Disruption of a Large Intergenic Noncoding RNA in Subjects with Neurodevelopmental Disabilities (original) (raw)
Abstract
Large intergenic noncoding (linc) RNAs represent a newly described class of ribonucleic acid whose importance in human disease remains undefined. We identified a severely developmentally delayed 16-year-old female with karyotype 46,XX,t(2;11)(p25.1;p15.1)dn in the absence of clinically significant copy number variants (CNVs). DNA capture followed by next-generation sequencing of the translocation breakpoints revealed disruption of a single noncoding gene on chromosome 2, LINC00299, whose RNA product is expressed in all tissues measured, but most abundantly in brain. Among a series of additional, unrelated subjects referred for clinical diagnostic testing who showed CNV affecting this locus, we identified four with exon-crossing deletions in association with neurodevelopmental abnormalities. No disruption of the LINC00299 coding sequence was seen in almost 14,000 control subjects. Together, these subjects with disruption of LINC00299 implicate this particular noncoding RNA in brain development and raise the possibility that, as a class, abnormalities of lincRNAs may play a significant role in human developmental disorders.
Main Text
Large intergenic noncoding RNAs (lincRNAs), thought to number more than 4,000 in the human genome, have recently been identified as a new class of RNA molecule postulated to play important roles in gene regulation.1,2 Those lincRNAs that have been characterized functionally exhibit diverse biological activities including involvement in X chromosome inactivation and regulation of gene expression in stem cells, cancer cells, and development.3–6 It has been estimated that more than 30% of lincRNAs associate with chromatin-modifying complexes, such as PRC2 and co-REST, and subsequently target these complexes to specific genomic regions.1 Evidence for lincRNA function comes from studies of HOTAIR, a lincRNA that is part of the Hox gene cluster, in breast cancer progression,7 and ANRIL, a lincRNA involved in regulation of CDKN2A and CDKN2B and associated with atherosclerosis.8 Still, despite their potentially broad functional impact in development, no lincRNAs have been implicated in human developmental abnormalities. Here, we identify a lincRNA specifically disrupted in independent subjects with developmental disabilities.
Arguably, the discovery of direct disruption of a single locus in the genome from a de novo balanced alteration is among the most powerful approaches in human genetics for isolating individual genomic loci directly associated with the phenotype. In this study, we describe a 16-year-old female (DGAP162) with developmental delay from the Developmental Genome Anatomy Project (DGAP)9 whose clinical karyotype revealed a de novo balanced translocation: 46,XX,t(2;11)(p25.1;p15.1)dn. Array comparative genomic hybridization via 1 million probes (Agilent G3 microarray, Agilent, Santa Clara, CA) revealed no genomic deletions or duplications clinically interpreted as pathogenic. To rule out the possibility that a known pathogenic mutation involved in neurodevelopment was contributing to the phenotype of DGAP162, we sequenced genes CDKL5, FOXG1, MECP2, SLC9A6, and TCF4 in the diagnostic clinical laboratory at Boston Children’s Hospital, revealing only common polymorphisms in this case. No novel or known pathogenic mutations were discovered.
At birth, DGAP162 was delivered normally, weighing 2.7 kg (<5th percentile), after a 37.5 week pregnancy notable for oligohydramnios and dilated fetal kidneys at 34 weeks. Her immediate postnatal period was remarkable for poor feeding but all scans were normal and she was discharged at 10 days. Her parents suspected some developmental issue at the age of 9 months because of her failure to sit on her own and she was referred for developmental delay at 12 months. At 22 months, DGAP162 was a friendly, happy, and very sociable girl with no dysmorphic features but who ate only soft food. Though Angelman syndrome was suspected, diagnostic tests were negative. Her workup also included serum amino acid levels, thyroid function, and blood count, all of which were normal. However, an MRI revealed slightly delayed myelination and partial agenesis of the corpus callosum. At 30 months, she was thriving with a weight of 11.4 kg (5th–10th percentile) and height of 84.6 cm (5th percentile), though her head circumference was noted at the 10th percentile and her developmental difficulties were worsening. A urine amino acid screen was unremarkable. By 3.5–4 years of age, she had only begun to walk and subsequently required a walker until age 7. She developed episodes of unresponsiveness/stiffness; an EEG was abnormal and she was started on, and continues to take, sodium valproate. She suffered from recurrent ear infections/conductive hearing loss, which necessitated adenoidectomy and insertion of grommets. At age 6.5 years, her weight and height were 20 kg (25th percentile) and 118 cm (50th percentile), respectively. She did not chew her food (instead she swallowed it whole) and often put hard objects in her mouth. Sensory issues were noted, along with prominent tip-toe walking, though there were no motor problems. At age 7, she was in a special school but showed no progress in learning, self-help skills, or development. She was sleeping 14 hr a day, and she showed reduced attention, though her hearing was normal. She also began to put her hands in her mouth and frequently engaged in self-stimulation. Her EEG remained abnormal in wake and sleep and was interpreted as resulting from a developmental abnormality in the frontotemporal area. By 12 years, she showed normal-set eyes, normal-set ears, no arched palate, and no abnormal hand creases. She had severe learning difficulties and many repetitive sensory behaviors, with a very brief attention span. She was very sociable and engaged well with family and caregivers. Her EEG was abnormal with continued changes in the bilateral frontotemporal region. At 16 years, DGAP162 is very thin with a high palate and is quite mobile despite an abnormal gait, but she requires complete care. She is double incontinent, cannot feed herself, and is nonverbal with only slight grunts and physical action for communication, with a laugh-like squeal when excited. She displays poor eye contact, seems “off in her own world,” and has particular routines and ritual behaviors, including hand-flapping, head-banging, stuffing her hands in her mouth, and masturbation. She has never been formally assessed for autism. DGAP162 has two younger, developmentally normal siblings. Partners HealthCare System institutional review boards approved subject recruitment procedures and DNA screening and informed consent was obtained from the family.
We performed a DNA capture and sequencing experiment to determine the translocation breakpoints of DGAP162 by using methods (CapBP) that we have described previously.3 In brief, standard insert paired-end genomic DNA libraries were prepared with NEBnext reagents (New England Biolabs, Ipswich, MA) and Illumina multiplex adapters (Illumina, San Diego, CA). Custom DNA capture arrays (Agilent, Santa Clara, CA) were designed based upon an approximate translocation region defined by FISH via mapped BAC clones. We targeted a 313,002 bp region on chromosome (chr) 11 and a 246,713 bp region on chr 2 over most unique and repeat-masked sequences (see Figure 4b in Talkowski et al.3). The captured DGAP162 DNA was sequenced within a pool of DNA from multiple subjects on a single lane of a flow cell (Illumina HiSeq2000). Reads were aligned and analyzed with BWA and samtools.10,11 Chimeric read pairs were clustered with BamStat, which performs a single linkage clustering of anomalous pairs,3 identifying the putative translocation cluster. Pile-ups and coverage were compared to expectations with a custom-designed mappability tool to verify the likelihood of good coverage after DNA capture3 and split reads from translocation junction breakpoints were identified to base-pair resolution (Figure 1), then confirmed by Sanger sequencing.
Figure 1.
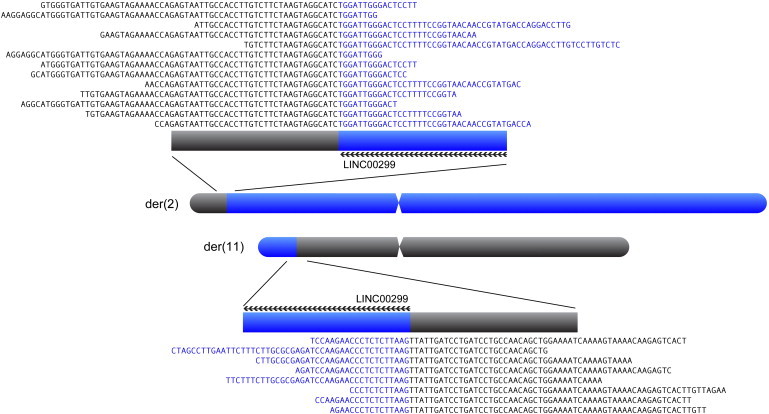
Identification of Translocation Breakpoints from DGAP162 by CapBP Methodology
A distal, short arm translocation involving chromosome 2 (blue) and chromosome 11 (gray) are shown, with split read sequences from fragments containing the breakpoint junctions provided. The next-gen cytogenetic karyotype is designated: 46,XX,der(2)(11pter–15,825,269::chr2 8,247,757–2qter),der(11)(2pter–8,247,756::chr11 15,825,273–11qter)dn (hg19). Additional details of sequence characteristics available in Chiang et al.12
Sequencing revealed a perfectly balanced translocation breakpoint on chr 2 and a loss of just three bases on chr 11 (hg19, Figure 1; der(2): 11pter–15,825,269::chr2 8,247,757–2qter, der(11): 2pter–8,247,756::chr11 15,825,273–11qter). There were no annotated genes, predicted genes, mRNAs, or expressed sequence tags within 500 kb on either side of the chr 11 breakpoint. However, on chr 2, the rearrangement breakpoint occurred within a large intron of LINC00299, directly disrupting this 316.9 kb gene that corresponds to cDNA clones BC043563 and AK127578; the former spans most of LINC00299 and the latter provides its 5′ portion and suggests alternative splicing. LINC00299 (previously known as FLJ45673, C2orf46, and NCRNA00299), assigned the name “long intergenic nonprotein coding RNA 299” by the HUGO Gene Nomenclature Committee, produces a member of the recently identified class of lincRNAs, based upon its large size, lack of coding potential, and location outside of known genes. Indeed, we screened, in silico, all of the annotated exons for ATG sites preceded by a GCC(A/G)CC Kozak sequence and found no evidence for such a translational start site. Similarly, to confirm whether any DNA in the region spanned by LINC00299 could give rise to an RNA with coding potential related to any known or suspected protein-coding RNA, we searched the entire genomic sequence with pfam, BlastX, and phyloCSF,13 all with negative results. Thus, although RNA is both transcribed and processed from this locus, it appears that no known or potential RNA transcript encodes any protein that can be detected by homology to known or predicted proteins. Finally, to confirm expression and predicted splicing of this gene, we performed an RNA fluorescence in situ hybridization (FISH) experiment by using lymphocytes from a karyotypically normal human subject. FISH probes were made from cDNA and the probe targeted an ∼500 bp region covering exons 5–7 (Figures 2 and 3A), suggesting that this gene is expressed and spliced in human lymphocytes.
Figure 2.
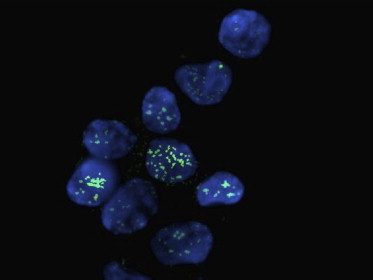
LINC00299 RNA Is Both Expressed and Spliced in Normal Human Lymphocytes
An RNA FISH probe targeting the spliced product of LINC00299 in EBV-transformed wild-type human lymphocytes. RNA FISH probe was ligated to an Alexa 488 dye, then hybridized to individual cells on a microscope slide. Individual cells are stained with the DNA dye 4′,6-diamidino-2-phenylindole (DAPI). Green dots in the blue nucleus suggest individual molecules of LINC00299 in each cell. Green stain, probe targeting exons 5–7 of LINC00299; blue stain, DAPI.
Figure 3.
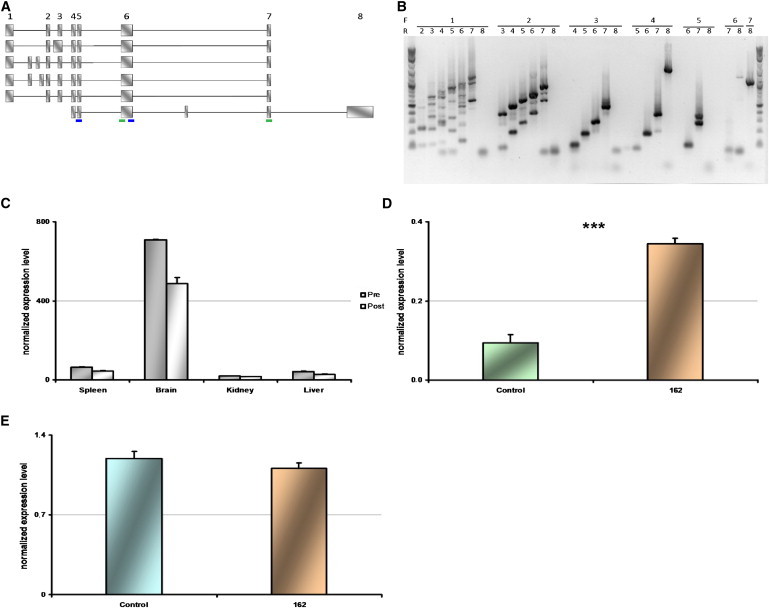
Structure of LINC00299 Transcripts in Brain, Expression Level across Human Tissues, and Expression of LINC00299 in Lymphoblastoid Cell Lines Comparing DGAP162 to Three Control Subjects
(A) LINC00299 alternative splice transcripts from RNA extracted from wild-type human prefrontal cortex (exons and introns not to scale). Numbers represent exons identified by RefSeq, and unreported exons are unnumbered. Each transcript represents a fully cloned RT-PCR fragment, confirmed by Sanger sequencing. Small bars below the final transcript refer to “pre” and “post” primer sets used for expression studies.
(B) Agarose electrophoresis gel showing amplification of LINC00299 transcripts in brain prefrontal cortex via different primers. Forward primers (F, top line) and reverse primers (R, bottom line) are noted by numbers representing which exon the specific primer targeted. Exon numbers correspond to exon numbers noted in (A).
(C) Expression level of LINC00299 transcripts in spleen, brain, kidney, and liver. “Pre” and “Post” refer to primers that bind 5′ and 3′, respectively, to the translocation breakpoint identified in DGAP162.
(D) Quantification of LINC00299 transcripts in lymphoblastoid cell lines from controls and DGAP162 with a probe targeting exon 6 of LINC00299 (pretranslocation), which amplified both the wild-type and mutant alleles of DGAP 162.
(E) Quantification of LINC00299 transcripts in lymphoblastoid cells via primers specific to the wild-type allele (posttranslocation probe).
∗∗∗p < 0.001. All reactions were run in quadruplicate and ACTB was used as an internal control in all cases. All primer sequences can be found in Table S1. All error bars represent standard error of the mean.
To determine the structure of LINC00299 RNA product(s), we designed primer pairs to amplify across each exon of cDNA BC043563, numbered as predicted by RefSeq (Figure 3A). Taqman RT-PCR reactions were performed in a total volume of 20 μl, on 384-well plates with an Applied Biosystems (Carlsbad, CA) 7900HT and a master mix commercialized by Quanta Biosciences. Serial dilutions provided amounts ranging from 0.04 ng to 10 ng of RNA. For each well, PCR mix included 10 μl of 2× Perfecta PCR 2 mix (Quanta Biosciences, Gaithersburg, MD), 1 μl of primers/probe mix, 2 μl of cDNA, H20 qsp 20 μl. A comparison of amplification product sizes and sequences to those predicted by BC043563 revealed several alternatively spliced transcripts (Figures 3A and 3B). Three exons were identified between BC043563 exons 1 and 2 (at sites, hg19, chr2: 8,452,858–8,452,972, 8,442,650–8,442,949, and 8,442,193–8,442,559) and one was found between exons 6 and 7 (chr2: 8,383,695–8,383,770). We were consistently able to amplify from exon 4 to 8, but never from upstream exons to exon 8, under a multitude of conditions, suggesting additional cryptic transcript complexity. All amplicons were cloned and Sanger sequenced. RNA sequencing data (not shown) suggests many more transcripts from this locus than identified here, highlighting the complexity of this lincRNA.
We next determined the expression pattern of LINC00299 in selected human tissues including spleen, brain, kidney, and liver as well as in DGAP162 lymphoblastoid cell lines and three control lymphoblastoid cell lines. In DGAP162, the translocation occurs in an intron immediately upstream of exon 7; thus this translocation results in a gene lacking the final two exons (exons 7 and 8, Figure 3A). One primer pair, referred to as “pre” (for “pretranslocation”) is located in exon 6 of LINC00299. The second primer pair, specific to only the wild-type allele in the mutant subject (DGAP162), amplifies from exon 5 to exon 7 (Figure 3A shows the binding sites of these primer pairs on the transcript). In cross-tissue comparisons, both primer sets revealed high expression of LINC00299 in brain compared to other regions (Figure 3C).
There was a significant increase of LINC00299 expression in the DGAP162 lymphoblastoid cell line (LCL) relative to controls via the pretranslocation primer set (p = 5.3 × 10−4; Figure 3D), though the overall expression levels were quite low in LCL (see Figure S1 available online for qRT-PCR Ct value graphs). With the wild-type-specific primer set (i.e., the primer set that can amplify only the nonmutant chromosome from DGAP162), the level of expression from the single normal allele of DGAP162 was equivalent to the level of expression from two wild-type alleles in controls (p > 0.05; Figure 3E). Quality control for RT-PCR experiments (no reverse transcriptase control experiments) can be found in Figure S1. These data suggest that an attempt at dosage compensation in DGAP162 cells in the presence of heterozygous inactivation results in upregulation of transcription of both normal and translocated alleles, producing increases in the normal amount of wild-type RNA from the former and producing a transcript from the latter that includes exon 6 but not exons 7 and 8. The latter represents a truncated transcript comprising only sequences from the chr 2 side of the breakpoint, or, alternatively, a fusion transcript that incorporates sequences from the chr 11 side of the breakpoint.
To understand whether LINC00299 might have a role in neurodevelopment, we used previously described human induced pluripotent stem (iPS) cell-derived neural progenitor cells that were developed from a healthy control subject.14 We differentiated these neural progenitor cells to functional, electrically active neurons over a 38 day period, sampling RNA at distinct time points and measuring LINC00299 expression. We are able to record stimulus-evoked action potentials from these cells 18 days postdifferentiation (initiated by the removal of FGF2 and EGF), suggesting that over a 38 day time period many neurodevelopmental changes are occurring (data not shown). We measured expression of pre- and posttranslocation exons from LINC00299 in these wild-type cells and found an increase in expression level over time (Figures 4A and 4B).
Figure 4.
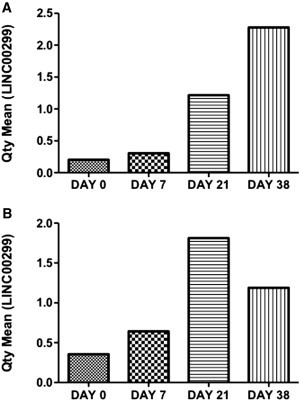
LINC00299 Temporal Expression in Induced Pluripotent Stem Cell-Derived Neural Progenitor Cells
mRNA expression levels were quantified using qRT-PCR and normalized using two endogenous controls, ACTB and GAPDH.
(A) Quantity mean values represent expression levels of LINC00299 in mRNA from exon 6.
(B) Quantity mean values represent expression levels of LINC00299 mRNA from exon 8.
All error bars represent standard error of the mean.
We tested whether disruption of LINC00299 also occurred in normal individuals, which would argue against it being a risk factor for abnormal neurodevelopment. We surveyed 13,991 adult controls from a series of genome-wide association studies, as we have previously described (see Talkowski et al.15). Among these controls, no individuals harbored a structural variant of any kind that disrupted any exonic region of this locus.
To corroborate the association of LINC00299 disruption with abnormal neurodevelopment, we also sought to identify other developmentally abnormal subjects where the locus was disrupted, and to compare their phenotypes where available. We analyzed diagnostic array data from Signature Genomics, LabCorp, DECIPHER, and ISCA (International Standards for Cytogenomic Arrays), selecting for subjects that had CNVs that overlapped LINC00299, a single CNV <10 Mb, and no other pathogenic CNVs in the genome. We identified four subjects with disruptions at LINC00299 (Table 1). Notably, all subjects with disruptions over LINC00299 had developmental delay. Together, subjects with nonrecurrent deletions in this region allow us to narrow a critical region to chr2: 7,554,804–8,945,097, which is less than 1.4 Mb. This region contains only ID2, MBOAT2, KIDINS220 5′ from LINC00299, and BC104747 3′ from LINC00299. Support for the specific involvement of LINC00299 in phenotypic expression comes from the translocation subject DGAP162 with a breakpoint directly in LINC00299 and subject L1 with a 60 kb deletion in the final two exons of LINC00299.
Table 1.
Subjects with Disruption Only at the LINC00299 Locus
| Sample | Chromosome Region | Event | Length | Phenotype |
|---|---|---|---|---|
| L1 | chr2: 8,058,207–8,117,927 | CN loss | 60 Kb | DD, seizures, bipolar |
| S1 | chr2: 5,148,670–8,945,097 | CN loss | 3.8 Mb | DD |
| S2 | chr2: 7,554,804–16,844,265 | CN loss | 9.3 Mb | DD |
| ISCA nssv577684 | chr2: 6,588,755–16,161,372 | CN loss | 9.6 Mb | global DD |
In one case (L1), we were able to recontact the physician for additional clinical information. This subject had an approximately 60 kb deletion that removed the final two exons of LINC00299 (chr2: 8,140,756–8,200,476), without altering neighboring genes. The individual is a 43-year-old female with a history of speech delay, mild-moderate intellectual disability, and bouts of confusion and abnormal behavior and is currently receiving treatment for bipolar disorder. She reportedly also has a seizure disorder with negative EEG assessment and has a disorder of articulation. She is said to be nondysmorphic, with weight 56.3 kg and height 164.5 cm. No brain imaging studies have been performed, and no cell line nor tissue were available for expression studies.
The two subjects (DGAP162 and L1) with their similarly defined genomic lesions altering only LINC00299 and the absence of such disruptions in normal individuals provide evidence for a role for this lincRNA gene in normal human development. Apart from the genetic lesions disrupting LINC00299, neither subject had a clinically interpreted dosage imbalance elsewhere in the genome, within the limits of the array analysis. The variability in the neurological and developmental phenotypes observed between the two subjects lacking the final two exons of this gene may reflect the actions of genetic, environmental, or stochastic modifiers. We acknowledge the differences in severity of phenotype between DGAP162 and L1. These issues, like delineation of the biological function of LINC00299, will require understanding its various isoforms and the timing and importance of their expression during development of the brain and other tissues. Because of the rarity of genomic lesions disrupting transcripts of LINC00299, this study does not have sufficient power to derive a statistically significant association between disruptions in this gene and pathology; these data show a suggestive clinical association and evidence for complex splicing patterns of LINC00299 and a potential role in neurodevelopment. Subjects with disruptions in LINC00299 have developmental disabilities of varying severity, though the most prominent effects appear to be in development and function of the brain. Both subjects for whom clinical data were available were also described as very thin, possibly suggesting some form of metabolic disorder. The model of dysregulation that we propose to explain the deficit is not haploinsufficiency, but rather either a gain-of-function or a dominant-negative action of a truncated form of LINC00299 where targets of the transcript are bound by a nonfunctional transcript. Extensive additional analyses are warranted to understand this mechanism and its potential specificity to lincRNA function. Overall, the implication of a lincRNA as an important component of proper neurodevelopment provides an entrée into the biology of such lincRNAs.
Acknowledgments
We thank the subjects and their families for participating in this study. This work was funded by NIH GM061354 (J.F.G. and C.C.M.), HD065286 (J.F.G.), K99MH095867 (M.E.T.), and R33MH087896 (S.J.H.). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. M.E.T. and J.F.G. are supported by the Simons Foundation for Autism Research and the Nancy Lurie Marks Family Foundation. C.E. is funded by a Canada Institute of Health Research Canada Research Chair in Psychiatric Genetics.
Supplemental Data
Document S1. Figure S1 and Table S1
Web Resources
The URLs for data presented herein are as follows:
- BamStat, http://talkowski.mgh.harvard.edu/
- BLAST and BLASTX, http://blast.ncbi.nlm.nih.gov/
- dbSNP, http://www.ncbi.nlm.nih.gov/projects/SNP/
- DECIPHER, https://decipher.sanger.ac.uk/
- DGAP database, http://www.bwhpathology.org/dgap/
- DGV, http://projects.tcag.ca/variation/
- ISCA, https://www.iscaconsortium.org/index.php/search
- Online Mendelian Inheritance in Man (OMIM), http://www.omim.org/
- Pfam, http://pfam.sanger.ac.uk/
References
- 1.Khalil A.M., Guttman M., Huarte M., Garber M., Raj A., Rivea Morales D., Thomas K., Presser A., Bernstein B.E., van Oudenaarden A. Many human large intergenic noncoding RNAs associate with chromatin-modifying complexes and affect gene expression. Proc. Natl. Acad. Sci. USA. 2009;106:11667–11672. doi: 10.1073/pnas.0904715106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Guttman M., Amit I., Garber M., French C., Lin M.F., Feldser D., Huarte M., Zuk O., Carey B.W., Cassady J.P. Chromatin signature reveals over a thousand highly conserved large non-coding RNAs in mammals. Nature. 2009;458:223–227. doi: 10.1038/nature07672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Talkowski M.E., Ernst C., Heilbut A., Chiang C., Hanscom C., Lindgren A., Kirby A., Liu S., Muddukrishna B., Ohsumi T.K. Next-generation sequencing strategies enable routine detection of balanced chromosome rearrangements for clinical diagnostics and genetic research. Am. J. Hum. Genet. 2011;88:469–481. doi: 10.1016/j.ajhg.2011.03.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wang K.C., Yang Y.W., Liu B., Sanyal A., Corces-Zimmerman R., Chen Y., Lajoie B.R., Protacio A., Flynn R.A., Gupta R.A. A long noncoding RNA maintains active chromatin to coordinate homeotic gene expression. Nature. 2011;472:120–124. doi: 10.1038/nature09819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Huarte M., Guttman M., Feldser D., Garber M., Koziol M.J., Kenzelmann-Broz D., Khalil A.M., Zuk O., Amit I., Rabani M. A large intergenic noncoding RNA induced by p53 mediates global gene repression in the p53 response. Cell. 2010;142:409–419. doi: 10.1016/j.cell.2010.06.040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Loewer S., Cabili M.N., Guttman M., Loh Y.H., Thomas K., Park I.H., Garber M., Curran M., Onder T., Agarwal S. Large intergenic non-coding RNA-RoR modulates reprogramming of human induced pluripotent stem cells. Nat. Genet. 2010;42:1113–1117. doi: 10.1038/ng.710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gupta R.A., Shah N., Wang K.C., Kim J., Horlings H.M., Wong D.J., Tsai M.C., Hung T., Argani P., Rinn J.L. Long non-coding RNA HOTAIR reprograms chromatin state to promote cancer metastasis. Nature. 2010;464:1071–1076. doi: 10.1038/nature08975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Burd C.E., Jeck W.R., Liu Y., Sanoff H.K., Wang Z., Sharpless N.E. Expression of linear and novel circular forms of an INK4/ARF-associated non-coding RNA correlates with atherosclerosis risk. PLoS Genet. 2010;6:e1001233. doi: 10.1371/journal.pgen.1001233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Higgins A.W., Alkuraya F.S., Bosco A.F., Brown K.K., Bruns G.A., Donovan D.J., Eisenman R., Fan Y., Farra C.G., Ferguson H.L. Characterization of apparently balanced chromosomal rearrangements from the developmental genome anatomy project. Am. J. Hum. Genet. 2008;82:712–722. doi: 10.1016/j.ajhg.2008.01.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Li H., Durbin R. Fast and accurate short read alignment with Burrows-Wheeler transform. Bioinformatics. 2009;25:1754–1760. doi: 10.1093/bioinformatics/btp324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Li H., Handsaker B., Wysoker A., Fennell T., Ruan J., Homer N., Marth G., Abecasis G., Durbin R., 1000 Genome Project Data Processing Subgroup The Sequence Alignment/Map format and SAMtools. Bioinformatics. 2009;25:2078–2079. doi: 10.1093/bioinformatics/btp352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Chiang C., Jacobsen J.C., Ernst C., Hanscom C., Heilbut A., Blumenthal I., Mills R.E., Kirby A., Lindgren A.M., Rudiger S.R. Complex reorganization and predominant non-homologous repair following chromosomal breakage in karyotypically balanced germline rearrangements and transgenic integration. Nat. Genet. 2012;44:390–397. doi: 10.1038/ng.2202. S1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Clamp M., Fry B., Kamal M., Xie X., Cuff J., Lin M.F., Kellis M., Lindblad-Toh K., Lander E.S. Distinguishing protein-coding and noncoding genes in the human genome. Proc. Natl. Acad. Sci. USA. 2007;104:19428–19433. doi: 10.1073/pnas.0709013104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sheridan S.D., Theriault K.M., Reis S.A., Zhou F., Madison J.M., Daheron L., Loring J.F., Haggarty S.J. Epigenetic characterization of the FMR1 gene and aberrant neurodevelopment in human induced pluripotent stem cell models of fragile X syndrome. PLoS ONE. 2011;6:e26203. doi: 10.1371/journal.pone.0026203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Talkowski M.E., Rosenfeld J.A., Blumenthal I., Pillalamarri V., Chiang C., Heilbut A., Ernst C., Hanscom C., Rossin E., Lindgren A.M. Sequencing chromosomal abnormalities reveals neurodevelopmental loci that confer risk across diagnostic boundaries. Cell. 2012;149:525–537. doi: 10.1016/j.cell.2012.03.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Document S1. Figure S1 and Table S1