Gastroesophageal Reflux Disease: Practice Essentials, Background, Anatomy (original) (raw)
Practice Essentials
Gastroesophageal reflux disease occurs when the amount of gastric juice that refluxes into the esophagus exceeds the normal limit, causing symptoms with or without associated esophageal mucosal injury (ie, esophagitis; see the image below).
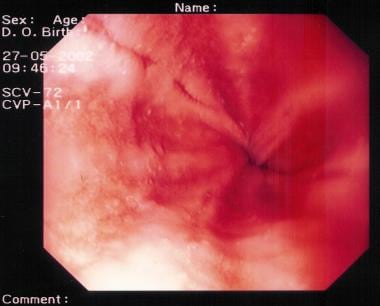
Gastroesophageal Reflux Disease. This image demonstrates peptic esophagitis.
Signs and symptoms
Typical esophageal symptoms include the following:
- Heartburn
- Regurgitation
- Dysphagia
Abnormal reflux can cause atypical (extraesophageal) symptoms, such as the following:
- Coughing and/or wheezing
- Hoarseness, sore throat
- Otitis media
- Noncardiac chest pain
- Enamel erosion or other dental manifestations
A history of nausea, vomiting, or regurgitation should alert the physician to evaluate for delayed gastric emptying.
See Presentation for more detail.
Diagnosis
Testing
The following studies are used to evaluate patients with suspected gastroesophageal reflux disease:
- Upper gastrointestinal endoscopy/esophagogastroduodenoscopy: Mandatory
- Esophageal manometry: Mandatory
- Ambulatory 24-hour pH monitoring: Criterion standard in establishing a diagnosis of gastroesophageal reflux disease
Imaging studies
Upper gastrointestinal contrast-enhanced studies are the initial radiologic procedure of choice in the workup gastroesophageal reflux disease. Plain chest radiographic findings are not useful in the evaluation of this condition, but they are helpful in assessing the pulmonary status and basic anatomy. Chest images may also demonstrate a large hiatal hernia, but small hernias can be easily missed.
Currently, no role exists for computed tomography scanning, magnetic resonance imaging, or ultrasonography in the routine evaluation of patients with reflux disease.
See Workup for more detail.
Management
Treatment of gastroesophageal reflux disease involves a stepwise approach. The goals are to control symptoms, to heal esophagitis, and to prevent recurrent esophagitis or other complications. The treatment is based on lifestyle modifications and control of gastric acid secretion through medical therapy with antacids or proton pump inhibitors or surgical treatment with corrective antireflux surgery. [1, 2, 3, 4, 5, 6]
Nonpharmacotherapy
Lifestyle modifications used in the management of gastroesophageal reflux disease include the following:
- Losing weight (if overweight)
- Avoiding alcohol, chocolate, citrus juice, and tomato-based products
- Avoiding peppermint, coffee, and possibly the onion family [7]
- Eating small, frequent meals rather than large meals
- Waiting 3 hours after a meal to lie down
- Refraining from ingesting food (except liquids) within 3 hours of bedtime
- Elevating the head of the bed by 8 inches
- Avoiding bending or stooping positions
Pharmacotherapy
The following medications are used in the management of gastroesophageal reflux disease:
- H2 receptor antagonists (eg, cimetidine, famotidine, nizatidine)
- Proton pump inhibitors (eg, omeprazole, lansoprazole, rabeprazole, esomeprazole, pantoprazole)
- Potassium-competitive acid blockers (eg, vonoprazan)
- Prokinetic agents (eg, metoclopramide)
- Antacids (eg, aluminum hydroxide, magnesium hydroxide)
Surgical options
Transthoracic and transabdominal fundoplications are performed for gastroesophageal reflux disease, including partial (anterior or posterior) and circumferential wraps. Open and laparoscopic techniques may be used.
Placement of a device to augment the lower esophageal sphincter is another surgical option.
Indications for fundoplication include the following:
- Patients with symptoms that are not completely controlled by proton pump inhibitors
- Patients with well-controlled reflux disease who desire definitive, one-time treatment
- The presence of Barrett esophagus
- The presence of extraesophageal manifestations
- Young patients
- Poor patient compliance with medications
- Postmenopausal women with osteoporosis
- Patients with cardiac conduction defects
- Cost of medical therapy
See Treatment and Medication for more detail.
![]()
Background
Gastroesophageal reflux is a normal physiologic phenomenon experienced intermittently by most people, particularly after a meal. Gastroesophageal reflux disease (GERD) occurs when the amount of gastric juice that refluxes into the esophagus exceeds the normal limit, causing symptoms with or without associated esophageal mucosal injury (ie, esophagitis).
A study by Richter and a Gallup Organization National Survey estimated that 25%-40% of healthy adult Americans experience symptomatic GERD, most commonly manifested clinically by pyrosis (heartburn), at least once a month. Furthermore, approximately 7%-10% of the adult population in the United States experiences such symptoms on a daily basis. [8, 9] (See Epidemiology.)
In most persons with GERD, endogenous defense mechanisms either limit the amount of noxious material that is introduced into the esophagus or rapidly clear the material from the esophagus so that symptoms and esophageal mucosal irritation are minimized. Examples of the defense mechanisms include actions of the lower esophageal sphincter (LES) and normal esophageal motility. When the defense mechanisms are defective or become overwhelmed so that the esophagus is bathed in acid or bile and acid-containing fluid for prolonged periods, GERD can be said to exist. (See Pathophysiology.)
Patients with GERD can exhibit various symptoms, both typical and atypical. Typical symptoms include heartburn, regurgitation, and dysphagia. Atypical symptoms include noncardiac chest pain, asthma, pneumonia, hoarseness, and aspiration. [10, 11] Patients typically have numerous daily episodes of symptomatic reflux, including pyrosis, water brash or sour taste in the mouth, nighttime coughing or aspiration, pneumonia or pneumonitis, bronchospasm, and laryngitis and voice changes, including hoarseness. In addition, objective evidence of esophageal damage can be seen on esophagogastroduodenoscopy as manifested by the incremental grades of esophagitis discussed below. (See Presentation.)
Laboratory tests are seldom useful in establishing a diagnosis of GERD. Esophageal manometry and pH monitoring are considered essential before performing an antireflux operation. Endoscopy reveals that 50% of patients do not have esophagitis. The only way to determine if abnormal reflux is present and if symptoms are actually caused by gastroesophageal reflux is through pH monitoring. Achalasia can present with heartburn. Only esophageal manometry and pH monitoring can be used to distinguish achalasia from GERD. Therapy is completely different for the two conditions. (See Workup.)
GERD is treated via a stepwise approach that is based on lifestyle modifications and control of gastric secretion by means of medical or surgical treatment. [1, 2, 3, 4, 5, 6] (See Treatment.)
GI disorders are some of the most frequent complaints during pregnancy, and gastroesophageal reflux is among these complaints. Some women have certain GI disorders that are unique to pregnancy, and others have chronic GI disorders that require special consideration during pregnancy. Understanding the presentation and prevalence of various GI disorders is necessary in order to optimize care for these patients.
For patient education resources, see Heartburn and GERD Center, as well as Acid Reflux (GERD), GERD FAQs (Gastroesophageal Acid Reflux), and GERD and Heartburn Medications.
![]()
Anatomy
The anatomy of the esophagus, stomach, and esophagogastric junction is critical in the understanding of the pathogenesis of reflux.
The esophagus is divided into three parts: cervical, thoracic, and abdominal. The body of the esophagus is made up of inner circular and outer longitudinal muscular layers. The proximal third of the esophagus is striated muscle, which transitions to smooth muscle in the distal two thirds. The proximal esophagus contains the upper esophageal sphincter (UES), which comprises the cricopharyngeus and thyropharyngeus muscles.
The distal thoracic esophagus is located on the left side of midline. As the thoracic esophagus enters the abdomen through the esophageal hiatus in the diaphragm, it becomes the abdominal esophagus. The hiatus is formed by the right crus of the diaphragm, which forms a sling around the esophagus with the right and left pillars, so that the esophagus narrows when the diaphragm contracts. [12, 13, 14] The actual contribution the diaphragm provides in maintaining an adequate length of intra-abdominal esophagus is not clearly understood; however, careful identification and approximation of the pillars during surgical treatment is crucial for preventing recurrence of reflux disease.
At this level, the phrenoesophageal ligament or membrane (see the image below), which is the reflection of the subdiaphragmatic fascia onto the transversalis fascia of the anterior abdominal wall, also encircles the esophagus. A prominent fat pad located on the anterior surface of the esophagus marks the lower limit of the phrenoesophageal ligament, which corresponds to the esophagogastric junction. This junction lies in the abdomen and forms the angle of His. The acute angle and the length of abdominal esophagus both contribute to the normal closure of the esophagus when intragastric and intra-abdominal pressures are high.
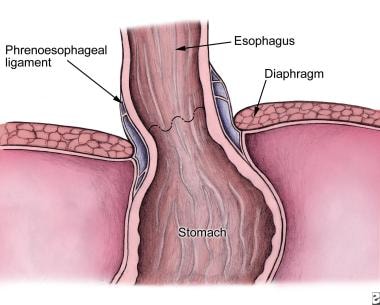
Gastroesophageal Reflux Disease. Relationship of the phrenoesophageal ligament to the diaphragm and esophagus.
The lower esophageal sphincter—or, more accurately, the distal esophageal high-pressure zone (HPZ)—is the distal most segment of the esophagus (3-5 cm in adults) and can be anywhere from 2-5 cm in length. Maintenance of an adequate intra-abdominal HPZ is crucial in preventing GERD. This HPZ does not correspond to any visible anatomic structure. It is a zone created by a complex architecture of smooth muscle fibers, and it is typically identified during manometry.
Usually, GERD is caused by a malfunction of one or more of these anatomic features. Proper surgical treatment requires complete preoperative and intraoperative evaluation and correction of all defective features.
Blood supply of esophagus and stomach
The blood supply of the esophagus is segmental (see the image below). The inferior thyroid artery supplies the cervical esophagus. Branches of the bronchial arteries and branches directly off of the aorta supply the proximal and distal thoracic esophagus, respectively. Finally, branches of the left gastric and inferior phrenic artery supply the abdominal esophagus. A relatively constant branch connects the left gastric and inferior phrenic arteries, called the Belsey artery.
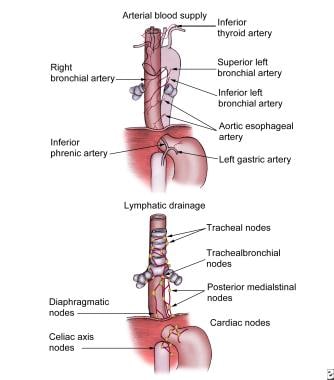
Gastroesophageal Reflux Disease. Arterial blood supply and lymphatic drainage of the esophagus.
The blood supply of the stomach is rich, with overlap among the vessels. The lesser curve is supplied by the left and right gastric arteries, branches of the celiac trunk and hepatic artery, respectively. The greater curve is supplied by the right gastroepiploic artery arising from the gastroduodenal artery and the left gastroepiploic artery and the short gastric arteries originating from the splenic artery. This excellent collateral blood supply of the stomach allows the surgeon to ligate much of the arterial supply (ie, the short gastric arteries during fundoplication) without the risk of ischemia (see the image above).
![]()
Pathophysiology
Schematically, the esophagus, lower esophageal sphincter (LES), and stomach can be envisioned as a simple plumbing circuit as described by Stein and coworkers. [15] The esophagus functions as an antegrade pump, the LES as a valve, and the stomach as a reservoir. The abnormalities that contribute to GERD can stem from any component of the system. Poor esophageal motility decreases clearance of acidic material. A dysfunctional LES allows reflux of large amounts of gastric juice. Delayed gastric emptying can increase the volume and pressure in the reservoir until the valve mechanism is defeated, leading to GERD. From a medical or surgical standpoint, it is extremely important to identify which of these components is defective so that an effective therapy can be applied.
Esophageal defense mechanisms
Esophageal defense mechanisms can be broken down into two categories (ie, esophageal clearance and mucosal resistance). Proper esophageal clearance is an extremely important factor in preventing mucosal injury. Esophageal clearance must be able to neutralize the acid refluxed through the lower esophageal sphincter. (Mechanical clearance is achieved by esophageal peristalsis; chemical clearance is achieved with saliva.) Normal clearance limits the amount of time the esophagus is exposed to refluxed acid or bile and gastric acid mixtures. Abnormal peristalsis can cause inefficient and delayed acid clearance.
Whether peristaltic dysfunction is secondary to esophageal exposure to acids or a primary defect is not understood clearly. In a review by Kahrilas et al, peristaltic dysfunction was progressively more common in patients with greater degrees of esophagitis. [16] Abnormal peristalsis was identified in 25% of patients with mild esophagitis and 48% of patients with severe esophagitis.
Buttar and associates described the importance of esophageal mucosal resistance as a protective mechanism. [17] They classified the factors into pre-epithelial, epithelial, and postepithelial defenses. When the defenses fail, esophagitis and other complications of reflux disease arise.
Dysfunction of the lower esophageal sphincter
The lower esophageal sphincter (LES) is defined by manometry as a zone of elevated intraluminal pressure at the esophagogastric junction. For proper LES function, this junction must be located in the abdomen so that the diaphragmatic crura can assist the action of the LES, thus functioning as an extrinsic sphincter. In addition, the LES must have a normal length and pressure and a normal number of episodes of transient relaxation (relaxation in the absence of swallowing).
LES dysfunction occurs via one of several mechanisms: transient relaxation of the LES (most common mechanism), permanent LES relaxation, and transient increase of intra-abdominal pressure that overcomes the LES pressure.
Delayed gastric emptying
The postulated mechanism by which delayed gastric emptying may cause GERD is an increase in the gastric contents resulting in increased intragastric pressure and, ultimately, increased pressure against the lower esophageal sphincter. This pressure eventually defeats the LES and leads to reflux. However, objective studies have produced conflicting data regarding the role of delayed gastric emptying in the pathogenesis of GERD.
Hiatal hernia
When discussing the mechanisms for GERD, the issue of hiatal hernia must be addressed. Hiatal hernias can be encountered frequently in patients with reflux disease; however, it has been well proven that not all patients with hiatal hernias have symptomatic reflux.
Buttar and coworkers state that a hiatal hernia may contribute to reflux via a variety of mechanisms. [17] (See the image below). The lower esophageal sphincter may migrate proximally into the chest and lose its abdominal high-pressure zone (HPZ), or the length of the HPZ may decrease. The diaphragmatic hiatus may be widened by a large hernia, which impairs the ability of the crura to function as an external sphincter. Finally, gastric contents may be trapped in the hernial sac and reflux proximally into the esophagus during relaxation of the LES. Reduction of the hernias and crural closure are critical to restoring an adequate intra-abdominal length of esophagus and recreating the HPZ.
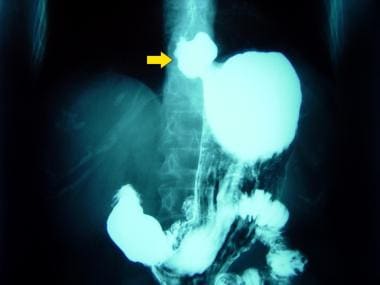
Gastroesophageal Reflux Disease. This radiograph shows a hiatal hernia.
Obesity as contributing factor
Some studies have shown that GERD is highly prevalent in patients who are morbidly obese and that a high body mass index (BMI) is a risk factor for the development of this condition. [18, 19, 20, 21, 22, 23] The hypothesis that obesity increases esophageal acid exposure is supported by the documentation of a dose-response relationship between increased BMI and increased prevalence of GERD and its complications. Therefore, the pathophysiology of GERD in patients who are morbidly obese might differ from that of patients who are not obese. The therapeutic implication of such a premise is that the correction of reflux in patients who are morbidly obese might be better achieved with a procedure that first controls obesity.
The mechanism by which a high BMI increases esophageal acid exposure is not completely understood. Increased intragastric pressure and gastroesophageal pressure gradient, incompetence of the lower esophageal sphincter (LES), and increased frequency of transient LES relaxations may all play a role in the pathophysiology of GERD in patients who are morbidly obese.
![]()
Etiology
Excessive retrograde movement of acid-containing gastric secretions or bile and acid-containing secretions from the duodenum and stomach into the esophagus is the etiologic effector of GERD. From a therapeutic point of view, informing patients that gastric refluxate is made up not only of acid but also of duodenal contents (eg, bile, pancreatic secretions) is important.
A functional (frequent transient LES relaxation) or mechanical (hypotensive LES) problem of the LES is the most common cause of GERD. Transient relaxation of the LES can be caused by foods (coffee, alcohol, chocolate, fatty meals), medications (beta-agonists, [24] nitrates, calcium channel blockers, anticholinergics), hormones (eg, progesterone), and nicotine.
![]()
Epidemiology
Western dietary habits have made GERD a common disease. The prevalence of GERD in Western populations is estimated to be 10-20%, whereas it is about 2.5-17.0% in Asian populations. [25]
Richter and associates reported that 25%-40% of Americans experience symptomatic GERD at some point. [19] Approximately 7%-10% of Americans experience symptoms of GERD on a daily basis. Because many individuals control their symptoms with over-the-counter (OTC) medications and without consulting a medical professional, the actual number of individuals with GERD is probably higher.
No sexual predilection exists: GERD is as common in men as in women. However, the male-to-female incidence ratio for esophagitis is 2:1-3:1. The male-to-female incidence ratio for Barrett esophagus is 10:1. White males are at a greater risk for Barrett esophagus and adenocarcinoma than other populations.
GERD occurs in all age groups. The prevalence of GERD increases in people older than 40 years.
![]()
Prognosis
Most patients with GERD do well with medications, although a relapse after cessation of medical therapy is common and indicates the need for long-term maintenance therapy.
Identifying the subgroup of patients who may develop the most serious complications of GERD and treating them aggressively is important. Surgery at an early stage is most likely indicated in these patients. After a laparoscopic Nissen fundoplication, symptoms resolve in approximately 92% of patients.
The LOTUS trial—a 5-year, exploratory randomized, open, parallel-group trial—demonstrated that with antireflux therapy for GERD, either using drug-induced acid suppression with esomeprazole or laparoscopic antireflux surgery, most patients achieve remission and remain in remission at 5 years. [26]
Most cases of gastroesophageal reflux in infants and very young children are benign and respond to conservative nonpharmacologic treatment (developmental disabilities represent an important diagnostic exception); 80% resolve by age 18 months (55% resolve by age 10 mo). Some patients require a "step-up" to acid-reducing medications, and only a very small minority require surgery. Because symptomatic gastroesophageal reflux after age 18 months likely represents a chronic condition, long-term risks are increased. For patients whose gastroesophageal reflux persists into later childhood, long-term therapy with antisecretory agents is often required.
In refractory cases or when complications related to reflux disease are identified (eg, stricture, aspiration, airway disease, Barrett esophagus), surgical treatment (fundoplication) is typically necessary. The prognosis with surgery is considered excellent. The surgical morbidity and mortality is higher in patients who have complex medical problems in addition to gastroesophageal reflux.
Complications of disease
Esophagitis
Esophagitis (esophageal mucosal damage) is the most common complication of GERD, occurring in approximately 50% of patients (see the images below).
Gastroesophageal Reflux Disease. This image demonstrates peptic esophagitis.

Gastroesophageal Reflux Disease. Reflux esophagitis is demonstrated on barium esophagram.
Esophagitis may be diagnosed using endoscopy, although it cannot always be appreciated on endoscopy. As many as 50% of symptomatic patients with GERD demonstrate no evidence of esophagitis on endoscopy. Still, documentation of this complication is important in diagnosing GERD. Degrees of esophagitis are described by the Savary-Miller classification as follows.
- Grade I – Erythema
- Grade II – Linear nonconfluent erosions
- Grade III – Circular confluent erosions
- Grade IV – Stricture or Barrett esophagus.
Stricture
Strictures are advanced forms of esophagitis and are caused by circumferential fibrosis due to chronic deep injury. Strictures can result in dysphagia and a short esophagus. Gastroesophageal reflux strictures typically occur in the mid-to-distal esophagus and can be visualized on upper GI tract studies and endoscopy. Presence of a stricture with a history of reflux can also help diagnose GERD. Patients present with dysphagia to solid meals and vomiting of nondigested foods.
As a rule, the presence of any esophageal stricture is an indication that the patient needs surgical consultation and treatment (usually surgical consultation). When patients present with dysphagia, barium esophagography is indicated to evaluate for possible stricture formation. In these cases, especially when associated with food impaction, eosinophilic esophagitis must be ruled out prior to attempting any mechanical dilatation of the narrowed esophageal region.
Barrett esophagus
The most serious complication of long-standing or severe GERD is the development of Barrett esophagus. Barrett esophagus is present in 8%-15% of patients with GERD. Barrett esophagus is thought to be caused by the chronic reflux of gastric juice into the esophagus. It is defined by metaplastic conversion of the normal distal squamous esophageal epithelium to columnar epithelium. Histologic examination of esophageal biopsy specimens is required to make the diagnosis. Varying degrees of dysplasia may be found on histologic examination.
Barrett esophagus with intestinal type metaplasia has malignant potential and is a risk factor for the development of esophageal adenocarcinoma (see the images below), increasing the risk of adenocarcinoma 30-40 times. The incidence of adenocarcinoma of the esophagus is increasing steadily in Western society. Currently, adenocarcinoma accounts for more than 50% of esophageal cancers in the Western industrialized nations.
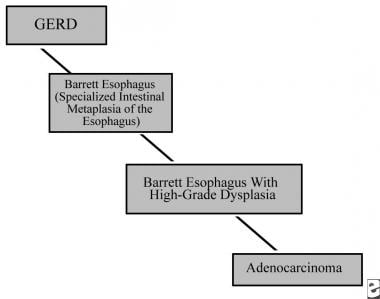
Gastroesophageal Reflux Disease. Gastroesophageal reflux disease (GERD)/Barrett esophagus/adenocarcinoma sequence.

Gastroesophageal Reflux Disease. Endoscopy demonstrating intraluminal esophageal cancer.
As with esophageal stricture, the presence of Barrett esophagus indicates the need for surgical consultation and treatment (usually surgical fundoplication).
![]()
- Giannini EG, Zentilin P, Dulbecco P, Vigneri S, Scarlata P, Savarino V. Management strategy for patients with gastroesophageal reflux disease: a comparison between empirical treatment with esomeprazole and endoscopy-oriented treatment. Am J Gastroenterol. 2008 Feb. 103(2):267-75. [QxMD MEDLINE Link].
- Katz PO. Medical therapy for gastroesophageal reflux disease in 2007. Rev Gastroenterol Disord. 2007 Fall. 7(4):193-203. [QxMD MEDLINE Link].
- Fass R, Sifrim D. Management of heartburn not responding to proton pump inhibitors. Gut. 2009 Feb. 58(2):295-309. [QxMD MEDLINE Link].
- Fass R. Proton pump inhibitor failure--what are the therapeutic options?. Am J Gastroenterol. 2009 Mar. 104 suppl 2:S33-8. [QxMD MEDLINE Link].
- Heidelbaugh JJ, Goldberg KL, Inadomi JM. Overutilization of proton pump inhibitors: a review of cost-effectiveness and risk [corrected]. Am J Gastroenterol. 2009 Mar. 104 suppl 2:S27-32. [QxMD MEDLINE Link].
- Dial MS. Proton pump inhibitor use and enteric infections. Am J Gastroenterol. 2009 Mar. 104 suppl 2:S10-6. [QxMD MEDLINE Link].
- DeVault KR, Castell DO. Updated guidelines for the diagnosis and treatment of gastroesophageal reflux disease. Am J Gastroenterol. 2005 Jan. 100(1):190-200. [QxMD MEDLINE Link].
- Gallup Organization. Heartburn Across America: A Gallup Organization National Survey. Princeton, NJ: Gallup Organization; 1988.
- Richter JE. Surgery for reflux disease: reflections of a gastroenterologist. N Engl J Med. 1992 Mar 19. 326(12):825-7. [QxMD MEDLINE Link].
- Chen CL, Robert JJ, Orr WC. Sleep symptoms and gastroesophageal reflux. J Clin Gastroenterol. 2008 Jan. 42(1):13-7. [QxMD MEDLINE Link].
- Sveen S. Symptom check: is it GERD?. J Contin Educ Nurs. 2009 Mar. 40(3):103-4. [QxMD MEDLINE Link].
- Mittal RK, Rochester DF, McCallum RW. Sphincteric action of the diaphragm during a relaxed lower esophageal sphincter in humans. Am J Physiol. 1989 Jan. 256(1 Pt 1):G139-44. [QxMD MEDLINE Link].
- Mittal RK, McCallum RW. Characteristics of transient lower esophageal sphincter relaxation in humans. Am J Physiol. 1987 May. 252(5 Pt 1):G636-41. [QxMD MEDLINE Link].
- Mittal RK, Rochester DF, McCallum RW. Effect of the diaphragmatic contraction on lower oesophageal sphincter pressure in man. Gut. 1987 Dec. 28(12):1564-8. [QxMD MEDLINE Link]. [Full Text].
- Stein HJ, DeMeester TR. Outpatient physiologic testing and surgical management of foregut motility disorders. Curr Probl Surg. 1992 Jul. 29(7):413-555. [QxMD MEDLINE Link].
- Kahrilas PJ, Dodds WJ, Hogan WJ, Kern M, Arndorfer RC, Reece A. Esophageal peristaltic dysfunction in peptic esophagitis. Gastroenterology. 1986 Oct. 91(4):897-904. [QxMD MEDLINE Link].
- Buttar NS, Falk GW. Pathogenesis of gastroesophageal reflux and Barrett esophagus. Mayo Clin Proc. 2001 Feb. 76(2):226-34. [QxMD MEDLINE Link].
- Hampel H, Abraham NS, El-Serag HB. Meta-analysis: obesity and the risk for gastroesophageal reflux disease and its complications. Ann Intern Med. 2005 Aug 2. 143(3):199-211. [QxMD MEDLINE Link]. [Full Text].
- Herbella FA, Sweet MP, Tedesco P, Nipomnick I, Patti MG. Gastroesophageal reflux disease and obesity. Pathophysiology and implications for treatment. J Gastrointest Surg. 2007 Mar. 11(3):286-90. [QxMD MEDLINE Link].
- Merrouche M, Sabate JM, Jouet P, et al. Gastro-esophageal reflux and esophageal motility disorders in morbidly obese patients before and after bariatric surgery. Obes Surg. 2007 Jul. 17(7):894-900. [QxMD MEDLINE Link].
- Murray L, Johnston B, Lane A, et al. Relationship between body mass and gastro-oesophageal reflux symptoms: The Bristol Helicobacter Project. Int J Epidemiol. 2003 Aug. 32(4):645-50. [QxMD MEDLINE Link]. [Full Text].
- Pandolfino JE, El-Serag HB, Zhang Q, Shah N, Ghosh SK, Kahrilas PJ. Obesity: a challenge to esophagogastric junction integrity. Gastroenterology. 2006 Mar. 130(3):639-49. [QxMD MEDLINE Link].
- El-Serag HB, Graham DY, Satia JA, Rabeneck L. Obesity is an independent risk factor for GERD symptoms and erosive esophagitis. Am J Gastroenterol. 2005 Jun. 100(6):1243-50. [QxMD MEDLINE Link].
- Tutuian R,. Adverse effects of drugs on the esophagus. Best Pract Res Clin Gastroenterol. 2010 Apr. 24(2):91-7. [QxMD MEDLINE Link].
- Kim SH. Esophageal mucosal impedance assessment: clinical usefulness for diagnosis of gastroesophageal reflux disease. J Neurogastroenterol Motil. 2024 Jul 30. 30 (3):253-4. [QxMD MEDLINE Link]. [Full Text].
- Galmiche JP, Hatlebakk J, Attwood S, et al. Laparoscopic antireflux surgery vs esomeprazole treatment for chronic GERD: the LOTUS randomized clinical trial. JAMA. 2011 May 18. 305(19):1969-77. [QxMD MEDLINE Link].
- Bhatia J, Parish A. GERD or not GERD: the fussy infant. J Perinatol. 2009 May. 29 suppl 2:S7-11. [QxMD MEDLINE Link].
- Levine MS, Rubesin SE. Diseases of the esophagus: diagnosis with esophagography. Radiology. 2005 Nov. 237(2):414-27. [QxMD MEDLINE Link].
- Lages RB, Fontes LHS, Barbuti RC, Navarro-Rodriguez T. Esophageal mucosal impedance assessment for the diagnosis of gastroesophageal reflux disease. J Neurogastroenterol Motil. 2024 Jul 30. 30 (3):352-60. [QxMD MEDLINE Link]. [Full Text].
- Ponce J, Garrigues V, Agreus L, et al. Structured management strategy based on the Gastro-oesophageal Reflux Disease (GERD) Questionnaire (GerdQ) vs. usual primary care for GERD: pooled analysis of five cluster-randomised European studies. Int J Clin Pract. 2012 Sep. 66(9):897-905. [QxMD MEDLINE Link].
- Woodcock J. Statement alerting patients and health care professionals of NDMA found in samples of ranitidine [news release]. September 13, 2019. US Food and Drug Administration. Available at https://www.fda.gov/news-events/press-announcements/statement-alerting-patients-and-health-care-professionals-ndma-found-samples-ranitidine. 2019 Jun; Accessed: October 15, 2020.
- US Food and Drug Administration. FDA requests removal of all ranitidine products (Zantac) from the market [news release]. April 1, 2020. Available at https://www.fda.gov/news-events/press-announcements/fda-requests-removal-all-ranitidine-products-zantac-market. Accessed: October 15, 2020.
- Yang YX, Lewis JD, Epstein S, Metz DC. Long-term proton pump inhibitor therapy and risk of hip fracture. JAMA. 2006 Dec 27. 296(24):2947-53. [QxMD MEDLINE Link]. [Full Text].
- Kellerman R, Kintanar T. Gastroesophageal reflux disease. Prim Care. 2017 Dec. 44(4):561-73. [QxMD MEDLINE Link].
- US Food and Drug Administration Press Announcements. FDA approves first generic versions of Aciphex delayed-release tablets to treat GERD. US Food and Drug Administration. Available at https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm374329.htm. Accessed: November 12, 2013.
- Agency for Healthcare Research and Quality. Comparative effectiveness of management strategies for gastroesophageal reflux disease - executive summary. AHRQ pub. no. 06-EHC003-1. December 2005. Available at https://effectivehealthcare.ahrq.gov/healthInfo.cfm?infotype=rr&ProcessID=1&DocID=42. Accessed: September 27, 2010.
- Rassameehiran S, Klomjit S, Hosiriluck N, Nugent K. Meta-analysis of the effect of proton pump inhibitors on obstructive sleep apnea symptoms and indices in patients with gastroesophageal reflux disease. Proc (Bayl Univ Med Cent). 2016 Jan. 29(1):3-6. [QxMD MEDLINE Link].
- Phathom Pharmaceuticals. Phathom Pharmaceuticals announces FDA approval of VOQUEZNA (vonoprazan) tablets for the treatment of erosive GERD and relief of heartburn associated with erosive GERD in adults [news release]. Available at https://investors.phathompharma.com/news-releases/news-release-details/phathom-pharmaceuticals-announces-fda-approval-voqueznar. November 1, 2023; Accessed: November 9, 2023.
- Phathom Pharmaceuticals announces positive topline results from PHALCON-EE pivotal phase 3 erosive esophagitis trial. Phathom Pharmaceuticals. Available at https://investors.phathompharma.com/news-releases/news-release-details/phathom-pharmaceuticals-announces-positive-topline-results-0. October 18, 2021; Accessed: November 9, 2023.
- Laine L, DeVault K, Katz P, Mitev S, Lowe J, Hunt B, et al. Vonoprazan versus lansoprazole for healing and maintenance of healing of erosive esophagitis: a randomized trial. Gastroenterology. 2023 Jan. 164 (1):61-71. [QxMD MEDLINE Link]. [Full Text].
- Phathom Pharmaceuticals. Phathom Pharmaceuticals announces FDA approval of VOQUEZNA (vonoprazan) tablets for the relief of heartburn associated with non-erosive GERD in adults [news release]. Available at https://investors.phathompharma.com/news-releases/news-release-details/phathom-pharmaceuticals-announces-fda-approval-voqueznar-0. July 18, 2024; Accessed: July 19, 2024.
- Laine L, Spechler S, Yadlapati R, et al. Vonoprazan is efficacious for treatment of heartburn in non-erosive reflux disease: a randomized trial. Clin Gastroenterol Hepatol. 2024 May 14. [QxMD MEDLINE Link]. [Full Text].
- Brooks M. FDA OKs Voquezna for heartburn relief in nonerosive gastroesophageal reflux disease. Medscape Medical News. Available at https://www.medscape.com/viewarticle/fda-oks-voquezna-heartburn-relief-nonerosive-2024a1000dal. July 18, 2024; Accessed: July 19, 2024.
- Boerema I. Hiatus hernia: repair by right-sided, subhepatic, anterior gastropexy. Surgery. 1969 Jun. 65(6):884-93. [QxMD MEDLINE Link].
- Allison PR. Hiatus hernia: (a 20-year retrospective survey). Ann Surg. 1973 Sep. 178(3):273-6. [QxMD MEDLINE Link]. [Full Text].
- Varshney S, Kelly JJ, Branagan G, Somers SS, Kelly JM. Angelchik prosthesis revisited. World J Surg. 2002 Jan. 26(1):129-33. [QxMD MEDLINE Link].
- Nissen R, Rossetti M, Siewert R. [20 years in the management of reflux disease using fundoplication]. Chirurg. 1977 Oct. 48(10):634-9. [QxMD MEDLINE Link].
- Kazerooni NL, VanCamp J, Hirschl RB, Drongowski RA, Coran AG. Fundoplication in 160 children under 2 years of age. J Pediatr Surg. 1994 May. 29(5):677-81. [QxMD MEDLINE Link].
- Dallemagne B, Weerts JM, Jehaes C, Markiewicz S, Lombard R. Laparoscopic Nissen fundoplication: preliminary report. Surg Laparosc Endosc. 1991 Sep. 1(3):138-43. [QxMD MEDLINE Link].
- Nilsson G, Larsson S, Johnsson F. Randomized clinical trial of laparoscopic versus open fundoplication: blind evaluation of recovery and discharge period. Br J Surg. 2000 Jul. 87(7):873-8. [QxMD MEDLINE Link].
- Wenner J, Nilsson G, Oberg S, Melin T, Larsson S, Johnsson F. Short-term outcome after laparoscopic and open 360 degrees fundoplication. A prospective randomized trial. Surg Endosc. 2001 Oct. 15(10):1124-8. [QxMD MEDLINE Link].
- Somme S, Rodriguez JA, Kirsch DG, Liu DC. Laparoscopic versus open fundoplication in infants. Surg Endosc. 2002 Jan. 16(1):54-6. [QxMD MEDLINE Link].
- Rangel SJ, Henry MC, Brindle M, Moss RL. Small evidence for small incisions: pediatric laparoscopy and the need for more rigorous evaluation of novel surgical therapies. J Pediatr Surg. 2003 Oct. 38(10):1429-33. [QxMD MEDLINE Link].
- Rothenberg SS. The first decade's experience with laparoscopic Nissen fundoplication in infants and children. J Pediatr Surg. 2005 Jan. 40(1):142-6; discussion 147. [QxMD MEDLINE Link].
- Pascoe E, Falvey T, Jiwane A, Henry G, Krishnan U. Outcomes of fundoplication for paediatric gastroesophageal reflux disease. Pediatr Surg Int. 2016 Apr. 32(4):353-61. [QxMD MEDLINE Link].
- Lundell L, Miettinen P, Myrvold HE, et al. Continued (5-year) followup of a randomized clinical study comparing antireflux surgery and omeprazole in gastroesophageal reflux disease. J Am Coll Surg. 2001 Feb. 192(2):172-9; discussion 179-81. [QxMD MEDLINE Link].
- Spechler SJ. Epidemiology and natural history of gastro-oesophageal reflux disease. Digestion. 1992. 51 suppl 1:24-9. [QxMD MEDLINE Link].
- Anvari M, Allen C, Marshall J, et al. A randomized controlled trial of laparoscopic Nissen fundoplication versus proton pump inhibitors for treatment of patients with chronic gastroesophageal reflux disease: One-year follow-up. Surg Innov. 2006 Dec. 13(4):238-49. [QxMD MEDLINE Link].
- Grant AM, Wileman SM, Ramsay CR, et al. Minimal access surgery compared with medical management for chronic gastro-oesophageal reflux disease: UK collaborative randomised trial. BMJ. 2008 Dec 15. 337:a2664. [QxMD MEDLINE Link]. [Full Text].
- El-Serag HB. Time trends of gastroesophageal reflux disease: a systematic review. Clin Gastroenterol Hepatol. 2007 Jan. 5(1):17-26. [QxMD MEDLINE Link].
- Grant AM, Cotton SC, Boachie C, et al. Minimal access surgery compared with medical management for gastro-oesophageal reflux disease: five year follow-up of a randomised controlled trial (REFLUX). BMJ. 2013 Apr 18. 346:f1908. [QxMD MEDLINE Link]. [Full Text].
- Rebecchi F, Allaix ME, Giaccone C, Ugliono E, Scozzari G, Morino M. Gastroesophageal reflux disease and laparoscopic sleeve gastrectomy: a physiopathologic evaluation. Ann Surg. 2014 Nov. 260(5):909-14; discussion 914-5. [QxMD MEDLINE Link].
- Oor JE, Roks DJ, Unlu C, Hazebroek EJ. Laparoscopic sleeve gastrectomy and gastroesophageal reflux disease: a systematic review and meta-analysis. Am J Surg. 2016 Jan. 211(1):250-67. [QxMD MEDLINE Link].
- US Food and Drug Administration. FDA approves LINX Reflux Management System to treat gastroesophageal reflux disease. Available at https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm296923.htm.
- Zhang H, Dong D, Liu Z, He S, Hu L, Lv Y. Revaluation of the efficacy of magnetic sphincter augmentation for treating gastroesophageal reflux disease. Surg Endosc. 2016 Sep. 30(9):3684-90. [QxMD MEDLINE Link].
- Schizas D, Mastoraki A, Papoutsi E, et al. LINX® reflux management system to bridge the "treatment gap" in gastroesophageal reflux disease: a systematic review of 35 studies. World J Clin Cases. 2020 Jan 26. 8(2):294-305. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] Katz PO, Dunbar KB, Schnoll-Sussman FH, Greer KB, Yadlapati R, Spechler SJ. ACG Clinical Guideline for the Diagnosis anCG Clinical guideline for the diagnosis and management of gastroesophageal reflux diseased Management of Gastroesophageal Reflux Disease. Am J Gastroenterol. 2022 Jan 1. 117 (1):27-56. [QxMD MEDLINE Link]. [Full Text].
- Kramer JR, Shakhatreh MH, Naik AD, Duan Z, El-Serag HB. Use and yield of endoscopy in patients with uncomplicated gastroesophageal reflux disorder. JAMA Intern Med. 2014 Mar. 174(3):462-5. [QxMD MEDLINE Link].
- Mattioli S, Lugaresi ML, Di Simone MP, et al. The surgical treatment of the intrathoracic migration of the gastro-oesophageal junction and of short oesophagus in gastro-oesophageal reflux disease. Eur J Cardiothorac Surg. 2004 Jun. 25(6):1079-88. [QxMD MEDLINE Link].
- Osterwell N. GERD: high-risk patients get endoscopic short shrift. January 27, 2014. Medscape Medical News by WebMD. Available at https://www.medscape.com/viewarticle/819754. Accessed: February 3, 2014.
- Scheffer RC, Samsom M, Haverkamp A, Oors J, Hebbard GS, Gooszen HG. Impaired bolus transit across the esophagogastric junction in postfundoplication dysphagia. Am J Gastroenterol. 2005 Aug. 100(8):1677-84. [QxMD MEDLINE Link].
- Talley NJ, Napthali KE. Endoscopy in symptomatic gastroesophageal reflux disease: scoping out whom to target. JAMA Intern Med. 2014 Mar. 174(3):465-6. [QxMD MEDLINE Link].
- Telem DA, Altieri M, Gracia G, Pryor AD. Perioperative outcome of esophageal fundoplication for gastroesophageal reflux disease in obese and morbidly obese patients. Am J Surg. 2014 Aug. 208(2):163-8. [QxMD MEDLINE Link].
- Liu L, Li S, Zhu K, et al. Relationship between esophageal motility and severity of gastroesophageal reflux disease according to the Los Angeles classification. Medicine (Baltimore). 2019 May. 98(19):e15543. [QxMD MEDLINE Link].
- Ratcliffe EG, Jankowski JA. Gastroesophageal reflux disease and Barrett esophagus: an overview of evidence-based guidelines. Pol Arch Intern Med. 2019 Aug 29. 129(7-8):516-25. [QxMD MEDLINE Link]. [Full Text].
- Popescu AL, Ionita-Radu F, Jinga M, Gavrila AI, Savulescu FA, Fierbinteanu-Braticevici C. Laparoscopic sleeve gastrectomy and gastroesophageal reflux. Rom J Intern Med. 2018 Dec 1. 56(4):227-32. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] Hunt R, Armstrong D, Katelaris P, et al. World Gastroenterology Organisation Global Guidelines: GERD global perspective on gastroesophageal reflux disease. J Clin Gastroenterol. 2017 Jul. 51(6):467-78. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] Gyawali CP, Carlson DA, Chen JW, Patel A, Wong RJ, Yadlapati RH. ACG clinical guidelines: clinical use of esophageal physiologic testing. Am J Gastroenterol. 2020 Sep. 115(9):1412-28. [QxMD MEDLINE Link]. [Full Text].
Author
Marco G Patti, MD Surgeon, UNC Hospitals Multispecialty Surgery Clinic
Marco G Patti, MD is a member of the following medical societies: American Association for the Advancement of Science, American College of Surgeons, American Gastroenterological Association, American Medical Association, American Surgical Association, Association for Academic Surgery, Pan-Pacific Surgical Association, Society for Surgery of the Alimentary Tract, Society of American Gastrointestinal and Endoscopic Surgeons, Southwestern Surgical Congress, Western Surgical Association
Disclosure: Nothing to disclose.
Chief Editor
Acknowledgements
Piero Marco Fisichella, MD Assistant Professor of Surgery, Stritch School of Medicine, Loyola University; Director, Esophageal Motility Center, Loyola University Medical Center.
Piero Marco Fisichella is a member of the following medical societies: American College of Surgeons, American Medical Association, Association for Academic Surgery, Society for Surgery of the Alimentary Tract, and Society of American Gastrointestinal and Endoscopic Surgeons
Disclosure: Nothing to disclose.
Fernando AM Herbella, MD, PhD, TCBC Affiliate Professor, Attending Surgeon in Gastrointestinal Surgery, Esophagus and Stomach Division, Department of Surgery, Federal University of Sao Paulo, Brazil; Private Practice; Medical Examiner, Sao Paulo's Medical Examiner's Office Headquarters, Brazil
Fernando AM Herbella, MD, PhD, TCBC is a member of the following medical societies: Society for Surgery of the Alimentary Tract
Disclosure: Nothing to disclose.
John Gunn Lee, MD Director of Pancreaticobiliary Service, Associate Professor, Department of Internal Medicine, Division of Gastroenterology, University of California at Irvine School of Medicine
John Gunn Lee, MD is a member of the following medical societies: American College of Gastroenterology, American College of Physicians, American Gastroenterological Association, and American Society for Gastrointestinal Endoscopy
Disclosure: Nothing to disclose.
Thomas F Murphy, MD Chief of Abdominal Imaging Section, Department of Radiology, Tripler Army Medical Center
Disclosure: Nothing to disclose.
Francisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical Center College of Pharmacy; Editor-in-Chief, Medscape Drug Reference
Disclosure: Medscape Salary Employment
Manish K Varma, MD Chief of Interventional Radiology, Department of Radiology, Tripler Army Medical Center
Manish K Varma, MD is a member of the following medical societies: American College of Radiology, American Roentgen Ray Society, and Radiological Society of North America
Disclosure: Nothing to disclose.
Noel Williams, MD Professor Emeritus, Department of Medicine, Dalhousie University, Halifax, Nova Scotia, Canada; Professor, Department of Internal Medicine, Division of Gastroenterology, University of Alberta, Edmonton, Alberta, Canada
Noel Williams, MD is a member of the following medical societies: Royal College of Physicians and Surgeons of Canada
Disclosure: Nothing to disclose.