Garlic intake and the risk of colorectal cancer: A meta-analysis (original) (raw)
Abstract
This was a meta-analysis of epidemiological articles that aimed to estimate the association of garlic intake with the risk of colorectal cancer (CRC).
Electronic databases, including the Cochrane Database of Systematic Reviews, PubMed, and EMBASE, were systemically searched from inception to May 2019 to identify related articles. In addition, a random model was used to pool the included evidence based on heterogeneity. Additionally, subgroup analyses were carried out to examine the differences between different groups. The stability of our findings was tested through sensitivity analyses. Publication bias was also assessed by Egger and Begg tests. Moreover, all enrolled studies were ordered according to the publication year for a cumulative meta-analysis.
A total of 11 studies (involving 12,558 cases) were included in the current meta-analysis. Our integrated relative risk (RR) of CRC was 0.80 (95% confidence interval [CI], 0.69–0.91) for the highest versus the lowest garlic consumption categories (RR: 0.71 [95% CI, 0.60–0.84] for controls and RR: 0.99 [95% CI, 0.80–1.23] for cohorts). There was significant heterogeneity across all enrolled studies (_I_2 = 68.3%, P < .01). The sensitivity analysis revealed no notable alterations of the integrated results. According to the funnel plot regarding garlic intake and the risk of CRC, together with the Egger test (P = .1) and Begg test (P = .064) results, there was no notable evidence of publication bias. The cumulative meta-analysis suggested that the 95% CIs became narrower with the increase in sample size.
Based on the existing evidence, garlic intake could reduce the risk of CRC.
Keywords: colorectal cancer, diet, epidemiology, garlic, meta-analysis
1. Introduction
Colorectal cancer (CRC) has the third highest rate of morbidity worldwide, behind lung cancer and breast cancer. Altogether, 1,849,518 patients are diagnosed with CRC every year, accounting for 10.2% of all cancer cases, and CRC ranked second and third in prevalence among females and males, respectively, in 2018.[1] In addition, CRC is the second leading cause of cancer-related death worldwide, regardless of certain geographical differences with regard to its morbidity and mortality. Typically, Asia has the greatest morbidity (n = 957,896; 51.8%) and mortality (n = 461,422; 52.4%), irrespective of age and sex. Many scientific articles have suggested that the consumption of vegetables may impact the incidence of cancer; in particular, certain geographical and environmental factors, including diet, may play a vital role in CRC development.[2–4]
Garlic has been used globally in numerous ways. According to the World Cancer Research Fund/American Institute for Cancer Research, garlic consumption has a potentially favorable effect against CRC.[5] Some evidence has suggested that garlic consumption can lower CRC risk.[6–8] Related data from the past 10 years have updated the knowledge in this regard, and some epidemiological studies have examined the relationship of garlic intake with CRC risk; nonetheless, no definite conclusion can be made. Two meta-analyses published in 2014[9,10] quantitatively estimated the association and suggested that garlic showed no evident effect in terms of CRC risk reduction. In contrast, Federica Turati's article[6] based on 9 articles published in the same year showed a pooled RR of CRC of 0.85 (95% confidence interval [CI], 0.72–1.00), and it was concluded that garlic intake might protect against CRC. In addition, a hospital-based case-control study carried out in Shanghai found that garlic consumption was linked to a reduced risk of CRC.[11] Additionally, the American Cancer Society Cancer Prevention Study II cohort indicated that CRC risk was weakly inversely associated with dietary garlic intake among females, but such a risk was possibly increased among males.[12] Additionally, an Italian and Swiss case-control study found that garlic intake could protect against CRC.[13] To further explore the relationship between garlic intake and CRC risk, the current meta-analysis was carried out.
2. Materials and methods
2.1. Retrieval strategy and screening criteria
Articles examining the relationship of garlic intake with CRC were systemically retrieved from the Cochrane Database of Systematic Reviews, PubMed and EMBASE databases from inception through May 2019 by 2 researchers (Xi Zhou and Dan Zhang) independently. The following string was used for the retrieval: “(((garlic) OR allium sativum) OR vegetable) AND (((((cancer) OR neoplastic disease) OR neoplasm) OR tumor) OR carcinoma) AND (((rectal) OR colon) OR colorectal).” Moreover, these 2 researchers were also responsible for retrieving and assessing the candidate studies that examined the relationship of garlic intake (excluding supplementary intake of garlic) with the risk of CRC based on human observational research published in the English language. Additionally, the reference lists of the selected studies were also screened to avoid omitting any eligible study. If we required more information, the original authors were contacted.
The study inclusion criteria were as follows:
- (1)
cohort or case-control studies; - (2)
studies evaluating the relationship of garlic consumption with CRC risk; - (3)
studies reporting the relative risk (RR) or odds ratio (OR) and 95% CI or the essential data for calculation.
For repeated studies carried out among identical research populations, the most informative study was included. Two studies were excluded because they examined garlic supplementation rather than dietary garlic intake.[14,15] In addition, studies examining pepper and onion consumption together with garlic intake or the overall intake of allium vegetables were excluded.[16,17] In addition, 2 studies were carried out with an identical study population, and the most informative one was included.[18,19]
2.2. Data collection and quality evaluation
Three researchers (Xi Zhou, Dan Zhang, Haihua Qian) were responsible for collecting and verifying the data. Any disagreement among them was settled by mutual negotiation. Data were collected from all included studies, including the last name of the first author, year of publication, study design, study region/country, sex, subject number (including cases and controls/noncases/cohort size), and estimated RR (for >1 estimated RR in 1 study, the 1 adjusting for the most confounding factors was included in the analysis) with the 95% CI (the greatest versus smallest garlic consumption categories; garlic supplement users were excluded). When necessary, the data of cases and noncases/persons that were at risk were adjusted for every exposure category and covariate before subsequent analysis.
Study quality was evaluated based on the 9-star Newcastle–Ottawa scale (NOS)[10] independently by 2 researchers (Xi Zhou and Dan Zhang). Each study was assigned 9 stars at most, and studies assigned ≥7 stars were of high quality.[20]
2.3. Statistical analyses
In this study, RRs were utilized as a risk estimate. There is a low absolute CRC risk among humans; as a result, ORs were directly deemed as RRs.[20,21] The fixed-effects model was utilized when studies reported the colon and rectal cancer risks separately to integrate all risk estimates while obtaining the overall CRC estimate.[21–23] The _I_2 statistic and Cochrane Q test were adopted to assess the potential heterogeneity among the included studies,[24,25] and _I_2 > 50% or P < .05 indicated heterogeneous results.[26] Moreover, the fixed-effects model was employed in the absence of distinct heterogeneity; otherwise, the random-effects model was adopted. Sensitivity analysis was also carried out by removing each individual study 1 at a time in sequence to assess the effect of each study on integrated risk estimates. Subgroup analyses were also carried out as stratified based on the cancer position, sex, geographic area, sample size, and study design. Begg and Egger[27] linear regression was employed to evaluate publication bias. Differences with P < .05 were regarded as statistically significant. STATA (version 12; StataCorp, College Station, TX) was utilized for all statistical analyses.
2.4. Ethical statement
This is a meta-analysis, which was based on previous published studies and did not have original data. Therefore, no ethical approval and patient consent are required.
3. Results
3.1. Literature retrieval
Altogether, 5081 candidate studies were identified during the initial retrieval, among which 5049 were eliminated after abstract or title screening. For the remaining 32 studies, the full texts were carefully read. One candidate studies were identified after viewing the reference lists of the included studies. After full-text assessment, 11 articles were retrieved and included in our meta-analysis. Figure 1 presents the study retrieval process.
Figure 1.
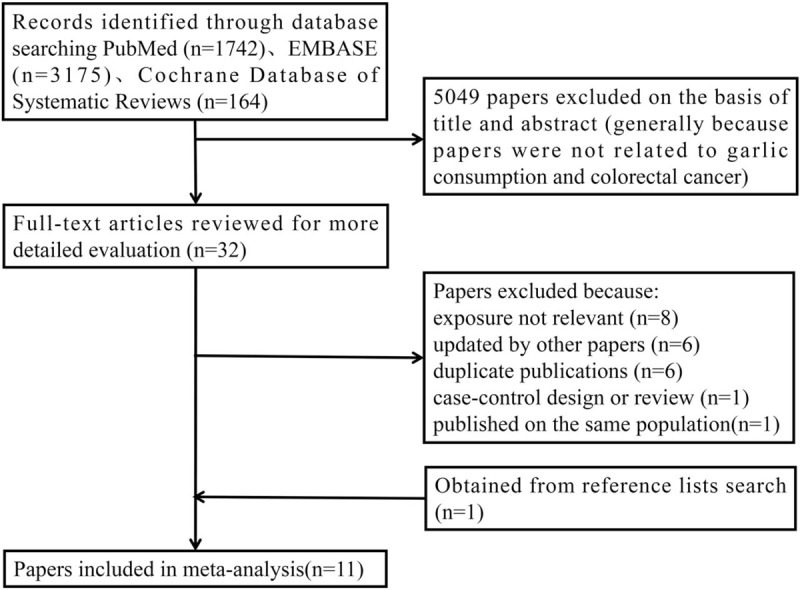
Process of study selection for the meta-analysis.
3.2. Study characteristics
A total of 11 articles published from 1991 to 2018 involving 12 datasets (n = 12,558) were included in the current meta-analysis.[11–13,19,28–34] Among these studies, the article from Meng et al[28] recruited 2 cohorts, namely, the Health Professionals Follow-up Study (HPFS) and the Nurses’ Health Study (NHS). Table 1 displays the major features of the 11 articles. We defined studies with a sample size ≤10,000 as having a small sample size; otherwise, they had a large sample size. Eight of the 11 studies had small sample sizes,[11,13,29–34] while the remaining 3 had large sample sizes[12,19,28] (n = 35,216–99,700). Furthermore, these studies were conducted in many regions, among which 6 datasets were from America, 2 datasets were from Asia, 3 datasets were from Europe, and 1 dataset was from Australia. The number of CRC cases among these articles ranged from 109 to 2280. Table 1 shows the study quality score on the basis of the 9-star NOS system. Two studies had 7 stars,[19,29] 6[13,28,30,31,34] had 8 stars, and 4[11,12,32,33] had 9 stars. Based on the quality evaluation criteria, each of the studies enrolled in the current meta-analysis were of high quality. Also, we conducted Grading of Recommendations Assessment Development and Evaluation (GRADE) evaluation of the evidence in Table 2.
Table 1.
Main characters of included studies.
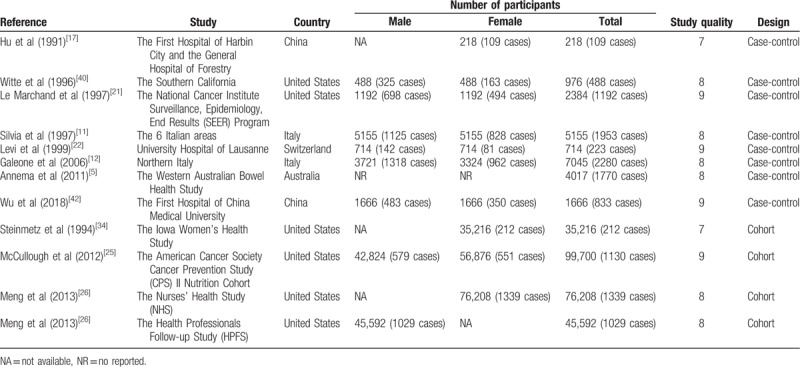
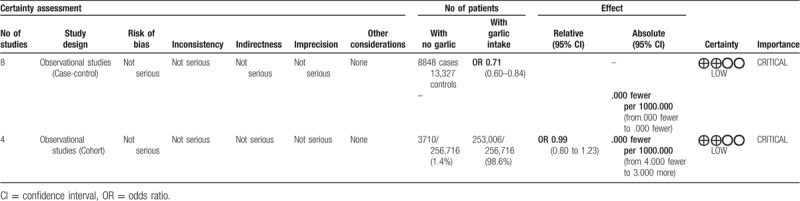
Table 2.
GRADE evidence profile of garlic intake for the risk of colorectal cancer.
3.3. Overall and subgroup analysis
Eleven studies mentioned risk estimates regarding garlic consumption and CRC risk. The random-effects model was used in the meta-analysis, which revealed an increased CRC risk (RR: 0.80; 95% CI: 0.69–0.91). Garlic consumption was related to a lower risk of CRC (Fig. 2).
Figure 2.
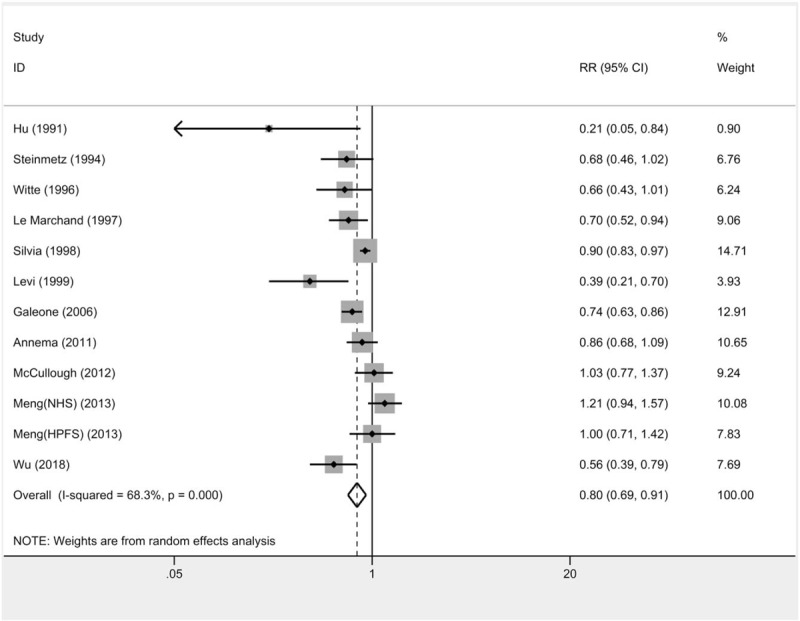
Forest plots for the associations between garlic intake and colorectal cancer risk.
As shown in Table 3, subgroup analyses were carried out to examine the underlying factors associated with CRC risk between the highest versus lowest garlic consumption groups. As observed, garlic consumption had a stronger association with rectal cancer than with colon cancer. European studies suggested a stronger inverse relationship of garlic than that identified in Asian and American studies, which was especially notable in the only 1 Australian study. Additionally, the sample size of the studies might have affected our assessment of the relationship of garlic intake with CRC. The small sample size suggested that garlic intake reduced CRC risk. Based on the study design, there was relevant heterogeneity among articles, and no definite results were obtained from cohort studies (Fig. 3). In subgroup analyses stratified by sex, no statistical significance was detected in the male and female groups.
Table 3.
Summary relative risks of colorectal cancer and corresponding 95% confidence intervals for the highest versus the lowest category of garlic intake of selected factors.
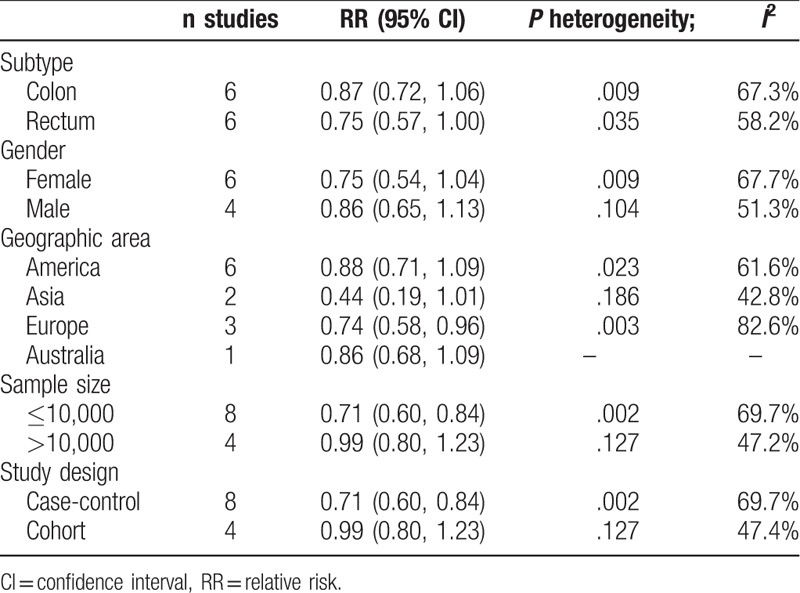
Figure 3.
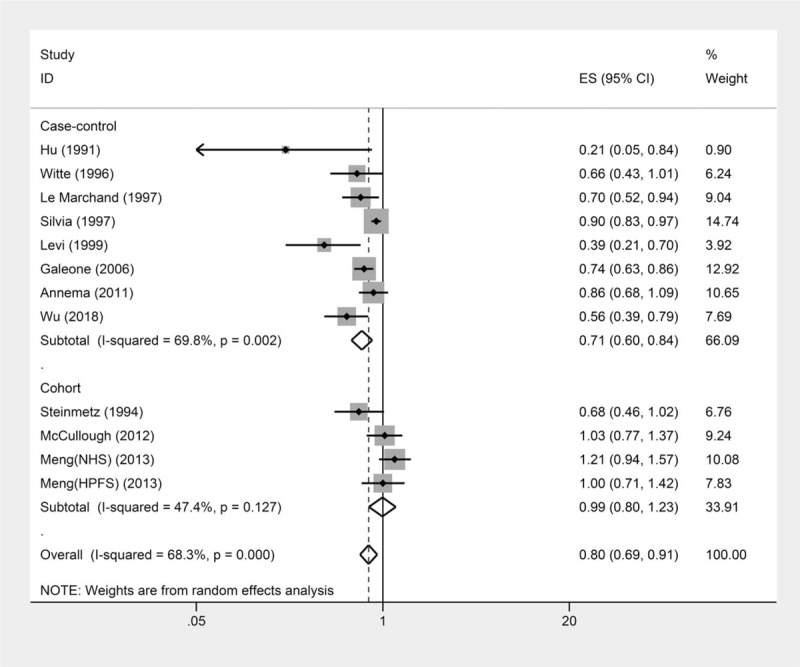
Subgroup analysis of study design for the associations between garlic intake and colorectal cancer risk.
3.4. Heterogeneity assessment
There was significant heterogeneity among the included articles (_I_2 = 68.3%, P < .01). As a result, the Galbraith plot test was conducted to explore the possible heterogeneity source based on the included articles. Nonetheless, our results suggested that 3 articles[11,28,33] might have been the leading sources of heterogeneity. No significant change was detected when these 3 studies were excluded (RR: 0.80; 95% CI: 0.71–0.91).
3.5. Cumulative meta-analysis
All enrolled articles were ordered according to their year of publication to conduct a cumulative meta-analysis. According to the cumulative meta-analysis results, the relationship of garlic consumption with CRC risk was in chronological order (Fig. 4). In addition, the corresponding 95% CIs became narrower as the sample size increased, suggesting increasing estimated accuracy with the continuous inclusion of studies.
Figure 4.
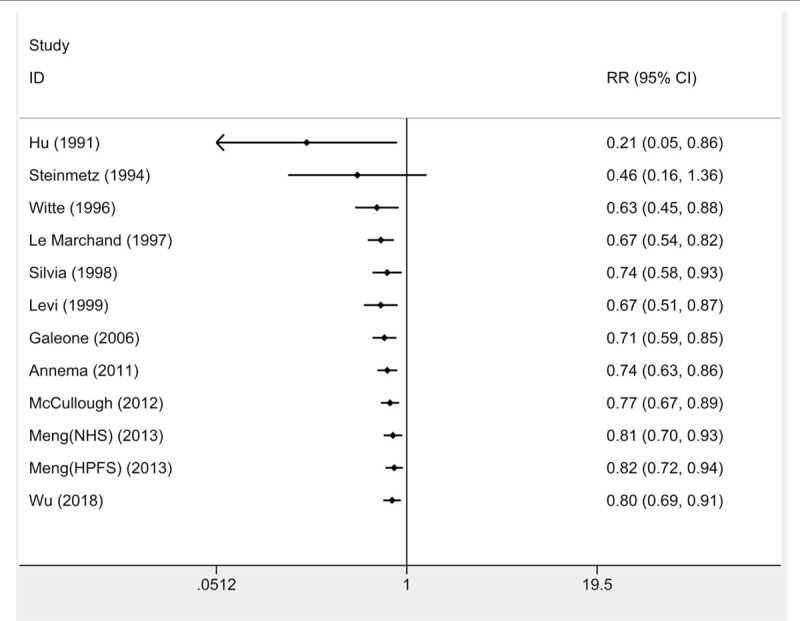
Cumulative meta-analysis of the relationship between the colorectal cancer risk and garlic intake.
3.6. Sensitivity analysis
The influence of 1 article on the overall estimates was assessed through sensitivity analysis, which was performed by eliminating 1 individual article at a time in sequence. According to the results of the sensitivity analysis, the RR varied from 0.76 ([95% CI: 0.67–0.88], when the study from Meng et al[28] was excluded [NHS]) to 0.82 ([95% CI: 0.72–0.93] when the study from Levi et al[33] was eliminated) (Fig. 5). There was no notable difference among the pooled findings.
Figure 5.
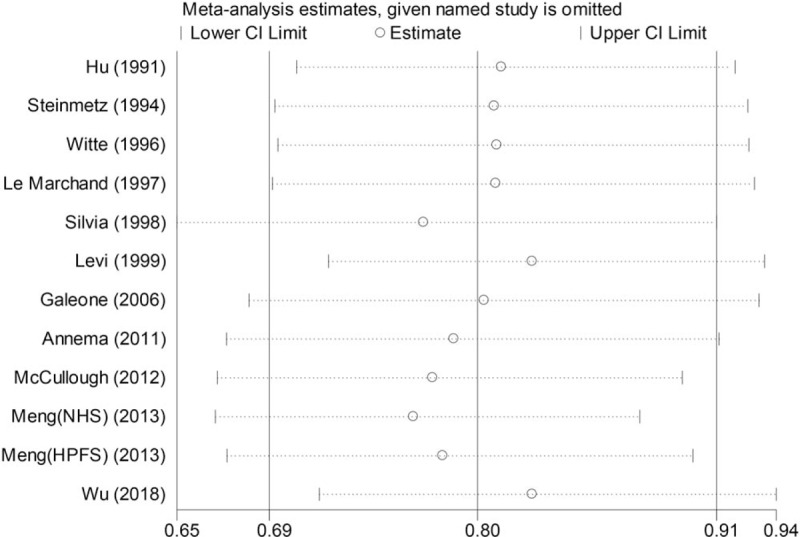
Sensitivity analysis to evaluate the effect of each study on the overall estimate by sequentially excluding 1 study in 1 turn.
3.7. Publication bias
The potential publication bias among the enrolled articles was assessed by Egger and Begg tests (Fig. 6). There was no notable evidence of publication bias (P = .1 and P = .064, respectively).
Figure 6.
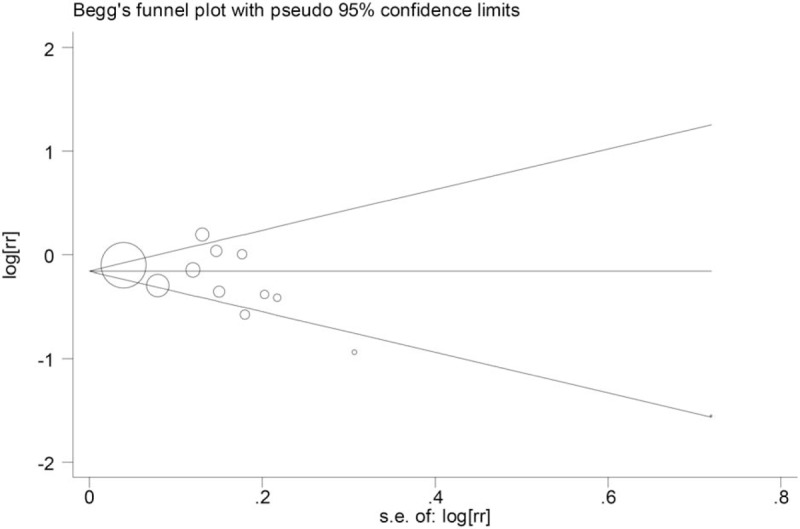
Funnel plot indicating publication bias in the studies included in the meta-analysis of the garlic intake and the colorectal cancer.
4. Discussion
The current meta-analysis integrated the findings from 11 epidemiological studies, which included 8 case-control and 4 cohort studies (Meng [NHS] and Meng [HPFS] were regarded as 2 cohort studies). Our results suggested that garlic consumption was associated with protection against CRC (RR = 0.80, 95% CI: 0.69–0.91).
The extent of heterogeneity among all included articles was assessed through a quantified _I_2 test and Q test, and significant heterogeneity was detected (_I_2 = 68.3%, P < .01). A Galbraith plot test was carried out, which revealed that 3 studies might be the main sources of heterogeneity, but no notable change was found when excluding these studies (RR = 0.80, 95% CI: 0.71–0.91). However, there was heterogeneity among the included articles, especially based on various regions and study design. The results of the case-control (RR = 0.71, 95% CI: 0.60–0.84) and cohort (RR = 0.99, 95% CI: 0.80–1.23) studies are shown. The following reasons may explain these results. First, this meta-analysis included observational studies, which might be influenced by different sources of bias, especially in regard to the retrospective studies. For a retrospective study, recall bias may partially lead to case-control results that are different from cohort results, which is ascribed to the influence of recent CRC diagnosis on recalling dietary habits. In addition, for case-control studies, health-conscious cases may have overreported the consumption of “health food” (such as vegetables), which may thereby hinder the potential determination of an actual relationship. Second, all cohort studies were carried out in America, a place distinct from Europe. In Europe, local people generally eat olive oil, tomatoes, and garlic in sauces of pasta and salads.[35] The per capita garlic consumption in the US has increased greatly over the past few decades.[6] In conclusion, this meta-analysis suggested that greater garlic intake led to a reduced CRC risk.
The cancer-prevention mechanism of garlic remains unclear. S-allylmercaptocysteine, the water-soluble derivative of garlic, has been found to display anti-proliferative capacity in numerous cancer cell lines, and it has also shown tumor-inhibiting effects in in vivo conditions.[36,37] Garlic can enhance the anticancer ability by activating the antioxidant transcription expression of Nrf2 and the downstream gene NQ01.[38] Aged black garlic (ABG) can modify the mRNA expression of neuropeptides and proteins in the case of inflammation.[39] Alternatively, ABG can exert its anticancer function by suppressing the proliferation of cells.[40] Garlic is potentially potent against some types of cancers; importantly, it is a universal anticancer drug that is potent against different cancers[41]; this effect is achieved by suppressing the growth of cancer cells and effectively suppressing the proliferation of infiltrative macrophages within the tumor-like microenvironment.[41] A large amount of preclinical data suggests that garlic has a certain effect on modulating the metabolism of carcinogens, inhibiting the progression of the cell cycle, inducing apoptosis and histone modification, and inhibiting angiogenesis.[42] Studies in vivo and in vitro suggest that garlic, together with garlic compounds, can protect against carcinogenesis by forming the carcinogen-DNA adduct, through angiogenesis and cell proliferation, by promoting apoptosis and anti-tumorigenic genes and redistributing the cell cycle.[3,43]
Some limitations should be noted in the current meta-analysis. First, all data were derived from observational studies, which resulted in residual or unmeasured confounding factors, even though the identified factors were adjusted in many included articles. Second, the unit and definition of garlic intake in every category were not standardized across all included studies. Third, certain subgroup analyses had a small dataset. Fourth, with regard to the features of case-control and cohort studies, the latter is a superior approach for illustrating the relationship of garlic consumption with CRC risk. In addition, the results obtained based on cohort studies are reliable and valuable because they are controlled for confounders. Finally, only the English articles were included in the current meta-analysis, which might lead to possible publication bias, even though Egger test revealed no evident publication bias.
Nonetheless, this meta-analysis had certain strengths. Specifically, the reporting recommendations from the MOOSE group were followed,[44] the retrieval string was used, and concept terms including “vegetable” and “allium sativum” were used, rather than depending on specific terms associated with garlic. This made it possible to identify studies that provided data regarding garlic from abstracts or titles, as well as those providing data from tables or the main text.
5. Conclusions
In summary, garlic intake can lower CRC risk. Nonetheless, such a conclusion was mainly drawn based on case-control studies, while no definite result was obtained from cohort studies. Thus, our results should be interpreted with caution. More epidemiological results, especially large-scale prospective cohort studies, can contribute to elucidating and quantifying the underlying protective effect of garlic against CRC.
Author contributions
Data curation: Xi Zhou, Haihua Qian, Dan Zhang.
Methodology: Xi Zhou, Li Zeng.
Software: Xi Zhou, Dan Zhang.
Supervision: Haihua Qian, Dan Zhang.
Writing – original draft: Xi Zhou.
Writing – review and editing: Li Zeng.
Footnotes
Abbreviations: CI = confidence interval, CRC = colorectal cancer, NA = not available, NR = not reported, RR = relative risk.
How to cite this article: Zhou X, Qian H, Zhang D, Zeng L. Garlic intake and the risk of colorectal cancer: A meta-analysis. Medicine. 2020;99:1(e18575).
The authors have no conflicts of interest to disclose.
References
- [1].Onyoh EF, Hsu W, Chang L, et al. The rise of colorectal cancer in Asia: epidemiology, screening, and management. Current Gastroenterol Rep 2019;21:36. [DOI] [PubMed] [Google Scholar]
- [2].Wang W, Dong Z, Zhang X, et al. Dietary and the risk of sporadic colorectal cancer in China: a case-control study. Iran J Public Health 2018;47:1327–35. [PMC free article] [PubMed] [Google Scholar]
- [3].Ngo SN, Williams DB, Cobiac L, et al. Does garlic reduce risk of colorectal cancer? A systematic review. J Nutr 2007;137:2264–9. [DOI] [PubMed] [Google Scholar]
- [4].Guercio V, Galeone C, Turati F, et al. Gastric cancer and allium vegetable intake: a critical review of the experimental and epidemiologic evidence. Nutr Cancer 2014;66:757–73. [DOI] [PubMed] [Google Scholar]
- [5].Wiseman M. Food, Nutrition, Physical Activity and the Prevention of Cancer: A Global Perspective: A Project of World Cancer Research Fund International. Washington, D.C: American Institute for Cancer Research; 2007. [Google Scholar]
- [6].Turati F, Guercio V, Pelucchi C, et al. Colorectal cancer and adenomatous polyps in relation to allium vegetables intake: a meta-analysis of observational studies. Mol Nutr Food Res 2014;58:1907–14. [DOI] [PubMed] [Google Scholar]
- [7].Dorant E, Van den Brandt PA, Goldbohm RA. A prospective cohort study on the relationship between onion and leek consumption, garlic supplement use and the risk of colorectal carcinoma in The Netherlands Carcinogenesis 1996;17:477–84. [DOI] [PubMed] [Google Scholar]
- [8].Ernst E, Posadzki P. Can garlic-intake reduce the risk of cancer? A systematic review of randomised controlled trials. Focus Altern Complement Ther 2012;17:192–6. [Google Scholar]
- [9].Zhu B, Zou L, Qi L, et al. Allium vegetables and garlic supplements do not reduce risk of colorectal cancer, based on meta-analysis of prospective studies. Clin Gastroenterol H 2014;12:1991–2001. [DOI] [PubMed] [Google Scholar]
- [10].Hu J. Consumption of garlic and risk of colorectal cancer: an updated meta-analysis of prospective studies. World J Gastroenterol 2014;20:15413–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Wu X, Shi J, Fang W, et al. Allium vegetables are associated with reduced risk of colorectal cancer: a hospital-based matched case-control study in China. Asia-Pac J Clin Oncol 2019;15:e132–41. [DOI] [PubMed] [Google Scholar]
- [12].McCullough ML, Jacobs EJ, Shah R, et al. Garlic consumption and colorectal cancer risk in the CPS-II nutrition cohort. Cancer Cause Control 2012;23:1643–51. [DOI] [PubMed] [Google Scholar]
- [13].Galeone C, Pelucchi C, Levi F, et al. Onion and garlic use and human cancer. Am J Clin Nutr 2006;84:1027–32. [DOI] [PubMed] [Google Scholar]
- [14].Dorant E, van den Brandt PA, Goldbohm RA. A prospective cohort study on the relationship between onion and leek consumption, garlic supplement use and the risk of colorectal carcinoma in The Netherlands. Carcinogenesis 1996;17:477–84. [DOI] [PubMed] [Google Scholar]
- [15].Satia JA, Littman A, Slatore CG, et al. Associations of herbal and specialty supplements with lung and colorectal cancer risk in the vitamins and lifestyle study. Cancer Epidemiol Biomarkers Prev 2009;18:1419–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Vogtmann E, Xiang Y, Li H, et al. Fruit and vegetable intake and the risk of colorectal cancer: results from the Shanghai Men's Health Study. Cancer Cause Control 2013;24:1935–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Iscovich JM, L’Abbe KA, Castelleto R, et al. Colon cancer in Argentina. I: risk from intake of dietary items. Int J Cancer 1992;51:851–7. [DOI] [PubMed] [Google Scholar]
- [18].Sellers TA, Bazyk AE, Bostick RM, et al. Diet and risk of colon cancer in a large prospective study of older women: an analysis stratified on family history (Iowa, United States). Cancer Causes Control 1998;9:357–67. [DOI] [PubMed] [Google Scholar]
- [19].Steinmetz KA, Kushi LH, Bostick RM, et al. Vegetables, fruit, and colon cancer in the Iowa Women's Health Study. Am J Epidemiol 1994;139:1–5. [DOI] [PubMed] [Google Scholar]
- [20].Zheng JS, Hu XJ, Zhao YM, et al. Intake of fish and marine n-3 polyunsaturated fatty acids and risk of breast cancer: meta-analysis of data from 21 independent prospective cohort studies. BMJ 2013;346:f3706. [DOI] [PubMed] [Google Scholar]
- [21].Wu QJ, Yang Y, Vogtmann E, et al. Cruciferous vegetables intake and the risk of colorectal cancer: a meta-analysis of observational studies. Ann Oncol 2013;24:1079–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Aune D, Chan DS, Lau R, et al. Dietary fibre, whole grains, and risk of colorectal cancer: systematic review and dose-response meta-analysis of prospective studies. BMJ 2011;343:d6617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Aune D, Lau R, Chan DS, et al. Nonlinear reduction in risk for colorectal cancer by fruit and vegetable intake based on meta-analysis of prospective studies. Gastroenterology 2011;141:106–18. [DOI] [PubMed] [Google Scholar]
- [24].Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med 2002;21:1539–58. [DOI] [PubMed] [Google Scholar]
- [25].Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses. BMJ 2003;327:557–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Jin M, Cai S, Guo J, et al. Alcohol drinking and all cancer mortality: a meta-analysis. Ann Oncol 2013;24:807–16. [DOI] [PubMed] [Google Scholar]
- [27].Papageorgiou SN, Papadopoulos MA, Athanasiou AE. Assessing small study effects and publication bias in orthodontic meta-analyses: a meta-epidemiological study. Clin Oral Investig 2014;18:1031–44. [DOI] [PubMed] [Google Scholar]
- [28].Meng S, Zhang X, Giovannucci EL, et al. No association between garlic intake and risk of colorectal cancer. Cancer Epidemiol 2013;37:152–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Hu JF, Liu YY, Yu YK, et al. Diet and cancer of the colon and rectum: a case-control study in China. Int J Epidemiol 1991;20:362–7. [DOI] [PubMed] [Google Scholar]
- [30].Franceschi S, Parpinel M, La Vecchia C, et al. Role of different types of vegetables and fruit in the prevention of cancer of the colon, rectum, and breast. Epidemiology 1998;9:338–41. [PubMed] [Google Scholar]
- [31].Annema N, Heyworth JS, McNaughton SA, et al. Fruit and vegetable consumption and the risk of proximal colon, distal colon, and rectal cancers in a case-control study in Western Australia. J Am Diet Assoc 2011;111:1479–90. [DOI] [PubMed] [Google Scholar]
- [32].Le Marchand L, Hankin JH, Wilkens LR, et al. Dietary fiber and colorectal cancer risk. Epidemiology 1997;8:658–65. [DOI] [PubMed] [Google Scholar]
- [33].Levi F, Pasche C, La Vecchia C, et al. Food groups and colorectal cancer risk. Br J Cancer 1999;79:1283–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Witte JS, Longnecker MP, Bird CL, et al. Relation of vegetable, fruit, and grain consumption to colorectal adenomatous polyps. Am J Epidemiol 1996;144:1015–25. [DOI] [PubMed] [Google Scholar]
- [35].Pelucchi C, Bosetti C, Rossi M, et al. Selected aspects of Mediterranean diet and cancer risk. Nutr Cancer 2009;61:756–66. [DOI] [PubMed] [Google Scholar]
- [36].Thomson M, Ali M. Garlic [Allium sativum]: a review of its potential use as an anti-cancer agent. Curr Cancer Drug Targets 2003;3:67–81. [DOI] [PubMed] [Google Scholar]
- [37].Liang D, Qin Y, Zhao W, et al. S-allylmercaptocysteine effectively inhibits the proliferation of colorectal cancer cells under in vitro and in vivo conditions. Cancer Lett 2011;310:69–76. [DOI] [PubMed] [Google Scholar]
- [38].Li S, Yang G, Zhu X, et al. Combination of rapamycin and garlic-derived S-allylmercaptocysteine induces colon cancer cell apoptosis and suppresses tumor growth in xenograft nude mice through autophagy/p62/Nrf2 pathway. Oncol Rep 2017;38:1637–44. [DOI] [PubMed] [Google Scholar]
- [39].Amor S, Gonzalez-Hedstrom D, Martin-Carro B, et al. Beneficial effects of an aged black garlic extract in the metabolic and vascular alterations induced by a high fat/sucrose diet in male rats. Nutrients 2019;11:E153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [40].Jikihara H, Qi G, Nozoe K, et al. Aged garlic extract inhibits 1,2-dimethylhydrazine-induced colon tumor development by suppressing cell proliferation. Oncol Rep 2015;33:1131–40. [DOI] [PubMed] [Google Scholar]
- [41].Bagul M, Kakumanu S, Wilson TA. Crude garlic extract inhibits cell proliferation and induces cell cycle arrest and apoptosis of cancer cells in vitro. J Med Food 2015;18:731–7. [DOI] [PubMed] [Google Scholar]
- [42].Powolny AA, Singh SV. Multitargeted prevention and therapy of cancer by diallyl trisulfide and related Allium vegetable-derived organosulfur compounds. Cancer Lett 2008;269:305–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [43].Altonsy MO, Andrews SC. Diallyl disulphide, a beneficial component of garlic oil, causes a redistribution of cell-cycle growth phases, induces apoptosis, and enhances butyrate-induced apoptosis in colorectal adenocarcinoma cells (HT-29). Nutr Cancer 2011;63:1104–13. [DOI] [PubMed] [Google Scholar]
- [44].Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of observational studies in epidemiology (MOOSE) group. JAMA 2000;283:2008–12. [DOI] [PubMed] [Google Scholar]