxin-producing Escherichia coli. Clinical microbiology reviews 2, 15–38 (1989)."),[14](/articles/s41598-018-37162-w#ref-CR14 "Shin, N. R., Whon, T. W. & Bae, J. W. Proteobacteria: microbial signature of dysbiosis in gut microbiota. Trends Biotechnol 33, 496–503,
https://doi.org/10.1016/j.tibtech.2015.06.011
(2015).").GIT is also a common site of infections in children younger than 5 years[15](/articles/s41598-018-37162-w#ref-CR15 "Fletcher, S. M., McLaws, M.-L. & Ellis, J. T. Prevalence of Gastrointestinal Pathogens In Developed and Developing Countries: Systematic Review and Meta-Analysis. Journal of Public Health Research 2, 42–53, https://doi.org/10.4081/jphr.2013.e9
(2013)."). Acute gastroenteritis (AGE) leads to around 1.34 million deaths annually, or nearly 15% of all child fatalities[16](/articles/s41598-018-37162-w#ref-CR16 "Chow, C. M., Leung, A. K. C. & Hon, K. L. Acute gastroenteritis: from guidelines to real life. Clinical and experimental gastroenterology 3, 97–112 (2010)."),[17](/articles/s41598-018-37162-w#ref-CR17 "do Carmo, G. M. I. et al. Decline in Diarrhea Mortality and Admissions after Routine Childhood Rotavirus Immunization in Brazil: A Time-Series Analysis. PLoS Medicine 8, e1001024,
https://doi.org/10.1371/journal.pmed.1001024
(2011)."). Viral infections remain the leading cause of AGE in children, particularly noroviruses (NoV) and rotaviruses (RV)[18](/articles/s41598-018-37162-w#ref-CR18 "Elliott, E. J. Acute gastroenteritis in children. BMJ 334, 35–40,
https://doi.org/10.1136/bmj.39036.406169.80
(2007)."). NoV are group of RNA viruses that are responsible for about one fifth of AGE cases globally[19](/articles/s41598-018-37162-w#ref-CR19 "CDC. Norovirus Worldwide,
https://www.cdc.gov/norovirus/worldwide.html
(2016)."). Annually, these viruses lead to around 200 million cases in children less than 5 years old, and result in about 50,000 fatalities[19](/articles/s41598-018-37162-w#ref-CR19 "CDC. Norovirus Worldwide,
https://www.cdc.gov/norovirus/worldwide.html
(2016)."),[20](/articles/s41598-018-37162-w#ref-CR20 "CDC. Burden of Norovirus Illness and Outbreaks,
https://www.cdc.gov/norovirus/php/illness-outbreaks.html
(2016)."). RV is also one of the main viral agents of AGE worldwide. Despite the availability of rotavirus vaccine (RVV), this virus is the most common cause of diarrhea related deaths in children, contributing to 215,000 deaths in young children every year, particularly in low-income countries[21](/articles/s41598-018-37162-w#ref-CR21 "WHO. Immunization, Vaccines and Biologicals - Rotavirus,
http://www.who.int/immunization/diseases/rotavirus/en/
(2016)."),[22](/articles/s41598-018-37162-w#ref-CR22 "Harris, V. C. et al. Significant Correlation Between the Infant Gut Microbiome and Rotavirus Vaccine Response in Rural Ghana. J Infect Dis 215, 34–41,
https://doi.org/10.1093/infdis/jiw518
(2017).").Gut microflora plays a critical role in immune response and pathogenesis of GIT infection especially in young children, where GIT infections are major cause of morbidity and mortality. Accordingly, several studies have investigated the correlation between intestinal microbiota composition and immune response to RVV[22](#ref-CR22 "Harris, V. C. et al. Significant Correlation Between the Infant Gut Microbiome and Rotavirus Vaccine Response in Rural Ghana. J Infect Dis 215, 34–41, https://doi.org/10.1093/infdis/jiw518
(2017)."),[23](#ref-CR23 "Harris, V. et al. Rotavirus vaccine response correlates with the infant gut microbiota composition in Pakistan. Gut Microbes, 1–9,
https://doi.org/10.1080/19490976.2017.1376162
(2017)."),[24](/articles/s41598-018-37162-w#ref-CR24 "Chen, S. Y. et al. Intestinal microbiome in children with severe and complicated acute viral gastroenteritis. Sci Rep 7, 46130,
https://doi.org/10.1038/srep46130
(2017)."). On the other hand, immune tolerance to gut microflora is an essential component of mucosal immunity[25](/articles/s41598-018-37162-w#ref-CR25 "Hand, T. W. et al. Acute gastrointestinal infection induces long-lived microbiota-specific T cell responses. Science 337, 1553–1556,
https://doi.org/10.1126/science.1220961
(2012)."). Loss of this immune tolerance has been reported as a consequence GIT infection, where immune response to commensals parallels the immune response to pathogenic microorganisms[25](/articles/s41598-018-37162-w#ref-CR25 "Hand, T. W. et al. Acute gastrointestinal infection induces long-lived microbiota-specific T cell responses. Science 337, 1553–1556,
https://doi.org/10.1126/science.1220961
(2012)."). Virally-infected infant’s exhibit altered gut microbiota after infection, which may put them at higher risk of developing health complications[26](/articles/s41598-018-37162-w#ref-CR26 "Nelson, A. M. et al. Disruption of the Human Gut Microbiota following Norovirus Infection. PLOS ONE 7, e48224,
https://doi.org/10.1371/journal.pone.0048224
(2012)."). More recently, it was reported that children with severe viral AGE, particularly patients infected with RV, have decreased intestinal microbiota diversity compared to healthy controls[24](/articles/s41598-018-37162-w#ref-CR24 "Chen, S. Y. et al. Intestinal microbiome in children with severe and complicated acute viral gastroenteritis. Sci Rep 7, 46130,
https://doi.org/10.1038/srep46130
(2017)."). The use of antibiotics following viral infections has also been linked to gut microbiota alteration in children[25](#ref-CR25 "Hand, T. W. et al. Acute gastrointestinal infection induces long-lived microbiota-specific T cell responses. Science 337, 1553–1556,
https://doi.org/10.1126/science.1220961
(2012)."),[26](#ref-CR26 "Nelson, A. M. et al. Disruption of the Human Gut Microbiota following Norovirus Infection. PLOS ONE 7, e48224,
https://doi.org/10.1371/journal.pone.0048224
(2012)."),[27](/articles/s41598-018-37162-w#ref-CR27 "Rosengaus, R. B., Zecher, C. N., Schultheis, K. F., Brucker, R. M. & Bordenstein, S. R. Disruption of the termite gut microbiota and its prolonged consequences for fitness. Applied and environmental microbiology 77, 4303–4312,
https://doi.org/10.1128/aem.01886-10
(2011)."). Nonetheless, the current data concerning the contribution of gut microbiota in the development, complications, and pathogenesis of AGE is still limited, which underscores the need for more investigations.In this present study, we evaluated gut microbiota composition in children suffering from viral or mixed infection with two major viruses (RV and NoV) and two pathogenic bacteria [Enteroaggregative E. coli (EAEC), and Enteropathogenic E. coli (EPEC)]. In addition, we investigated the correlation between gut microbiome alterations due to various infections and disease manifestations.
Results
Patient characteristics and study design
A total of 79 fecal samples were analyzed, including 70 stool samples from children suffering from AGE [RV (n = 40) and NoV (n = 30); median age of 14 months], and nine samples from healthy children [median age of 13.5 months]. Of the 40 RV positive children, 18 children had RV-alone infection (Vesikari score ≤10), eight had mixed infection with RV + EAEC (Vesikari score >10), nine had RV + EPEC infection (Vesikari score > 10) and five samples had RV + EPEC + EAEC mixed infection (Vesikari score > 10). Of the 30 NoV positive samples, 17 had NoV-alone infection (Vesikari score ≤10), eight had NoV + EAEC (Vesikari score <10) and five children had NoV + EPEC infection (Vesikari score > 10). We did not have NoV + EPEC + EAEC, nor single bacterial infections to include in the analysis. The number of children vaccinated with RVV in the NoV group [NoV: 76.5% (13/17), NoV + EAEC: 71.4% (5/7), NoV + EPEC: 80% (4/5)] was higher compared to RV group [RV: 61.1% (11/18), RV + EAEC: 62.5% (5/8), RV + EPEC: 60% (6/10) and RV + EPEC + EAEC: 40% (2/5)]. Children admitted to pediatric emergency center with AGE were observed to have multiple clinical characteristics comprised of fever, prolonged period of diarrhea, vomiting, hospitalization and both mild to moderate dehydration. All fecal samples were collected before the administration of any medications. Table 1 summarizes the clinical characteristics and conditions of the children enrolled in this study.
Table 1 Clinical characteristics and conditions of the children enrolled in this study.
Mapping the microbiome community composition and biodiversity in AGE patients and healthy controls
We sequenced 16S (V4 region) genes on an Illumina MiSeq. Raw Fastq files were quality-filtered and clustered into 97% similarity operational taxonomic units (OTUs) using the mothur software package[28](/articles/s41598-018-37162-w#ref-CR28 "Schloss., MiSeq SOP, http://www.mothur.org/wiki/MiSeq_SOP
(2013)."). For all samples, we obtained 1.488075 × 106 high-quality 16S rRNA sequence reads generated from Miseq Illumina platform. The final dataset yielded 8118 OTUs including those bacteria with a count of one. The read range which was between 1436 and 3.17 × 104 denotes the size of the sequences aligned for the identified OTUs. High quality reads were classified using Greengenes (v. 13\_8) as the reference database. We obtained a consensus taxonomy for each OTU. We then aggregated OTU abundances into genera, and plotted the relative abundances of the most abundant ones with Analysis of variance (ANOVA). We have represented a plot to denote the most abundant genera for each cohort (Fig. [1](/articles/s41598-018-37162-w#Fig1)), as well as per each group independently (Supplementary Fig. [1](/articles/s41598-018-37162-w#MOESM1)). The results of positive correlation between relative abundance and prevalence was calculated by using Spearman’s correlation coefficient. We summarized OTU abundances with the Bray-Curtis index and performed a non-metric multidimensional scaling (NMDS) analysis to visualize microbiome similarities[28](/articles/s41598-018-37162-w#ref-CR28 "Schloss., MiSeq SOP,
http://www.mothur.org/wiki/MiSeq_SOP
(2013)."). We used a Permutational analysis of variance (PERMANOVA) to test the significance of group differences[29](/articles/s41598-018-37162-w#ref-CR29 "Kozich, J. J., Westcott, S. L., Baxter, N. T., Highlander, S. K. & Schloss, P. D. Development of a dual-index sequencing strategy and curation pipeline for analyzing amplicon sequence data on the MiSeq Illumina sequencing platform. Applied and environmental microbiology 79, 5112–5120,
https://doi.org/10.1128/aem.01043-13
(2013)."). Enteric bacteria in the 79 fecal samples were classified into 24 phyla, 154 families, and 273 genera based 16S rRNA sequences and metagenomics analysis of the selected reads. The complete AGE bacterial communities and the relative abundance for each genus, phylum and family level for all children samples are listed in Additional File 1\. We categorized samples into two cohorts: RV cohort which includes RV, RV + EAEC, RV + EPEC, RV + EAEC + EPEC, and NoV cohort which includes NoV, NoV + EAEC, and NoV + EPEC. The relative abundance of species in each group was compared with other groups to determine the relatedness.Figure 1
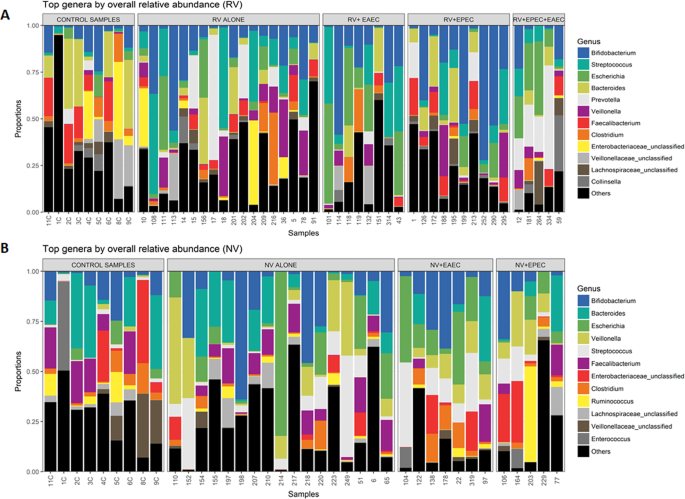
Community clustering and composition of top genera of bacterial species and their overall relative abundance in 79 children. All gut microbiota OTU profiles of the patients were aggregated into genera and plotted. “Other” under the genus represents lower-abundance taxa. Optimal number of consensus taxonomy was obtained for each OTU and 12 most abundant genera were displayed. (A) Clustering and composition of top 12 genera in RV cohort in comparison with control group. (B) Clustering and composition of top 12 genera in NoV cohort in comparison with control group.
In all AGE samples, 273 bacterial genera were detected. Despite this large number of gut microbes, a relatively small collection of genera represented 90% of all bacterial reads in all samples. Distinct bacterial composition and communities were present between healthy samples as compared with RV and NoV groups, which differed in both diversity and composition [Fig. 1(A,B)]. We identified 12 genera showing significant differences of relative abundance in community between RV and NoV infected children. We found a positive correlation between relative abundance and prevalence of bacteria in both RV and NoV cohorts. That is, a genus highly abundant in one sample was also highly prevalent across all samples of the same group. The twelve most abundant genera in RV infected groups were Bifidobacterium, Streptococcus, Escherichia, Bacteroides, Prevotella, Veillonella, Faecalibacterium, Clostridium, Collinsella and unclassified genus of Enterobacteriaceae, Veillonellaceae and Lachnospiraceae [Fig. 1(A)]. Specifically, genera (abundance value) which includes Streptococcus (0.124), Escherichia (0.107), Prevotella (0.0759) and Veillonella (0.0633) showed the highest prevalence and relative abundance, and accounted in average for 77.5% of the bacteria in RV positive samples. In the RV + EAEC mixed-infection group, Streptococcus and Escherichia genera were also more prevalent and relatively abundant. Both genera declined in the RV + EPEC mixed-infection with a mean relative abundance of 0.25 and 0.37, though they were prevalent in all samples. Interestingly, predominant abundance of genera Prevotella and Escherichia was observed in RV + EAEC + EPEC mixed infections with a mean relative abundance of 0.75 when present. Relative abundance with respect to unclassified genera, Lachnospiraceae and Collinsella, were abundant in RV + EPEC and RV + EPEC + EAEC, while less abundant in RV + EAEC [Fig. 1(A)]. The twelve top bacterial genera and their overall relative abundance per each group individually are represented in Supplementary Data S1- Fig. 1. Abundance of specific genera was also noticed in each of RV groups, particularly Oscillospira (0.0141) (RV-alone and RV + EAEC), Dialister (0.0256) and Megamonas (0.0385) (RV + EPEC), and Sutterella (0.0122) (RV + EAEC + EPEC).
On the other hand, the twelve most abundant genera for NoV cohort were Bifidobacterium, Bacteroides, Escherichia, Veillonella, Streptococcus, Faecalibacterium, Clostridium, Ruminococcus, Enterococcus and unclassified genus of Enterobacteriaceae, Veillonellaceae and Lachnospiraceae. Escherichia, Veillonella, Streptococcus, Faecalibacterium and an unknown genus belonging to the Lachnospiraceae were highly prevalent across all NoV positive samples with an average of 60.8%. [Fig. 1(B)]. NoV + EAEC mixed infections was dominated by high levels of Streptococcus, Escherichia and Clostridium genera. Although similar pattern was observed with NoV + EPEC mixed infections, it was with lesser abundance. It was also interesting to observe that though Enterococcus (0.00575) and Veillonellaceae unclassified (0.0157) were listed among the top genera by overall relative abundance in NoV cohort, they were found less abundant in NoV + EAEC and NoV + EPEC groups. We observed that Collinsella and Prevotella which were among the top 12 genera in RV cohort, were not entitled in NoV abundant genera. Similarly, unique genera of Ruminococcus and Enterococcus were observed in NoV cohort, but were absent in RV cohort. The twelve top bacterial genera and their overall relative abundance per each group including healthy controls and NoV cohort are represented in Supplementary Data S1- Fig. 2. Abundance of specific genera was also noticed in each NoV groups particularly, Sutterella (0.0170) (NoV-alone and NoV + EAEC), Haemophilus (0.0163) (NoV-alone), Oscillospira (0.0377) and Dorea (0.022) (NoV + EPEC). In general, we noticed that genus Bifidobacterium was less abundant, but prevalent in all the samples of RV and NoV cohorts. On the other hand, genus Bacteroides was dominantly abundant in control samples and reduced significantly in RV cohort compared to NoV cohort [Fig. 1(B)].
Richness, diversity and differential abundance of gut microbiota of AGE children
To further characterize the inter-individual differences between groups (beta-diversity) at the group level, post-hoc test and NMDS were performed. Pairwise differences: post-hoc test of gut microbiome in healthy children and AGE infected children is shown in Table 2. NMDS analysis revealed separation and clustering of samples along NMDS1 axis, whilst species tended to cluster along NMDS2 [Fig. 2(A,B)]. Children with RV infection had significantly scattered clustering compared to the controls (_r_2 = 0.074, p = 0.013, pvalBon = 0.13), with higher significance observed in RV + EAEC (_r_2 = 0.146, p = 0.009, pvalBon = 0.09) and RV + EPEC + EAEC (_r_2 = 0.179, p = 0.010, pvalBon = 0.10) (Fig. 2(A) and Table 2]. However, children with RV + EPEC mixed infections appear to show significant clustering with higher p-value (r2 = 0.101, p = 0.045, pvalBon = 0.45) compared to the controls (Table 2 and Fig. 2). We did not detect obvious significant differences when we compared the diversity of RV alone infected children with their mixed infections groups. On the other hand, significance with higher p-value was observed between RV + EPEC and RV + EPEC + EAEC (_r_2 = 0.146, p = 0.043, pvalBon = 0.43) groups. Children with NoV infection showed microbe clustering compared to healthy samples with higher p-value (_r_2 = 0.067, p = 0.049, pvalBon = 0.29) but high significance was observed in NoV + EAEC (_r_2 = 0.165, p = 0.009, pvalBon = 0.054) [Fig. 2(B)]. Analysis of variance showed no significant association between NoV + EPEC mixed-infection group and controls (_r_2 = 0.097, p = 0.188, pvalBon = 1.12). Overall, the pairwise differences with the control samples indicated that mixed infections with RV cohort had significant associations, specifically RV + EAEC mixed infection (p < 0.05). On the other hand, only NoV infection and NoV + EAEC groups showed significant (p < 0.05) associations. Moreover, no association was observed with NoV + EPEC group (p = 1.88).
Table 2 Pairwise differences: post-hoc test of gut microbiome in healthy children and AGE (RV and NoV) infected children.
Figure 2
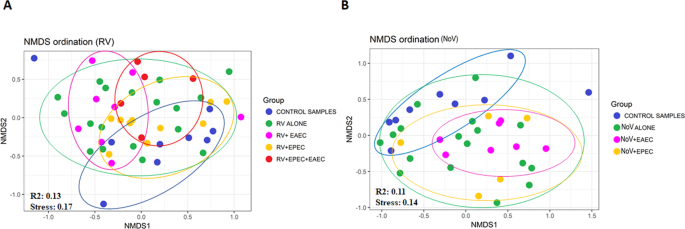
Nonmetric multidimensional scaling (NMDS) ordination of fecal microbiota in AGE infected patients. The Bray-Curtis index were performed between all infected children and controls to generate NMDS to visualize gut microbiome similarities. Each dot in the figure denotes microbiota profile of a single patient in a low-dimensional space. Colored dots denotes groups of patient’s microbiome. The subject’s cluster together depending upon their microbiome profiles. (A) NMDS ordination of microbiomes in control samples, RV-alone, RV + EAEC, RV + EPEC, and RV + EPEC + EAEC. (B) NMDS ordination of microbiomes in control samples, NV-alone, NV + EAEC, and NV + EPEC.
Shannon diversity index, reported as entropy scores, were calculated for control group and each infected group of children and elucidated in Fig. 3. The entropy score is known to increase as the number of species increases as well the distribution of individuals among the species becomes even. All RV infected groups reported lower entropy scores compared to the control group. Decrease in scores was more significant (p = 0.0024) in the mixed infections with EAEC, especially the RV + EAEC 1.65 (1.6–1.9). On the other hand, entropy scores were less divergent in the NoV groups, recoding the following values: NoV-alone 2.4 (2.0–2.7), NoV + EAEC 2.3 (2.0–2.5), and NoV + EPEC 2.3 (2.0–2.9), [Fig. 3(B)]. In summary, Shannon diversity indices suggested severe alteration in childrens’ gut microbiome communities with RV single and mixed-infections with EAEC.
Figure 3
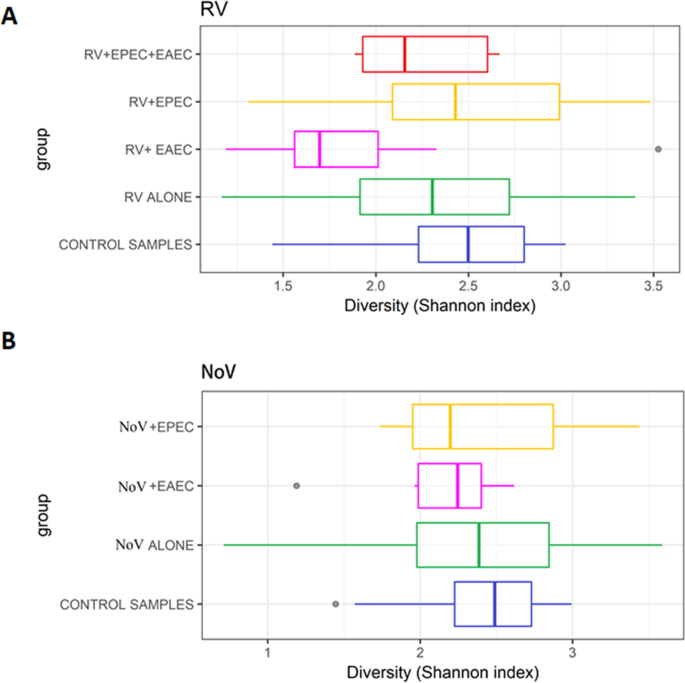
Shannon diversity index of microbiota among healthy controls and infected AGE cohorts. (A) Analysis of Shannon diversity index in control samples, RV-alone, RV + EAEC, RV + EPEC, and RV + EPEC + EAEC. (B) Analysis of Shannon diversity index in control samples, NV-alone, NV + EAEC, and NV + EPEC.
We observed 14 RV (_p_adjusted < 0.05) and 20 NoV (_p_adjusted < 0.01) differentially abundant OTUs, respectively, in infected children regardless of the bacterial co-infections [Supplementary Data S1- Fig. 3(A,B)]. Each of these OTUs represented 0.025–0.3% of the total abundance in RV cohort, and 0.0001 to 0.2% of the total abundance in NoV cohort. OTUs in RV cohort were associated with diverse range of bacteria including Roseburia, Blautia, Parabacteroides faecis, Fusobacterium, Gemella, Moraxella and Pullicaecorum [Supplementary Data S1- Fig. 3(A)]. Only five OTUs were significantly abundant in the RV-alone infected children group (_p_adjusted < 0.05), compared with healthy controls, including Melaninogenica, Blautia, Bacteroides, Fusobacterium and Gemella. Melaninogenica (0.003–0.015%) and Gemella (0.007 to 0.0015%) were observed in RV + EAEC whereas _Coprocococu_s (0.005 to 0.010%), Moraxella (0.001–0.06%) and Gemella (0.002–0.008%) were significantly abundant in RV + EPEC group. On the other hand, seven OTUs were differentially abundant in NoV cohort including Clostridium Citroniae (0.001–0.015%), Haemophilus parainfluenzae (0.01–0.03%), Alistipes putredinis (0.003–0.006%), Anaerostipes caccae (0.002–0.04%), Acinetobacter guillouiae (0.001–0.006%), Clostridiales (0.004–0.012), and Trachinotus ovatus (0.01 to 0.03). A comparison between EAEC- and EPEC-infected groups showed differential abundance of Streptococcus and Coprococcus in both RV + EAEC and NoV + EAEC children, whereas Coprococcus and Melaninogenica were differentially abundant in both RV + EPEC and NoV + EPEC [Supplementary Data S1- Fig. 3(B)]. Moreover, it was peculiarly noticed that the number of differential abundant pathogenic OTUs were found only with NoV mixed infection compared to RV mixed infected groups.
Correlation between microbiome composition and clinical manifestations in RV- and NoV- alone infected groups
The correlations of the gut microbiota composition with clinical manifestations were evaluated based on Table 1. The abundance of genus Clostridium resulted in increased frequency of diarrhea (6 to 7 times/day) and vomiting (6 times/day) in children with RV positive infection. Further, children with fever had greater richness in Prevotella compared to other genera. On the other hand, abundance of genus Streptococcus was observed to be associated with increase in diarrhea duration (7–8 days) in children with NoV positive infection.
RV-alone infected children with an increased frequency of diarrhea exhibited greater abundance of Sulfur River 1 (SR1) (50%), Lentisphaerae (50%), Nitrospirae (38%) and Caldiserica (5%), which were absent in NoV- alone infected and healthy children (Supplementary Data S1 – Fig. 4). Dominance of phyla Chlorobi was associated with moderate dehydration in NoV infected children. Microbial profiles and their correlation in phylum level between RV, NoV and healthy pediatric cohorts are shown in Supplementary Data S1 – Fig. 4.
Microbiome composition and clinical manifestations in mixed infections with EAEC
In the RV + EAEC mixed infection, children with an onset of AGE symptoms for more than 2 days prior to hospitalization exhibited significant abundance and Escherichia, and lesser abundance of Bacteroides. The abundance of Bacteroides was even lesser in NoV + EAEC group compared to RV + EAEC group. There was no abundance of specific genera that correlated with degree of dehydration in RV + EAEC group. However, genera Escherichia, Streptococcus, Rumella and Clostridium seemed to be specifically correlated with degree of dehydration in NoV + EAEC group. Analysis at the phylum level for viral-EAEC mixed infections did not show any significant difference in various microbial diversity indices as was observed in RV- and NoV- infections alone (Supplementary Data S1 – Fig. 5).
Microbiome composition and clinical manifestations in mixed infections with EPEC
In RV + EPEC mixed-infection group, children with high Streptococcus abundance had adverse condition of vomiting and diarrhea, reaching approximately 7–8 times per day. Only children infected with Escherichia were admitted and hospitalized for more than a day. Similar to our observation with EAEC mixed infection, and in comparison with RV + EPEC infected group, NoV + EPEC mixed-infections resulted in substantial decrease in genus Bacteroides as well as Bifidobacterium (Supplementary Data S1 – Fig. 6). Importantly, phyla Chlorobi, which was observed absent in RV- alone group, was significantly abundant RV + EPEC mixed infections, but absent in NoV + EPEC. Conversely, phyla Rubiaceae richness was observed only in NoV + EPEC, but absent in RV + EPEC. Furthermore, phyla Nitrospirae was particularly absent in RV- and NoV- mixed infections (Additional File 1).
Microbiome composition and clinical manifestations in RV vaccinated cohort
The number of children in RV cohort with one or two doses of vaccine represented about 27% and 34.1%, respectively. The most notable difference observed in RVV group with one dose was the abundance of Clostridium (1.05E-1) and E. coli (3.28E-1) compared to two doses vaccination. Microbial composition at phylum level denoted higher levels of Firmicutes in both vaccinated and non-vaccinated children. Two doses vaccination in children resulted in decrease in Bacteroidetes compared to one dose or non-vaccinated. When comparing total number of bacteria genera as a whole, RVV vaccinated children either with one or two doses of vaccine, showed less abundance of bacterial genera compared to non-vaccinated children (Supplementary Data S1 - Figs 4–6).
Discussion
Few studies have evaluated the microbiota of children suffering from enteric viral infection[26](/articles/s41598-018-37162-w#ref-CR26 "Nelson, A. M. et al. Disruption of the Human Gut Microbiota following Norovirus Infection. PLOS ONE 7, e48224, https://doi.org/10.1371/journal.pone.0048224
(2012)."), severe and complicated AGE[24](/articles/s41598-018-37162-w#ref-CR24 "Chen, S. Y. et al. Intestinal microbiome in children with severe and complicated acute viral gastroenteritis. Sci Rep 7, 46130,
https://doi.org/10.1038/srep46130
(2017)."), and irritable bowel syndrome with diarrhea (IBS-D)[30](/articles/s41598-018-37162-w#ref-CR30 "Shankar, V., Reo, N. V. & Paliy, O. Simultaneous fecal microbial and metabolite profiling enables accurate classification of pediatric irritable bowel syndrome. Microbiome 3, 73,
https://doi.org/10.1186/s40168-015-0139-9
(2015)."). In the current study, we investigated the interplay between viral-bacterial mixed infections in children hospitalized with AGE by evaluating microbiome compositions and clinical outcomes in the studied populations. Our study focused on two major viruses (RV and NoV) as well as two major pathogenic _E_. _coli_ (EAEC and EPEC) that are known to cause AGE in children. The number of samples evaluated in this study, especially in the viral infection groups, ensured sufficient statistical power in data analysis and interpretation as compared to previously published studies.We found that both, taxonomical composition and the diversity of gut microbiome, were disrupted or altered in children infected with single enteric virus, but the disruption was worsened with mixed viral-bacterial infections as compared to healthy controls. Moreover, reduction or richness of specific bacterial genera was linked to increased frequency of diarrhea, vomiting and fever, longer hospitalization and age, but not related to gender of the children (Supplementary Data S1 - Figs 4–6). We observed greater richness in bacterial genera in the RV infected group compared to NoV infected group (additional file 1), which is in contrast to recent study done by Chen et al. 2017[24](/articles/s41598-018-37162-w#ref-CR24 "Chen, S. Y. et al. Intestinal microbiome in children with severe and complicated acute viral gastroenteritis. Sci Rep 7, 46130, https://doi.org/10.1038/srep46130
(2017)."). According to their study, RV infection resulted in decreased microbiota diversity compared with NoV infection, which has not been reported previously. This difference might be attributed to the NoV samples included in their study. They enrolled children with complicated clinical conditions including convulsion, necrotizing enterocolitis, severe electrolyte imbalance and malnutrition. In addition, all fecal samples collected in that study were at least one week after discontinuation of the antibiotics. This could have severely altered the microbiome diversity in NoV infected children. Moreover, although the overall mean severity was higher in RV infected children in their study, the number of cases evaluated for the comparison was less \[RV (n = 5) and NoV (n = 15)\]. Additionally, Chen _et al_. study indicated that some of their children were administered antibiotics prior to confirmation of a viral infection, which could have drastically altered the gut microbiome.In comparison to gut microbiota in healthy controls, our results demonstrated that abundance of taxa Clostridiaceae and Streptococcaceae in the RV- and NoV-alone infected children had an adverse effect as measured by the increased severity of vomiting and diarrhea. In concordance with our findings, the abundance of these two bacteria was previously reported by Kersten et al.,198731 in a study that evaluated pediatric gastroenteritis in primary care and in hospitalized patients. This suggests that the growth of Clostridiaceae and Streptococcaceae may be promoted by disturbances in normal gut microflora, even in the absence of antibiotics use32,33; i.e., induced by gastroenteritis. Direct interaction of Clostridiaceae with the epithelial cells results in a cascade of inflammatory processes that can contribute to intestinal diseases such as diarrhea and pseudomembranous colitis34. Interestingly, the richness of Streptococcaceae was also observed with RV + EAEC infections, but the proportion of its richness declined in both RV + EPEC and RV + EPEC + EAEC mixed infections. Similar observations were noticed with NoV cohort, where Streptococcaceae richness was observed in mixed infections with EAEC compared EPEC. The association of Streptococcaceae with one E. coli type (EAEC) infection but not the other (EPEC), regardless of the viral infection, is an interesting observation that requires further assessment. Several other studies have also reported the abundance of the above taxa in other diseases including gastric mucosa-associated microbiota in dyspeptic patients[35](/articles/s41598-018-37162-w#ref-CR35 "Minalyan, A., Gabrielyan, L., Scott, D., Jacobs, J. & Pisegna, J. R. The Gastric and Intestinal Microbiome: Role of Proton Pump Inhibitors. Curr Gastroenterol Rep 19, 42, https://doi.org/10.1007/s11894-017-0577-6
(2017)."), cystic fibrosis[36](/articles/s41598-018-37162-w#ref-CR36 "Fouhy, F. et al. A pilot study demonstrating the altered gut microbiota functionality in stable adults with Cystic Fibrosis. Sci Rep 7, 6685,
https://doi.org/10.1038/s41598-017-06880-y
(2017)."), ulcerative colitis[37](/articles/s41598-018-37162-w#ref-CR37 "Ohkusa, T. & Koido, S. Intestinal microbiota and ulcerative colitis. Journal of Infection and Chemotherapy 21, 761–768,
https://doi.org/10.1016/j.jiac.2015.07.010
(2015).") and chronic rhinosinusitis (CRS)[38](/articles/s41598-018-37162-w#ref-CR38 "Cope, E. K., Goldberg, A. N., Pletcher, S. D. & Lynch, S. V. Compositionally and functionally distinct sinus microbiota in chronic rhinosinusitis patients have immunological and clinically divergent consequences. Microbiome 5, 53,
https://doi.org/10.1186/s40168-017-0266-6
(2017)."). Recently, efforts to engineer the microbiome to cure _Clostridioides difficile_ infections through fecal microbiota transplantation (FMT) has evolved[39](/articles/s41598-018-37162-w#ref-CR39 "Gianotti, R. J. & Moss, A. C. Fecal MicrobiotaTransplantation: From Clostridium difficile to Inflammatory Bowel Disease. Gastroenterology & Hepatology 13, 209–213 (2017)."). Being currently in the clinical trial, FMT may elucidate the factors that determine species-species interaction in the gut environment[39](/articles/s41598-018-37162-w#ref-CR39 "Gianotti, R. J. & Moss, A. C. Fecal MicrobiotaTransplantation: From Clostridium difficile to Inflammatory Bowel Disease. Gastroenterology & Hepatology 13, 209–213 (2017).").With respect to the difference in top genera by overall relative abundance of specific populations, our findings indicate that the populations of Prevotella and Ruminococcus were significantly increased in RV cohort compared NoV cohort. However, a recent study by Rodríguez-Díaz et al., 2017, specifically link the abundance of Ruminococcus to lower immunoglobulin A titers against both NoV and RV[40](/articles/s41598-018-37162-w#ref-CR40 "Rodriguez-Diaz, J. et al. Relevance of secretor status genotype and microbiota composition in susceptibility to rotavirus and norovirus infections in humans. Scientific Reports 7, https://doi.org/10.1038/srep45559
(2017)."). The occurrence of these bacteria in RV infected patients could also depend on other factors including host’s secretor status and RV genotype, as described for RV P type (P\[6\] and P\[8\]) variants[41](/articles/s41598-018-37162-w#ref-CR41 "Nordgren, J. et al. Both Lewis and secretor status mediate susceptibility to rotavirus infections in a rotavirus genotype-dependent manner. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America 59, 1567–1573,
https://doi.org/10.1093/cid/ciu633
(2014)."). On the other hand, population based studies have shown that _Prevotella_ and _Ruminococcus_ possess diagnostic values[42](/articles/s41598-018-37162-w#ref-CR42 "Gorvitovskaia, A., Holmes, S. P. & Huse, S. M. Interpreting Prevotella and Bacteroides as biomarkers of diet and lifestyle. Microbiome 4, 15,
https://doi.org/10.1186/s40168-016-0160-7
(2016)."), where abundance of _Prevotella_ has been associated with rural communities[43](/articles/s41598-018-37162-w#ref-CR43 "De Filippo, C. et al. Impact of diet in shaping gut microbiota revealed by a comparative study in children from Europe and rural Africa. Proceedings of the National Academy of Sciences of the United States of America 107, 14691–14696,
https://doi.org/10.1073/pnas.1005963107
(2010)."), non-Western[44](/articles/s41598-018-37162-w#ref-CR44 "Ou, J. et al. Diet, microbiota, and microbial metabolites in colon cancer risk in rural Africans and African Americans. The American journal of clinical nutrition 98, 111–120,
https://doi.org/10.3945/ajcn.112.056689
(2013).") and a plant-based diet[45](/articles/s41598-018-37162-w#ref-CR45 "Wu, G. D. et al. Linking long-term dietary patterns with gut microbial enterotypes. Science 334, 105–108,
https://doi.org/10.1126/science.1208344
(2011)."). These factors were not evaluated in our study and worth investigation in future work.RVV has been shown to substantially reduce morbidity and mortality among children worldwide. Previous studies suggest that the use of RVV reduce emergency department visits and hospitalizations of children with rotavirus acute gastroenteritis by 70% to 100%. Interestingly, substantial number of RV infected patients in our study had received one (n = 9) or two doses (n = 12) of the RV vaccine. We therefor sought of analyzing the effect of vaccine on microbiome composition in the different groups involved in this study. When comparing total number of bacteria genera as a whole, AGE-affected RV-vaccinated children either with one or two doses of vaccine showed slightly less abundance of bacterial genera compared to non-vaccinated children (Supplementary Data S1 - Figs 4–6). One-dose vaccination with RVV correlated with abundance to Clostridium and E. coli, similar to what has been reported in a recent study by Harris et al.[23](/articles/s41598-018-37162-w#ref-CR23 "Harris, V. et al. Rotavirus vaccine response correlates with the infant gut microbiota composition in Pakistan. Gut Microbes, 1–9, https://doi.org/10.1080/19490976.2017.1376162
(2017)."). In another study that investigated gut microbiome in RVV-responder and non-responders Ghanaian infants, bacteria belonging to the Bacteroidetes phylum, especially several bacteria related to species from the Bacteroides and Prevotella genera, were significantly associated with a lack of RVV response[22](/articles/s41598-018-37162-w#ref-CR22 "Harris, V. C. et al. Significant Correlation Between the Infant Gut Microbiome and Rotavirus Vaccine Response in Rural Ghana. J Infect Dis 215, 34–41,
https://doi.org/10.1093/infdis/jiw518
(2017)."),[46](/articles/s41598-018-37162-w#ref-CR46 "Atherly, D. et al. Rotavirus vaccination: cost-effectiveness and impact on child mortality in developing countries. J Infect Dis 200(Suppl 1), S28–38,
https://doi.org/10.1086/605033
(2009)."). None of the above studies, including ours, have looked at the RV genotype causing the infection, which could dramatically influence infection severity and consequently gut microbiome. Dietary and nutritional status of infants, history of chronic illness, mixed infections, and other factors could explain the discrepancies between the different studies. Although our study is the only one that evaluated mixed-infection effect on gut microbiota, the low number of patients in the mixed-infection groups did not enable valid statistical comparison between groups regarding vaccine effect.There was no abundance of specific genera that correlated with degree of dehydration in RV groups. However, genera Escherichia, Streptococcus, Rumella and Clostridium seemed to be specifically correlated with degree of dehydration in NoV groups (Supplemental Figs 3–4). Diarrhea and vomiting frequencies were worsened with EPEC mixed infections with both RV and NoV. This is in agreement with previous studies that reported persistent diarrhea in children with viral-EPEC mixed infections[47](/articles/s41598-018-37162-w#ref-CR47 "Tobias, J. et al. Involvement of main diarrheagenic Escherichia coli, with emphasis on enteroaggregative E. coli, in severe non-epidemic pediatric diarrhea in a high-income country. BMC Infectious Diseases 15, 79, https://doi.org/10.1186/s12879-015-0804-4
(2015)."),[48](/articles/s41598-018-37162-w#ref-CR48 "Langendorf, C. et al. Enteric Bacterial Pathogens in Children with Diarrhea in Niger: Diversity and Antimicrobial Resistance. PloS one 10, e0120275,
https://doi.org/10.1371/journal.pone.0120275
(2015)."), where EPEC is known to be the most common cause of acute diarrhea and may also cause persistent diarrhea in children[49](/articles/s41598-018-37162-w#ref-CR49 "Ochoa, T. J. & Contreras, C. A. Enteropathogenic E. coli (EPEC) infection in children. Current Opinion in Infectious Diseases 24, 478–483,
https://doi.org/10.1097/QCO.0b013e32834a8b8b
(2011)."). In our study, most of the children with EPEC mixed infections were admitted and hospitalized for more than a day. Coinfection with EPEC was associated with richness of bacteria _Rothia_, _Leptotrichia_, and _Haemophilus_ and poorness of genera _Lactobacillus_ and _Prevotella_ in both RV and NoV cohorts.On the other hand, children infected with RV/NoV-EAEC mixed infections showed an onset of AGE symptoms for more than 2–3 days prior to hospitalization and exhibited significant abundance in Escherichia. Coinfection with EAEC was associated with richness of bacteria genera Lachnospiraceae, Oscillospira, Faecalibacterium and unclassified. Triple infection with RV + EAEC + EPEC was associated with preponderance of bacterial genera Collinsella, Roseburia, and Sutterella.
Studies detailing viral-bacterial interplays and their effect on microbiome are limited and contradictory. Experimental studies in mice revealed exacerbated disturbance of gut microbiota in viral-bacterial mixed infections compared to single RV or NoV infections[50](/articles/s41598-018-37162-w#ref-CR50 "Howe, A. et al. Divergent responses of viral and bacterial communities in the gut microbiome to dietary disturbances in mice. The ISME Journal 10, 1217–1227, https://doi.org/10.1038/ismej.2015.183
(2016)."). In an earlier study, Hori _et al_. 1996, reported that rotavirus causes more severe gastroenteritis than bacteria or parasites in Ghanaian children[51](/articles/s41598-018-37162-w#ref-CR51 "Hori, H. et al. Enteric pathogens in severe forms of acute gastroenteritis in Ghanaian children. Acta Paediatr Jpn 38, 672–676 (1996)."). Another study from Bangladesh found that mixed RV and _E_. _coli_ infections were similar in severity to infections with _E_. _coli_ or RV alone[52](/articles/s41598-018-37162-w#ref-CR52 "Unicomb, L. E., Faruque, S. M., Malek, M. A., Faruque, A. S. & Albert, M. J. Demonstration of a lack of synergistic effect of rotavirus with other diarrheal pathogens on severity of diarrhea in children. J Clin Microbiol 34, 1340–1342 (1996)."). These results indicate that factors other than the enteric pathogens are responsible for disease manifestations. This partially includes gut microbiome, which is an important player in determining immune response to- and pathogenesis of GIT infection. Our study partially answer some of the questions, while many remained unanswered. A larger follow up study is needed to unveil the contribution of several others factors such as virus genotype, levels of virus replication, mixed infections with other pathogens, genetic makeup of the host and others. Expectedly, _Bacteroidaceae_ richness was significantly greater in healthy children as this microflora is known to maintain the physiologic conditions of the colon[53](/articles/s41598-018-37162-w#ref-CR53 "Knoll, R. L. et al. Gut microbiota differs between children with Inflammatory Bowel Disease and healthy siblings in taxonomic and functional composition: a metagenomic analysis. Am J Physiol-Gastr L 312, G327–G339,
https://doi.org/10.1152/ajpgi.00293.2016
(2017)."). On the other hand, reduction of relative numbers of _Bacteroides_ was reported in both RV and NoV infections, which was more prominent in the mixed infection with EPEC and EAEC. Reduced numbers of _Bacteroides_ have been reported earlier in stools from NoV-infected patients, which seems to have been more deteriorated in viral-bacterial mixed infection as the case in our study[26](/articles/s41598-018-37162-w#ref-CR26 "Nelson, A. M. et al. Disruption of the Human Gut Microbiota following Norovirus Infection. PLOS ONE 7, e48224,
https://doi.org/10.1371/journal.pone.0048224
(2012)."). Whether this reduction _Bacteroides_ is a consequence of infection, or a predisposition factor that facilitated the infection requires further investigations. Of note, certain _Bacteroidetes_ express a form of lipopolysaccharide (LPS) that is structurally and functionally different from the LPS expressed on _E_. _coli_[54](/articles/s41598-018-37162-w#ref-CR54 "Alexander, C. & Rietschel, E. T. Bacterial lipopolysaccharides and innate immunity. Journal of endotoxin research 7, 167–202 (2001)."). LPS is a strong immunogenic stimulator, present in the outer membrane of gram-negative bacteria[54](/articles/s41598-018-37162-w#ref-CR54 "Alexander, C. & Rietschel, E. T. Bacterial lipopolysaccharides and innate immunity. Journal of endotoxin research 7, 167–202 (2001)."). _Bacteroidetes_ LPS has been shown to inhibit innate immune signaling and endotoxin tolerance as compared with that of _E_. _coli_[55](/articles/s41598-018-37162-w#ref-CR55 "Vatanen, T. et al. Variation in Microbiome LPS Immunogenicity Contributes to Autoimmunity in Humans. Cell 165, 842–853,
https://doi.org/10.1016/j.cell.2016.04.007
(2016)."). This suggests that differences in microbiota-derived LPS may modulate aspects of immune education and play a role in determining susceptibility to immune diseases. Alternatively, _Bifidobacteriaceae_, which act as probiotics, seems to increase depending on the severity of the infections. That is, we observed an increase in _Bifidobacteriaceae_ richness in the viral-bacterial mixed infections compared to single viral infections (Fig. [1](/articles/s41598-018-37162-w#Fig1)). Studies have proven that the decrease in _Bifidobacteriaceae_ impairs the gastroenteritis homeostasis and may result in mucosal inflammation in the GI tract. In addition to _Lactobacillus_, strains belonging to _Bifidobacterium_, are widely used as probiotic bacteria and are included in many functional foods and dietary supplements[56](/articles/s41598-018-37162-w#ref-CR56 "Guarner, F. & Malagelada, J. R. Gut flora in health and disease. Lancet (London, England) 361, 512–519,
https://doi.org/10.1016/s0140-6736(03)12489-0
(2003)."),[57](/articles/s41598-018-37162-w#ref-CR57 "Gourbeyre, P., Denery, S. & Bodinier, M. Probiotics, prebiotics, and synbiotics: impact on the gut immune system and allergic reactions. J Leukoc Biol 89, 685–695,
https://doi.org/10.1189/jlb.1109753
(2011)."). These probiotics have been reported to suppress diarrhea[58](/articles/s41598-018-37162-w#ref-CR58 "Lye, H. S., Kuan, C. Y., Ewe, J. A., Fung, W. Y. & Liong, M. T. The improvement of hypertension by probiotics: effects on cholesterol, diabetes, renin, and phytoestrogens. Int J Mol Sci 10, 3755–3775,
https://doi.org/10.3390/ijms10093755
(2009)."), exhibit antimicrobial effect[59](/articles/s41598-018-37162-w#ref-CR59 "Karska-Wysocki, B., Bazo, M. & Smoragiewicz, W. Antibacterial activity of Lactobacillus acidophilus and Lactobacillus casei against methicillin-resistant Staphylococcus aureus (MRSA). Microbiol Res 165, 674–686,
https://doi.org/10.1016/j.micres.2009.11.008
(2010)."), prevent inflammatory bowel disease[60](/articles/s41598-018-37162-w#ref-CR60 "Golowczyc, M. A., Mobili, P., Garrote, G. L., Abraham, A. G. & De Antoni, G. L. Protective action of Lactobacillus kefir carrying S-layer protein against Salmonella enterica serovar Enteritidis. Int J Food Microbiol 118, 264–273,
https://doi.org/10.1016/j.ijfoodmicro.2007.07.042
(2007)."), and alleviate lactose intolerance and postoperative complications[61](/articles/s41598-018-37162-w#ref-CR61 "Pelletier, X., Laure-Boussuge, S. & Donazzolo, Y. Hydrogen excretion upon ingestion of dairy products in lactose-intolerant male subjects: importance of the live flora. European journal of clinical nutrition 55, 509–512,
https://doi.org/10.1038/sj.ejcn.1601169
(2001)."),[62](/articles/s41598-018-37162-w#ref-CR62 "Woodard, G. A. et al. Probiotics improve outcomes after Roux-en-Y gastric bypass surgery: a prospective randomized trial. Journal of gastrointestinal surgery: official journal of the Society for Surgery of the Alimentary Tract 13, 1198–1204,
https://doi.org/10.1007/s11605-009-0891-x
(2009)."). _Bifidobacterium_ and _Lactobacilli_ have been also shown to inhibit a wide range of pathogens, including _Helicobacter pylori_, _E_. _coli_, _Listeria monocytogenes_, _Salmonella_, and RV[63](#ref-CR63 "Furrie, E. et al. Synbiotic therapy (Bifidobacterium longum/Synergy 1) initiates resolution of inflammation in patients with active ulcerative colitis: a randomised controlled pilot trial. Gut 54, 242–249,
https://doi.org/10.1136/gut.2004.044834
(2005)."),[64](#ref-CR64 "Tsaia, C. C., Lin, P. P. & Hsieh, Y. M. Three Lactobacillus strains from healthy infant stool inhibit enterotoxigenic Escherichia coli grown in vitro. Anaerobe 14, 61–67,
https://doi.org/10.1016/j.anaerobe.2007.11.003
(2008)."),[65](#ref-CR65 "Nakamura, S. et al. Inhibitory effects of Leuconostoc mesenteroides 1RM3 isolated from narezushi, a fermented fish with rice, on Listeria monocytogenes infection to Caco-2 cells and A/J mice. Anaerobe 18, 19–24,
https://doi.org/10.1016/j.anaerobe.2011.11.006
(2012)."),[66](/articles/s41598-018-37162-w#ref-CR66 "Bermudez-Brito, M., Plaza-Díaz, J., Muñoz-Quezada, S., Gómez-Llorente, C. & Gil, A. Probiotic Mechanisms of Action. Annals of Nutrition and Metabolism 61, 160–174 (2012)."). Our results suggest that our body has evolved mechanisms to combat GIT disease by promoting probiotic bacteria growth over the aggression of pathogenic ones. Nonetheless, generalizations regarding the potential probiotic health benefits should not be made because they tend to be strain specific.Despite the differences in the age of children of each subgroup, we believe that this difference was not a confounder and it did not affect the microbiota composition. Although it has been suggested that the composition of bacterial communities evolve towards an adult-like configuration after 1–3 year of age, other studies showed that it continues to change until teenage years[10](/articles/s41598-018-37162-w#ref-CR10 "Hollister, E. B. et al. Structure and function of the healthy pre-adolescent pediatric gut microbiome. Microbiome 3, 36, https://doi.org/10.1186/s40168-015-0101-x
(2015)."). Moreover, having age-matched subgroups is difficult for such studies and here we present the first data set of results describing mixed infections effect on microbiome. We therefore believe that future studies with larger cohorts should count for age, gender, ethnicity, and other factors.Conclusion
We evaluated the bacterial composition in viral-bacterial AGE mixed infections in correlation with various clinical severities. Our results revealed that richness of Bifidobacteriaceae, which act as probiotics, increased with the severity of the viral-bacterial mixed infections. As expected, significant reduction of relative numbers of Bacteroides was characterized in both RV and NoV infection, in which was more prominent in mixed infections with pathogenic E. coli. Though EAEC mixed infection resulted in significant microbiota alterations compared to virus-alone or virus-EPEC mixed infection, the clinical conditions of the children was worsened with both E. coli virotypes. This could be attributed to the type of toxins secreted and mode of pathogenesis exerted by each type. However, this study did not look into the virulence factors exerted by each of the E. coli types on the gut microbial community, which mandates further investigations. Further, augmented number of differential abundant pathogenic OTUs was peculiarly noticed only with NoV mixed infection. Certain pathogenic commensal bacteria express carbohydrates indistinguishable from human histo-blood group antigen (HBGA) and NoV particles bind to these HBGA-expressing bacteria[67](/articles/s41598-018-37162-w#ref-CR67 "Karst, S. M. & Wobus, C. E. A Working Model of How Noroviruses Infect the Intestine. PLOS Pathogens 11, e1004626, https://doi.org/10.1371/journal.ppat.1004626
(2015)."). Interaction of NoV particles with HBGA-expressing bacteria further enhances infection of the host[67](/articles/s41598-018-37162-w#ref-CR67 "Karst, S. M. & Wobus, C. E. A Working Model of How Noroviruses Infect the Intestine. PLOS Pathogens 11, e1004626,
https://doi.org/10.1371/journal.ppat.1004626
(2015)."),[68](/articles/s41598-018-37162-w#ref-CR68 "Jones, M. K. et al. Enteric bacteria promote human and mouse norovirus infection of B cells. Science 346, 755–759,
https://doi.org/10.1126/science.1257147
(2014)."). Viral-bacterial interplay in the gut environment is a rather complicated process that involves multiple factors including host genetic makeup, host diet, host immune status, microbiome composition in addition to the infectious agents. Results from this study will facilitate further studies on the interaction between aforementioned factors.Methods
Ethical approvals
This study was approved by the institutional review board (IRB) committees at Hamad Medical Corporation (HMC) and Qatar University (QU). All samples were collected with informed consent signed from the parents/legal guardians under IRB approval from HMC (Approval # 16173/19) and exemption from QU (Approval # QU-IRB605-E/16). Samples were collected with information about age, nationality and clinical data, such as frequency and duration of vomiting, diarrhea, fever, severity of dehydration, and duration of hospitalization. All methods were performed in accordance with the relevant national and international guidelines and regulations.
Patient enrollment and sample collection
Samples from viral AGE affected children were collected from the Pediatric Emergency Center, Hamad Medical Coorporation, Doha, Qatar. Samples were screened for viral infections (group A RV and NoV), and bacterial infections (EPEC and EAEC) using the FilmArray Gastrointestinal (GI) Panel kit®, BioFire Diagnostics, United States. We evaluated the severity of gastroenteritis using the Vesikari score system69 with the following definitions: A score of 10–20 indicates severe gastroenteritis, 7 ≤ 10 indicate moderate, and <7 indicate mild illness. A total of 70 young children with confirmed AGE (RV = 18, RV + EAEC = 8, RV + EPEC = 10, RV + EPEC + EAEC = 5, NoV = 17, NoV + EAEC = 7 and NoV + EPEC = 5) along with nine healthy children (negative controls) were enrolled in our study. All the fecal specimens were processed with 10% glycerol, and stored at −80 °C for bacteria preservation.
Extraction and amplification of 16S rRNA
Total bacterial DNA was extracted using QIAamp UCP Pathogen Mini Kit (Qiagen, Hilden, Germany) according to the manufacturer’s recommendations by using Pathogen Lysis Tubes for efficient lysis of cells of gram negative and gram positive bacteria. Bacterial 16S rRNA genes were PCR-amplified with dual-barcoded primers targeting the V4 region, as per the protocol of Kozich et al.[29](/articles/s41598-018-37162-w#ref-CR29 "Kozich, J. J., Westcott, S. L., Baxter, N. T., Highlander, S. K. & Schloss, P. D. Development of a dual-index sequencing strategy and curation pipeline for analyzing amplicon sequence data on the MiSeq Illumina sequencing platform. Applied and environmental microbiology 79, 5112–5120, https://doi.org/10.1128/aem.01043-13
(2013)."). The PCR products were normalized, pooled and quantified before being denatured and spiked with PhiX DNA control, Illumina®, Unites States.Handling contamination
The potential for contamination was addressed by co-sequencing of the DNA amplified from specimens, and four template-free controls[29](/articles/s41598-018-37162-w#ref-CR29 "Kozich, J. J., Westcott, S. L., Baxter, N. T., Highlander, S. K. & Schloss, P. D. Development of a dual-index sequencing strategy and curation pipeline for analyzing amplicon sequence data on the MiSeq Illumina sequencing platform. Applied and environmental microbiology 79, 5112–5120, https://doi.org/10.1128/aem.01043-13
(2013)."). Two positive controls, consisting of cloned SUP05 DNA, were also included (number of copies = 2\*106). Operational Taxonomic Units (OTUs) were considered putative contaminants (and were removed) if their mean abundance in controls reached or exceeded 25% of their mean abundance in specimens.Illumina MiSeq sequencing
Amplicons were sequenced with an Illumina MiSeq using the 250-bp paired-end kit (v.2), Illumina®, Unites States. The resulted bacterial reads were distributed across the samples, to demonstrate uniform coverage and clustered with the mothur software package (v. 1.39.5)[70](/articles/s41598-018-37162-w#ref-CR70 "Schloss, P. D. et al. Introducing mothur: Open-Source, Platform-Independent, Community-Supported Software for Describing and Comparing Microbial Communities. Applied and environmental microbiology 75, 7537–7541, https://doi.org/10.1128/Aem.01541-09
(2009)."), following the recommended procedure[71](/articles/s41598-018-37162-w#ref-CR71 "Schloss., Mothur protocol,
https://www.mothur.org/wiki/MiSeq_SOP
(2018).").Microbiome data analysis
High quality reads were classified using Greengenes (v. 13_8) as the reference database. Alpha diversity was estimated with the Shannon index on raw OTU abundance tables after filtering out contaminants by using the mothur version of the Bayesian classifier[71](/articles/s41598-018-37162-w#ref-CR71 "Schloss., Mothur protocol, https://www.mothur.org/wiki/MiSeq_SOP
(2018)."). Positive correlation between relative abundance and prevalence was calculated using Spearman’s correlation coefficient. To estimate beta diversity across samples, we excluded OTUs occurring in fewer than 10% of the samples with a count of less than three and computed Bray-Curtis indices[72](/articles/s41598-018-37162-w#ref-CR72 "Weiss, S. et al. Normalization and microbial differential abundance strategies depend upon data characteristics. Microbiome 5, 27,
https://doi.org/10.1186/s40168-017-0237-y
(2017)."). We visualized beta diversity, emphasizing differences across samples, using non-metric multidimensional scaling (NMDS) ordination. Pairwise differences: post-hoc test was estimated to characterize the inter-individual differences between groups (beta-diversity) at the group level. Variation in community structure was assessed with permutational multivariate analyses of variance (PERMANOVA) with treatment group as the main fixed factor and using 4,999 permutations for significance testing. All analyses were conducted in the R environment. To determine which OTUs were driving the differences in microbial composition, we analyzed negative binomial Generalized Linear Models on each OTU with the DESeq. 2 R package (v. 1.19.1)[73](/articles/s41598-018-37162-w#ref-CR73 "Love, M. I., Huber, W. & Anders, S. Moderated estimation of fold change and dispersion for RNA-seq data with DESeq. 2. Genome Biol 15,
https://doi.org/10.1186/s13059-014-0550-8
(2014)."). Hypothesis testing was achieved with likelihood ratio tests. _P_\-values were adjusted using the Bonferroni correction (_p_\-values threshold = 0.05) and Benjamini-Hochberg procedure[74](/articles/s41598-018-37162-w#ref-CR74 "Shannon, C. E. The mathematical theory of communication. 1963. MD Comput 14, 306–317 (1997).").Data Availability
All the necessary data and materials are included in as supporting data and additional files.
References
- Arora, S. K., Dewan, P. & Gupta, P. Microbiome: Paediatricians’ perspective. Indian J Med Res 142, 515–524, https://doi.org/10.4103/0971-5916.171275 (2015).
Article CAS PubMed PubMed Central Google Scholar - Althani, A. A. et al. Human Microbiome and its Association With Health and Diseases. Journal of cellular physiology 231, 1688–1694, https://doi.org/10.1002/jcp.25284 (2016).
Article CAS PubMed Google Scholar - Bermon, S. et al. The microbiota: an exercise immunology perspective. Exerc Immunol Rev 21, 70–79 (2015).
PubMed Google Scholar - Flint, H. J., Scott, K. P., Louis, P. & Duncan, S. H. The role of the gut microbiota in nutrition and health. Nat Rev Gastroenterol Hepatol 9, 577–589, https://doi.org/10.1038/nrgastro.2012.156 (2012).
Article CAS PubMed Google Scholar - Nieuwdorp, M., Gilijamse, P. W., Pai, N. & Kaplan, L. M. Role of the microbiome in energy regulation and metabolism. Gastroenterology 146, 1525–1533, https://doi.org/10.1053/j.gastro.2014.02.008 (2014).
Article CAS PubMed Google Scholar - Reinhardt, C. et al. Tissue factor and PAR1 promote microbiota-induced intestinal vascular remodelling. Nature 483, 627–631, https://doi.org/10.1038/nature10893 (2012).
Article ADS CAS PubMed Google Scholar - Maruvada, P., Leone, V., Kaplan, L. M. & Chang, E. B. The Human Microbiome and Obesity: Moving beyond Associations. Cell Host Microbe 22, 589–599, https://doi.org/10.1016/j.chom.2017.10.005 (2017).
Article CAS PubMed Google Scholar - Reeves, A. E. et al. The interplay between microbiome dynamics and pathogen dynamics in a murine model of Clostridium difficile Infection. Gut Microbes 2, 145–158 (2011).
Article Google Scholar - Giongo, A. et al. Toward defining the autoimmune microbiome for type 1 diabetes. ISME J 5, 82–91, https://doi.org/10.1038/ismej.2010.92 (2011).
Article CAS PubMed Google Scholar - Hollister, E. B. et al. Structure and function of the healthy pre-adolescent pediatric gut microbiome. Microbiome 3, 36, https://doi.org/10.1186/s40168-015-0101-x (2015).
Article PubMed PubMed Central Google Scholar - Palmer, C., Bik, E. M., DiGiulio, D. B., Relman, D. A. & Brown, P. O. Development of the human infant intestinal microbiota. PLoS Biol 5, e177, https://doi.org/10.1371/journal.pbio.0050177 (2007).
Article CAS PubMed PubMed Central Google Scholar - Johnson, C. L. & Versalovic, J. The human microbiome and its potential importance to pediatrics. Pediatrics 129, 950–960, https://doi.org/10.1542/peds.2011-2736 (2012).
Article PubMed PubMed Central Google Scholar - Karmali, M. A. Infection by verocytotoxin-producing Escherichia coli. Clinical microbiology reviews 2, 15–38 (1989).
Article CAS Google Scholar - Shin, N. R., Whon, T. W. & Bae, J. W. Proteobacteria: microbial signature of dysbiosis in gut microbiota. Trends Biotechnol 33, 496–503, https://doi.org/10.1016/j.tibtech.2015.06.011 (2015).
Article CAS Google Scholar - Fletcher, S. M., McLaws, M.-L. & Ellis, J. T. Prevalence of Gastrointestinal Pathogens In Developed and Developing Countries: Systematic Review and Meta-Analysis. Journal of Public Health Research 2, 42–53, https://doi.org/10.4081/jphr.2013.e9 (2013).
Article PubMed PubMed Central Google Scholar - Chow, C. M., Leung, A. K. C. & Hon, K. L. Acute gastroenteritis: from guidelines to real life. Clinical and experimental gastroenterology 3, 97–112 (2010).
Article Google Scholar - do Carmo, G. M. I. et al. Decline in Diarrhea Mortality and Admissions after Routine Childhood Rotavirus Immunization in Brazil: A Time-Series Analysis. PLoS Medicine 8, e1001024, https://doi.org/10.1371/journal.pmed.1001024 (2011).
Article PubMed PubMed Central Google Scholar - Elliott, E. J. Acute gastroenteritis in children. BMJ 334, 35–40, https://doi.org/10.1136/bmj.39036.406169.80 (2007).
Article PubMed PubMed Central Google Scholar - CDC. Norovirus Worldwide, https://www.cdc.gov/norovirus/worldwide.html (2016).
- CDC. Burden of Norovirus Illness and Outbreaks, https://www.cdc.gov/norovirus/php/illness-outbreaks.html (2016).
- WHO. Immunization, Vaccines and Biologicals - Rotavirus, http://www.who.int/immunization/diseases/rotavirus/en/ (2016).
- Harris, V. C. et al. Significant Correlation Between the Infant Gut Microbiome and Rotavirus Vaccine Response in Rural Ghana. J Infect Dis 215, 34–41, https://doi.org/10.1093/infdis/jiw518 (2017).
Article CAS PubMed Google Scholar - Harris, V. et al. Rotavirus vaccine response correlates with the infant gut microbiota composition in Pakistan. Gut Microbes, 1–9, https://doi.org/10.1080/19490976.2017.1376162 (2017).
- Chen, S. Y. et al. Intestinal microbiome in children with severe and complicated acute viral gastroenteritis. Sci Rep 7, 46130, https://doi.org/10.1038/srep46130 (2017).
Article ADS CAS PubMed PubMed Central Google Scholar - Hand, T. W. et al. Acute gastrointestinal infection induces long-lived microbiota-specific T cell responses. Science 337, 1553–1556, https://doi.org/10.1126/science.1220961 (2012).
Article ADS CAS PubMed PubMed Central Google Scholar - Nelson, A. M. et al. Disruption of the Human Gut Microbiota following Norovirus Infection. PLOS ONE 7, e48224, https://doi.org/10.1371/journal.pone.0048224 (2012).
Article ADS CAS PubMed PubMed Central Google Scholar - Rosengaus, R. B., Zecher, C. N., Schultheis, K. F., Brucker, R. M. & Bordenstein, S. R. Disruption of the termite gut microbiota and its prolonged consequences for fitness. Applied and environmental microbiology 77, 4303–4312, https://doi.org/10.1128/aem.01886-10 (2011).
Article CAS PubMed PubMed Central Google Scholar - Schloss., MiSeq SOP, http://www.mothur.org/wiki/MiSeq_SOP (2013).
- Kozich, J. J., Westcott, S. L., Baxter, N. T., Highlander, S. K. & Schloss, P. D. Development of a dual-index sequencing strategy and curation pipeline for analyzing amplicon sequence data on the MiSeq Illumina sequencing platform. Applied and environmental microbiology 79, 5112–5120, https://doi.org/10.1128/aem.01043-13 (2013).
Article CAS PubMed PubMed Central Google Scholar - Shankar, V., Reo, N. V. & Paliy, O. Simultaneous fecal microbial and metabolite profiling enables accurate classification of pediatric irritable bowel syndrome. Microbiome 3, 73, https://doi.org/10.1186/s40168-015-0139-9 (2015).
Article PubMed PubMed Central Google Scholar - Nivenius, K., Blomberg, J., Hagander, B., Mardh, P. A. & Schalen, C. Pediatric gastroenteritis in primary care and in hospitalized patients. Scandinavian journal of primary health care 5, 41–45 (1987).
Article CAS Google Scholar - Knoop, F. C., Owens, M. & Crocker, I. C. Clostridium difficile: clinical disease and diagnosis. Clinical Microbiology Reviews 6, 251–265 (1993).
Article CAS Google Scholar - Falsen, E., Kaijser, B., Nehls, L., Nygren, B. & Svedhem, A. Clostridium difficile in relation to enteric bacterial pathogens. Journal of Clinical Microbiology 12, 297–300 (1980).
CAS PubMed PubMed Central Google Scholar - Holst, E., Helin, I. & Mardh, P. A. Recovery of Clostridium difficile from children. Scandinavian journal of infectious diseases 13, 41–45 (1981).
Article CAS Google Scholar - Minalyan, A., Gabrielyan, L., Scott, D., Jacobs, J. & Pisegna, J. R. The Gastric and Intestinal Microbiome: Role of Proton Pump Inhibitors. Curr Gastroenterol Rep 19, 42, https://doi.org/10.1007/s11894-017-0577-6 (2017).
Article PubMed PubMed Central Google Scholar - Fouhy, F. et al. A pilot study demonstrating the altered gut microbiota functionality in stable adults with Cystic Fibrosis. Sci Rep 7, 6685, https://doi.org/10.1038/s41598-017-06880-y (2017).
Article ADS CAS PubMed PubMed Central Google Scholar - Ohkusa, T. & Koido, S. Intestinal microbiota and ulcerative colitis. Journal of Infection and Chemotherapy 21, 761–768, https://doi.org/10.1016/j.jiac.2015.07.010 (2015).
Article PubMed Google Scholar - Cope, E. K., Goldberg, A. N., Pletcher, S. D. & Lynch, S. V. Compositionally and functionally distinct sinus microbiota in chronic rhinosinusitis patients have immunological and clinically divergent consequences. Microbiome 5, 53, https://doi.org/10.1186/s40168-017-0266-6 (2017).
Article PubMed PubMed Central Google Scholar - Gianotti, R. J. & Moss, A. C. Fecal MicrobiotaTransplantation: From Clostridium difficile to Inflammatory Bowel Disease. Gastroenterology & Hepatology 13, 209–213 (2017).
Google Scholar - Rodriguez-Diaz, J. et al. Relevance of secretor status genotype and microbiota composition in susceptibility to rotavirus and norovirus infections in humans. Scientific Reports 7, https://doi.org/10.1038/srep45559 (2017).
- Nordgren, J. et al. Both Lewis and secretor status mediate susceptibility to rotavirus infections in a rotavirus genotype-dependent manner. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America 59, 1567–1573, https://doi.org/10.1093/cid/ciu633 (2014).
Article CAS Google Scholar - Gorvitovskaia, A., Holmes, S. P. & Huse, S. M. Interpreting Prevotella and Bacteroides as biomarkers of diet and lifestyle. Microbiome 4, 15, https://doi.org/10.1186/s40168-016-0160-7 (2016).
Article PubMed PubMed Central Google Scholar - De Filippo, C. et al. Impact of diet in shaping gut microbiota revealed by a comparative study in children from Europe and rural Africa. Proceedings of the National Academy of Sciences of the United States of America 107, 14691–14696, https://doi.org/10.1073/pnas.1005963107 (2010).
Article ADS PubMed PubMed Central Google Scholar - Ou, J. et al. Diet, microbiota, and microbial metabolites in colon cancer risk in rural Africans and African Americans. The American journal of clinical nutrition 98, 111–120, https://doi.org/10.3945/ajcn.112.056689 (2013).
Article CAS PubMed PubMed Central Google Scholar - Wu, G. D. et al. Linking long-term dietary patterns with gut microbial enterotypes. Science 334, 105–108, https://doi.org/10.1126/science.1208344 (2011).
Article ADS CAS PubMed PubMed Central Google Scholar - Atherly, D. et al. Rotavirus vaccination: cost-effectiveness and impact on child mortality in developing countries. J Infect Dis 200(Suppl 1), S28–38, https://doi.org/10.1086/605033 (2009).
Article PubMed Google Scholar - Tobias, J. et al. Involvement of main diarrheagenic Escherichia coli, with emphasis on enteroaggregative E. coli, in severe non-epidemic pediatric diarrhea in a high-income country. BMC Infectious Diseases 15, 79, https://doi.org/10.1186/s12879-015-0804-4 (2015).
Article PubMed PubMed Central Google Scholar - Langendorf, C. et al. Enteric Bacterial Pathogens in Children with Diarrhea in Niger: Diversity and Antimicrobial Resistance. PloS one 10, e0120275, https://doi.org/10.1371/journal.pone.0120275 (2015).
Article CAS PubMed PubMed Central Google Scholar - Ochoa, T. J. & Contreras, C. A. Enteropathogenic E. coli (EPEC) infection in children. Current Opinion in Infectious Diseases 24, 478–483, https://doi.org/10.1097/QCO.0b013e32834a8b8b (2011).
Article PubMed PubMed Central Google Scholar - Howe, A. et al. Divergent responses of viral and bacterial communities in the gut microbiome to dietary disturbances in mice. The ISME Journal 10, 1217–1227, https://doi.org/10.1038/ismej.2015.183 (2016).
Article CAS PubMed Google Scholar - Hori, H. et al. Enteric pathogens in severe forms of acute gastroenteritis in Ghanaian children. Acta Paediatr Jpn 38, 672–676 (1996).
Article CAS Google Scholar - Unicomb, L. E., Faruque, S. M., Malek, M. A., Faruque, A. S. & Albert, M. J. Demonstration of a lack of synergistic effect of rotavirus with other diarrheal pathogens on severity of diarrhea in children. J Clin Microbiol 34, 1340–1342 (1996).
CAS PubMed PubMed Central Google Scholar - Knoll, R. L. et al. Gut microbiota differs between children with Inflammatory Bowel Disease and healthy siblings in taxonomic and functional composition: a metagenomic analysis. Am J Physiol-Gastr L 312, G327–G339, https://doi.org/10.1152/ajpgi.00293.2016 (2017).
Article Google Scholar - Alexander, C. & Rietschel, E. T. Bacterial lipopolysaccharides and innate immunity. Journal of endotoxin research 7, 167–202 (2001).
CAS PubMed Google Scholar - Vatanen, T. et al. Variation in Microbiome LPS Immunogenicity Contributes to Autoimmunity in Humans. Cell 165, 842–853, https://doi.org/10.1016/j.cell.2016.04.007 (2016).
Article CAS PubMed PubMed Central Google Scholar - Guarner, F. & Malagelada, J. R. Gut flora in health and disease. Lancet (London, England) 361, 512–519, https://doi.org/10.1016/s0140-6736(03)12489-0 (2003).
Article Google Scholar - Gourbeyre, P., Denery, S. & Bodinier, M. Probiotics, prebiotics, and synbiotics: impact on the gut immune system and allergic reactions. J Leukoc Biol 89, 685–695, https://doi.org/10.1189/jlb.1109753 (2011).
Article CAS PubMed Google Scholar - Lye, H. S., Kuan, C. Y., Ewe, J. A., Fung, W. Y. & Liong, M. T. The improvement of hypertension by probiotics: effects on cholesterol, diabetes, renin, and phytoestrogens. Int J Mol Sci 10, 3755–3775, https://doi.org/10.3390/ijms10093755 (2009).
Article CAS PubMed PubMed Central Google Scholar - Karska-Wysocki, B., Bazo, M. & Smoragiewicz, W. Antibacterial activity of Lactobacillus acidophilus and Lactobacillus casei against methicillin-resistant Staphylococcus aureus (MRSA). Microbiol Res 165, 674–686, https://doi.org/10.1016/j.micres.2009.11.008 (2010).
Article PubMed Google Scholar - Golowczyc, M. A., Mobili, P., Garrote, G. L., Abraham, A. G. & De Antoni, G. L. Protective action of Lactobacillus kefir carrying S-layer protein against Salmonella enterica serovar Enteritidis. Int J Food Microbiol 118, 264–273, https://doi.org/10.1016/j.ijfoodmicro.2007.07.042 (2007).
Article CAS PubMed Google Scholar - Pelletier, X., Laure-Boussuge, S. & Donazzolo, Y. Hydrogen excretion upon ingestion of dairy products in lactose-intolerant male subjects: importance of the live flora. European journal of clinical nutrition 55, 509–512, https://doi.org/10.1038/sj.ejcn.1601169 (2001).
Article CAS PubMed Google Scholar - Woodard, G. A. et al. Probiotics improve outcomes after Roux-en-Y gastric bypass surgery: a prospective randomized trial. Journal of gastrointestinal surgery: official journal of the Society for Surgery of the Alimentary Tract 13, 1198–1204, https://doi.org/10.1007/s11605-009-0891-x (2009).
Article Google Scholar - Furrie, E. et al. Synbiotic therapy (Bifidobacterium longum/Synergy 1) initiates resolution of inflammation in patients with active ulcerative colitis: a randomised controlled pilot trial. Gut 54, 242–249, https://doi.org/10.1136/gut.2004.044834 (2005).
Article CAS PubMed PubMed Central Google Scholar - Tsaia, C. C., Lin, P. P. & Hsieh, Y. M. Three Lactobacillus strains from healthy infant stool inhibit enterotoxigenic Escherichia coli grown in vitro. Anaerobe 14, 61–67, https://doi.org/10.1016/j.anaerobe.2007.11.003 (2008).
Article CAS Google Scholar - Nakamura, S. et al. Inhibitory effects of Leuconostoc mesenteroides 1RM3 isolated from narezushi, a fermented fish with rice, on Listeria monocytogenes infection to Caco-2 cells and A/J mice. Anaerobe 18, 19–24, https://doi.org/10.1016/j.anaerobe.2011.11.006 (2012).
Article PubMed Google Scholar - Bermudez-Brito, M., Plaza-Díaz, J., Muñoz-Quezada, S., Gómez-Llorente, C. & Gil, A. Probiotic Mechanisms of Action. Annals of Nutrition and Metabolism 61, 160–174 (2012).
Article CAS Google Scholar - Karst, S. M. & Wobus, C. E. A Working Model of How Noroviruses Infect the Intestine. PLOS Pathogens 11, e1004626, https://doi.org/10.1371/journal.ppat.1004626 (2015).
Article CAS PubMed PubMed Central Google Scholar - Jones, M. K. et al. Enteric bacteria promote human and mouse norovirus infection of B cells. Science 346, 755–759, https://doi.org/10.1126/science.1257147 (2014).
Article ADS CAS PubMed PubMed Central Google Scholar - Vesikari, T., Rautanen, T., Varis, T., Beards, G. M. & Kapikian, A. Z. Rhesus Rotavirus candidate vaccine. Clinical trial in children vaccinated between 2 and 5 months of age. American journal of diseases of children (1960) 144, 285–289 (1990).
Article CAS Google Scholar - Schloss, P. D. et al. Introducing mothur: Open-Source, Platform-Independent, Community-Supported Software for Describing and Comparing Microbial Communities. Applied and environmental microbiology 75, 7537–7541, https://doi.org/10.1128/Aem.01541-09 (2009).
Article CAS PubMed PubMed Central Google Scholar - Schloss., Mothur protocol, https://www.mothur.org/wiki/MiSeq_SOP (2018).
- Weiss, S. et al. Normalization and microbial differential abundance strategies depend upon data characteristics. Microbiome 5, 27, https://doi.org/10.1186/s40168-017-0237-y (2017).
Article PubMed PubMed Central Google Scholar - Love, M. I., Huber, W. & Anders, S. Moderated estimation of fold change and dispersion for RNA-seq data with DESeq. 2. _Genome Bio_l 15, https://doi.org/10.1186/s13059-014-0550-8 (2014).
- Shannon, C. E. The mathematical theory of communication. 1963. MD Comput 14, 306–317 (1997).
CAS PubMed Google Scholar
Acknowledgements
We would like to thank all the staff in Pediatric Emergency Centre-Hamad Medical Coorporation that helped in samples and data collection. We also thank Vineetha C. David for her contribution. This work was supported by internal funds from the Biomedical Research Center of Qatar University and funds from Qatar National Research Fund (QNRF), grant #NPRP9-133-1-025.
Author information
Authors and Affiliations
- Biomedical Research Center, Qatar University, Doha, 2713, Qatar
Shilu Mathew, Maria K. Smatti, Gheyath K. Nasrallah, Asmaa A. Al Thani & Hadi M. Yassine - Pediatric Emergency Center, Hamad Medical Corporation, Doha, 3050, Qatar
Khalid Al Ansari - Department of Biomedical Science, College of Health Science, Qatar University, Doha, 2713, Qatar
Gheyath K. Nasrallah, Asmaa A. Al Thani & Hadi M. Yassine
Authors
- Shilu Mathew
- Maria K. Smatti
- Khalid Al Ansari
- Gheyath K. Nasrallah
- Asmaa A. Al Thani
- Hadi M. Yassine
Contributions
Conceived and designed the experiments: H.M.Y. Performed the experiments: S.M.M. Analyzed the data: S.M.M., M.K.S. and H.M.Y. Contributed reagents/materials/analysis tools: H.M.Y., M.K.S., K.A.A., G.K.N., A.A.T. Wrote the manuscript: S.M.M., M.K.S., G.K.N., A.A.T., H.M.Y.
Corresponding author
Correspondence toHadi M. Yassine.
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article
Cite this article
Mathew, S., Smatti, M.K., Al Ansari, K. et al. Mixed Viral-Bacterial Infections and Their Effects on Gut Microbiota and Clinical Illnesses in Children.Sci Rep 9, 865 (2019). https://doi.org/10.1038/s41598-018-37162-w
- Received: 18 May 2018
- Accepted: 29 November 2018
- Published: 29 January 2019
- Version of record: 29 January 2019
- DOI: https://doi.org/10.1038/s41598-018-37162-w