Adjusting the Use of Glucose-Lowering Agents in the Real-World Clinical Management of People with Type 2 Diabetes: A Narrative Review (original) (raw)
FormalPara Key Summary Points
| Hyperglycaemia in diabetes causes microvascular and macrovascular complications, along with an increased risk of premature mortality. |
|---|
| Early attainment of individualized glycaemic control can have a legacy effect in patients with type 2 diabetes with long-term benefits. |
| Pragmatic implementation of international practice guidelines for management of type 2 diabetes is required due to variations in epidemiology, patient phenotypes, cultures, socioeconomic status, health systems, and access to medications. |
Introduction
Type 2 diabetes (T2D) is a complex, heterogeneous metabolic condition with an array of dysfunctions including insulin resistance and impaired insulin secretion [[1](/article/10.1007/s13300-023-01386-5#ref-CR1 "Lim LL, Chow E, Chan JCN. Cardiorenal diseases in type 2 diabetes mellitus: clinical trials and real-world practice. Nat Rev Endocrinol. 2023;19(3):151–63. https://doi.org/10.1038/s41574-022-00776-2
.")\]. One in 10 adults worldwide are living with diabetes, 90% of whom have T2D \[[2](/article/10.1007/s13300-023-01386-5#ref-CR2 "International Diabetes Federation. IDF Diabetes Atlas, 10th ed. 2021.
https://diabetesatlas.org/
. Accessed 20 Jan 2023.")\]. The Asia–Pacific accounts for more than 50% of the global population with diabetes, with more than 260 million people managing T2D on a daily basis \[[2](/article/10.1007/s13300-023-01386-5#ref-CR2 "International Diabetes Federation. IDF Diabetes Atlas, 10th ed. 2021.
https://diabetesatlas.org/
. Accessed 20 Jan 2023.")\]. The increasing prevalence of T2D mirrors the socioeconomic development, especially in low- and middle-income countries, with no sign of slowing down \[[2](/article/10.1007/s13300-023-01386-5#ref-CR2 "International Diabetes Federation. IDF Diabetes Atlas, 10th ed. 2021.
https://diabetesatlas.org/
. Accessed 20 Jan 2023."), [3](/article/10.1007/s13300-023-01386-5#ref-CR3 "Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H, Al Kaabi J. Epidemiology of type 2 diabetes—global burden of disease and forecasted trends. J Epidemiol Glob Health. 2020;10(1):107–11.
https://doi.org/10.2991/jegh.k.191028.001
.")\].Patients with T2D are at increased risk of developing microvascular and macrovascular complications, which are driven by hyperglycaemia and other cardiometabolic risk factors, notably hypertension, dyslipidaemia, and obesity [[4](/article/10.1007/s13300-023-01386-5#ref-CR4 "Stratton IM, Adler AI, Neil HA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321(7258):405–12. https://doi.org/10.1136/bmj.321.7258.405
.")\]. Despite the availability of new treatment classes, glycaemic control in patients with diabetes remained suboptimal globally \[[5](/article/10.1007/s13300-023-01386-5#ref-CR5 "Aschner P, Gagliardino JJ, Ilkova H, et al. Persistent poor glycaemic control in individuals with type 2 diabetes in developing countries: 12 years of real-world evidence of the International Diabetes Management Practices Study (IDMPS). Diabetologia. 2020;63(4):711–21.
https://doi.org/10.1007/s00125-019-05078-3
.")\]. This is associated with high risk of premature mortality related to diabetes and its complications \[[2](/article/10.1007/s13300-023-01386-5#ref-CR2 "International Diabetes Federation. IDF Diabetes Atlas, 10th ed. 2021.
https://diabetesatlas.org/
. Accessed 20 Jan 2023.")\]. In 2021, excluding deaths associated with the COVID-19 pandemic, an estimated 6.7 million people aged 20–79 years died as a result of diabetes. This corresponded to 12.2% of global deaths, with half of these deaths happening in the Asia–Pacific region \[[2](/article/10.1007/s13300-023-01386-5#ref-CR2 "International Diabetes Federation. IDF Diabetes Atlas, 10th ed. 2021.
https://diabetesatlas.org/
. Accessed 20 Jan 2023.")\]. In addition, one-third of these diabetes-related deaths occurred in people of working age (< 60 years), accounting for 11.8% of all deaths in people with diabetes \[[2](/article/10.1007/s13300-023-01386-5#ref-CR2 "International Diabetes Federation. IDF Diabetes Atlas, 10th ed. 2021.
https://diabetesatlas.org/
. Accessed 20 Jan 2023.")\].Cardiovascular disease (CVD) affected one-third of people with T2D [[6](/article/10.1007/s13300-023-01386-5#ref-CR6 "Einarson TR, Acs A, Ludwig C, Panton UH. Prevalence of cardiovascular disease in type 2 diabetes: a systematic literature review of scientific evidence from across the world in 2007–2017. Cardiovasc Diabetol. 2018;17(1):83. https://doi.org/10.1186/s12933-018-0728-6
.")\] and accounted for 50% of deaths in people with diabetes (with coronary artery disease \[CAD\] and stroke being the main contributors). In 2008, as a result of the complexity of diabetes and diverse mechanisms of actions of glucose-lowering drugs (GLDs), the US Food and Drug Administration (FDA) mandated the pharmaceutical industry to demonstrate cardiovascular safety for all new GLDs. Since then, none of the new classes of GLDs have been associated with increased risk of cardiovascular events \[[7](/article/10.1007/s13300-023-01386-5#ref-CR7 "Smith RJ, Goldfine AB, Hiatt WR. Evaluating the cardiovascular safety of new medications for type 2 diabetes: time to reassess? Diabetes Care. 2016;39(5):738–42.
https://doi.org/10.2337/dc15-2237
.")\]. More recent cardiovascular outcome trials (CVOTs) further confirmed the cardiorenal benefits of sodium–glucose cotransporter 2 (SGLT2) inhibitors and glucagon-like peptide 1 (GLP-1) receptor agonists in patients with T2D who had multiple risk factors and/or complications \[[1](/article/10.1007/s13300-023-01386-5#ref-CR1 "Lim LL, Chow E, Chan JCN. Cardiorenal diseases in type 2 diabetes mellitus: clinical trials and real-world practice. Nat Rev Endocrinol. 2023;19(3):151–63.
https://doi.org/10.1038/s41574-022-00776-2
."), [8](#ref-CR8 "Buse JB, Bain SC, Mann JFE, et al. Cardiovascular risk reduction with liraglutide: an exploratory mediation analysis of the LEADER trial. Diabetes Care. 2020;43(7):1546–52.
https://doi.org/10.2337/dc19-2251
."),[9](#ref-CR9 "Giugliano D, Scappaticcio L, Longo M, et al. GLP-1 receptor agonists and cardiorenal outcomes in type 2 diabetes: an updated meta-analysis of eight CVOTs. Cardiovasc Diabetol. 2021;20(1):189.
https://doi.org/10.1186/s12933-021-01366-8
."),[10](/article/10.1007/s13300-023-01386-5#ref-CR10 "Konig M, Riddle MC, Colhoun HM, et al. Exploring potential mediators of the cardiovascular benefit of dulaglutide in type 2 diabetes patients in REWIND. Cardiovasc Diabetol. 2021;20(1):194.
https://doi.org/10.1186/s12933-021-01386-4
.")\]. Although Asians were generally under-represented in these CVOTs \[[11](/article/10.1007/s13300-023-01386-5#ref-CR11 "Khunti K, Bellary S, Karamat MA, et al. Representation of people of South Asian origin in cardiovascular outcome trials of glucose-lowering therapies in type 2 diabetes. Diabet Med. 2017;34(1):64–8.
https://doi.org/10.1111/dme.13103
.")\], in a meta-analysis, Asian patients treated with SGLT2 inhibitors or GLP-1 receptor agonists were found to have lower hazard ratios (HR) of major events than their Caucasian counterparts \[[12](/article/10.1007/s13300-023-01386-5#ref-CR12 "Lee MMY, Ghouri N, McGuire DK, Rutter MK, Sattar N. Meta-analyses of results from randomized outcome trials comparing cardiovascular effects of SGLT2is and GLP-1RAs in Asian versus White patients with and without type 2 diabetes. Diabetes Care. 2021;44(5):1236–41.
https://doi.org/10.2337/dc20-3007
.")\].Despite these encouraging advancements, these CVOTs were conducted with the primary objective to evaluate the glucose-independent organ-protective effects [[7](/article/10.1007/s13300-023-01386-5#ref-CR7 "Smith RJ, Goldfine AB, Hiatt WR. Evaluating the cardiovascular safety of new medications for type 2 diabetes: time to reassess? Diabetes Care. 2016;39(5):738–42. https://doi.org/10.2337/dc15-2237
.")\] and did not address the causal relationships between diabetes complications and glycaemic control \[[4](/article/10.1007/s13300-023-01386-5#ref-CR4 "Stratton IM, Adler AI, Neil HA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321(7258):405–12.
https://doi.org/10.1136/bmj.321.7258.405
.")\]. The persistently poor glycaemic control despite the increasing number of GLDs calls for holistic and patient-centred management with dual attention to glucocentric and cardiorenal risk reduction. The objective of T2D management is to prevent complications and premature mortality and improve quality of life \[[13](/article/10.1007/s13300-023-01386-5#ref-CR13 "American Diabetes Association Professional Practice Committee. 6. Glycemic targets: Standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S83–S96.
https://doi.org/10.2337/dc22-S006
."), [14](/article/10.1007/s13300-023-01386-5#ref-CR14 "Davies MJ, Aroda VR, Collins BS, et al. Management of hyperglycemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022;45(11):2753–86.
https://doi.org/10.2337/dci22-0034
.")\]. Most international and regional practice guidelines recommend glycated haemoglobin (HbA1c) < 7.0% as a therapeutic goal in T2D \[[13](#ref-CR13 "American Diabetes Association Professional Practice Committee. 6. Glycemic targets: Standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S83–S96.
https://doi.org/10.2337/dc22-S006
."),[14](#ref-CR14 "Davies MJ, Aroda VR, Collins BS, et al. Management of hyperglycemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022;45(11):2753–86.
https://doi.org/10.2337/dci22-0034
."),[15](#ref-CR15 "International Diabetes Federation. IDF clinical practice recommendations for managing type 2 diabetes in primary care. 2017.
https://idf.org/e-library/guidelines/128-idf-clinical-practice-recommendations-for-managing-type-2-diabetes-in-primary-care.html
. Accessed 19 Jan 2023."),[16](#ref-CR16 "Jia W, Weng J, Zhu D, et al. Standards of medical care for type 2 diabetes in China 2019. Diabetes Metab Res Rev. 2019;35(6):e3158.
https://doi.org/10.1002/dmrr.3158
."),[17](/article/10.1007/s13300-023-01386-5#ref-CR17 "Araki E, Goto A, Kondo T, et al. Japanese clinical practice guideline for diabetes 2019. Diabetol Int. 2020;11(3):165–223.
https://doi.org/10.1007/s13340-020-00439-5
.")\]. However, hypoglycaemia and therapeutic inertia are major barriers in achieving optimal glycaemic control \[[18](/article/10.1007/s13300-023-01386-5#ref-CR18 "Khunti K, Davies M, Majeed A, Thorsted BL, Wolden ML, Paul SK. Hypoglycemia and risk of cardiovascular disease and all-cause mortality in insulin-treated people with type 1 and type 2 diabetes: a cohort study. Diabetes Care. 2015;38(2):316–22.
https://doi.org/10.2337/dc14-0920
.")\]. Apart from safety and efficacy, available resources and treatment affordability are additional considerations in selecting GLDs \[[19](/article/10.1007/s13300-023-01386-5#ref-CR19 "Mohan V, Khunti K, Chan SP, et al. Management of type 2 diabetes in developing countries: balancing optimal glycaemic control and outcomes with affordability and accessibility to treatment. Diabetes Ther. 2020;11(1):15–35.
https://doi.org/10.1007/s13300-019-00733-9
.")\]. Practice guidelines, largely based on experience in the USA and Europe, may not apply to regions such as Asia Pacific, where differences in epidemiology, patient phenotypes, cultures, and socioeconomic status need to be considered. Besides, to ensure accessibility, affordability, and sustainability of healthcare provision, a pragmatic approach is needed to optimize the use of all available drugs, including new and old, to reduce the burden of diabetes and its complications.This review is based on the content of a symposium entitled ‘Oral hypoglycaemic agents fact checking. Adjusting treatment options to real-world practice’ presented at the International Diabetes Federation’s Virtual Congress 2021 on 7 December 2021. In this article, we review the glucocentric and cardiorenal risk reduction approaches to the management of T2D supplemented by real-world evidence from the Asia Pacific region.
This article does not contain any new studies with human or animal subjects performed by any of the authors.
Importance of Glycaemic Control in Management of T2D
There are close relationships between glycaemic control and vascular complications in patients with T2D, including those of Asian descent [[4](/article/10.1007/s13300-023-01386-5#ref-CR4 "Stratton IM, Adler AI, Neil HA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321(7258):405–12. https://doi.org/10.1136/bmj.321.7258.405
."), [20](#ref-CR20 "UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352(9131):837–53."),[21](#ref-CR21 "Chen YY, Lin YJ, Chong E, et al. The impact of diabetes mellitus and corresponding HbA1c levels on the future risks of cardiovascular disease and mortality: a representative cohort study in Taiwan. PLoS ONE. 2015;10(4):e0123116.
https://doi.org/10.1371/journal.pone.0123116
."),[22](#ref-CR22 "Elley CR, Kenealy T, Robinson E, Drury PL. Glycated haemoglobin and cardiovascular outcomes in people with type 2 diabetes: a large prospective cohort study. Diabet Med. 2008;25(11):1295–301.
https://doi.org/10.1111/j.1464-5491.2008.02581.x
."),[23](#ref-CR23 "Perkovic V, Heerspink HL, Chalmers J, et al. Intensive glucose control improves kidney outcomes in patients with type 2 diabetes. Kidney Int. 2013;83(3):517–23.
https://doi.org/10.1038/ki.2012.401
."),[24](#ref-CR24 "Sakurai M, Saitoh S, Miura K, et al. HbA1c and the risks for all-cause and cardiovascular mortality in the general Japanese population: NIPPON DATA90. Diabetes Care. 2013;36(11):3759–65.
https://doi.org/10.2337/dc12-2412
."),[25](/article/10.1007/s13300-023-01386-5#ref-CR25 "Zoungas S, Chalmers J, Ninomiya T, et al. Association of HbA1c levels with vascular complications and death in patients with type 2 diabetes: evidence of glycaemic thresholds. Diabetologia. 2012;55(3):636–43.
https://doi.org/10.1007/s00125-011-2404-1
.")\]. In a prospective cohort of patients with T2D and no history of CVD, 51% of whom were non-Europeans, each 1% increase in HbA1c was associated with an increased risk for CVD (HR 1.08; 95% confidence interval \[CI\] 1.06, 1.10; _p_ < 0.001), after controlling for traditional risk factors \[[22](/article/10.1007/s13300-023-01386-5#ref-CR22 "Elley CR, Kenealy T, Robinson E, Drury PL. Glycated haemoglobin and cardiovascular outcomes in people with type 2 diabetes: a large prospective cohort study. Diabet Med. 2008;25(11):1295–301.
https://doi.org/10.1111/j.1464-5491.2008.02581.x
.")\].In the United Kingdom Prospective Diabetes Study (UKPDS), glycaemic control was associated with long-term reduction in all diabetes-related endpoints during the 10-year post-trial period [20]. In UKPDS, approximately 10% of patients were of Asian descent, and a sub-analysis of this study (UKPDS 32) demonstrated that the rate of myocardial infarction in patients from Asia (15.4 per 1000 patients) was similar to that in Europeans (14.6 per 1000 patients) [[26](/article/10.1007/s13300-023-01386-5#ref-CR26 "UK Prospective Diabetes Study Group. Ethnicity and cardiovascular disease. The incidence of myocardial infarction in white, South Asian, and Afro-Caribbean patients with type 2 diabetes (U.K. Prospective Diabetes Study 32). Diabetes Care. 1998;21(8):1271–7. https://doi.org/10.2337/diacare.21.8.1271
.")\]. In another sub-analysis of UKPDS (UKPDS 33), reducing HbA1c from 7.9% to 7.0% using sulfonylureas (SU) or insulin reduced the risk of microvascular complications (Table [1](/article/10.1007/s13300-023-01386-5#Tab1)) \[[20](/article/10.1007/s13300-023-01386-5#ref-CR20 "UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352(9131):837–53.")\]. In a post hoc epidemiological analysis of UKPDS (UKPDS 35), glycaemic exposure was linearly associated with increased risks of vascular complications and death \[[4](/article/10.1007/s13300-023-01386-5#ref-CR4 "Stratton IM, Adler AI, Neil HA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321(7258):405–12.
https://doi.org/10.1136/bmj.321.7258.405
.")\]. For every 1% decrement in HbA1c, there was a 14% risk reduction in myocardial infarction (_p_ < 0.0001) and a 37% risk reduction in microvascular complications (_p_ < 0.0001). For all clinical outcomes studied, there was no apparent threshold of glycaemia suggesting that a near-normal HbA1c target should be aimed at for reducing complications \[[4](/article/10.1007/s13300-023-01386-5#ref-CR4 "Stratton IM, Adler AI, Neil HA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321(7258):405–12.
https://doi.org/10.1136/bmj.321.7258.405
.")\].Table 1 United Kingdom Prospective Diabetes Study (UKPDS): risk reduction of key events during 10 years with intensive glycaemic control versus conventional treatment in newly diagnosed patients with type 2 diabetes [20]
The Action in Diabetes and Vascular Disease: Preterax and Diamicron MR Controlled Evaluation (ADVANCE) study assessed the effects of intensive glycaemic control on vascular outcomes in patients with T2D [[27](/article/10.1007/s13300-023-01386-5#ref-CR27 "ADVANCE Collaborative Group, Patel A, MacMahon S, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358(24):2560–72. https://doi.org/10.1056/NEJMoa0802987
.")\]. In this multicentre study, 11,140 patients (32% with CVD) received either standard glycaemic control or intensive glycaemic control, the latter using modified release gliclazide plus other GLDs, as required, in a 1:1 ratio. In ADVANCE, 37% of patients were enrolled from Asia, notably China. After 5 years, the intensive-control group achieved a mean HbA1c of 6.5% versus 7.3% in the standard-control group. This difference translated to a 10% relative risk reduction in the composite outcome of macrovascular and microvascular events, driven by a 21% relative risk reduction in kidney disease \[[27](/article/10.1007/s13300-023-01386-5#ref-CR27 "ADVANCE Collaborative Group, Patel A, MacMahon S, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358(24):2560–72.
https://doi.org/10.1056/NEJMoa0802987
.")\]. Further analysis indicated that intensive glycaemic control with modified-release gliclazide resulted in 65% risk reduction in end-stage kidney disease \[[23](/article/10.1007/s13300-023-01386-5#ref-CR23 "Perkovic V, Heerspink HL, Chalmers J, et al. Intensive glucose control improves kidney outcomes in patients with type 2 diabetes. Kidney Int. 2013;83(3):517–23.
https://doi.org/10.1038/ki.2012.401
.")\]. Post hoc analyses of the ADVANCE study suggested a non-linear relationship between mean HbA1c and risks of microvascular and macrovascular events and death with different threshold values \[[25](/article/10.1007/s13300-023-01386-5#ref-CR25 "Zoungas S, Chalmers J, Ninomiya T, et al. Association of HbA1c levels with vascular complications and death in patients with type 2 diabetes: evidence of glycaemic thresholds. Diabetologia. 2012;55(3):636–43.
https://doi.org/10.1007/s00125-011-2404-1
.")\]. While achieving HbA1c < 7.0% was not associated with further risk reduction for macrovascular events and death, the threshold value for microvascular events was 6.5%. For every 1% HbA1c level higher than these respective threshold values, there was a 38% higher risk for macrovascular events (vs a 7% threshold) and 40% higher risk for microvascular events and 38% higher risk for death (vs a 6.5% threshold; all _p_ < 0.0001) \[[25](/article/10.1007/s13300-023-01386-5#ref-CR25 "Zoungas S, Chalmers J, Ninomiya T, et al. Association of HbA1c levels with vascular complications and death in patients with type 2 diabetes: evidence of glycaemic thresholds. Diabetologia. 2012;55(3):636–43.
https://doi.org/10.1007/s00125-011-2404-1
.")\].In a pooled analysis of nine studies including 44,623 participants (20–79 years) with gradable retinal photographs recruited from five countries including Japan, India, and Singapore, a curvilinear relationship between HbA1c and moderate/severe diabetic retinopathy was reported [[28](/article/10.1007/s13300-023-01386-5#ref-CR28 "Colagiuri S, Lee CM, Wong TY, et al. Glycemic thresholds for diabetes-specific retinopathy: implications for diagnostic criteria for diabetes. Diabetes Care. 2011;34(1):145–50. https://doi.org/10.2337/dc10-1206
.")\]. While the prevalence of diabetic retinopathy was negligible for HbA1c < 6.0%, a glycaemic threshold was observed over the range of 6.3–6.7%, with prevalence increasing above these levels. A sensitivity analysis confirmed the same HbA1c threshold (6.4%) in both Asian and European participants. This finding supported the use of an HbA1c value of 6.5% as a diagnostic criterion for diabetes and emphasized the differential relationships between threshold HbA1c values and complications \[[28](/article/10.1007/s13300-023-01386-5#ref-CR28 "Colagiuri S, Lee CM, Wong TY, et al. Glycemic thresholds for diabetes-specific retinopathy: implications for diagnostic criteria for diabetes. Diabetes Care. 2011;34(1):145–50.
https://doi.org/10.2337/dc10-1206
.")\]. In a meta-analysis of recent CVOTs, a 1% decrement in HbA1c achieved with GLP-1 receptor agonists was associated with a 30% risk reduction of major adverse cardiovascular events (MACE; Fig. [1](/article/10.1007/s13300-023-01386-5#Fig1)) \[[29](/article/10.1007/s13300-023-01386-5#ref-CR29 "Nauck MA, Quast DR, Wefers J, Meier JJ. GLP-1 receptor agonists in the treatment of type 2 diabetes—state-of-the-art. Mol Metab. 2021;46:101102.
https://doi.org/10.1016/j.molmet.2020.101102
.")\].Fig. 1
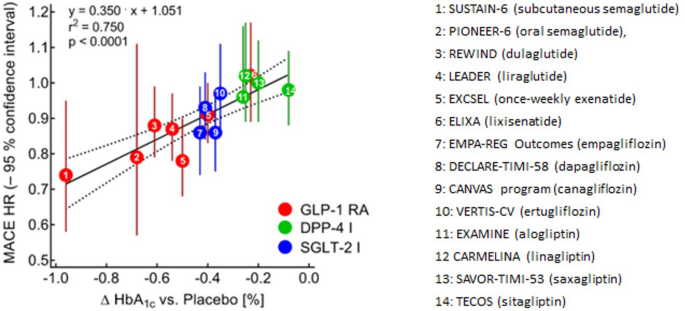
Reduction in HbA1c leads to a significant risk reduction of MACE [[29](/article/10.1007/s13300-023-01386-5#ref-CR29 "Nauck MA, Quast DR, Wefers J, Meier JJ. GLP-1 receptor agonists in the treatment of type 2 diabetes—state-of-the-art. Mol Metab. 2021;46:101102. https://doi.org/10.1016/j.molmet.2020.101102
.")\]. Regression analysis of differences achieved in HbA1c between patients with type 2 diabetes treated with placebo and active drug. Reprinted from Mol Metab, 46:101102, Nauck MA, Quast DR, Wefers J, Meier JJ; GLP-1 receptor agonists in the treatment of type 2 diabetes − state-of-the-art, pg. 13\. © 2021, with permission from Elsevier. _DPP-4 I_ dipeptidyl peptidase 4 inhibitor, _HbA_ _1c_ glycated haemoglobin, _HR_ hazard ratio, _MACE_ major adverse cardiovascular events, _GLP-1 RA_ glucagon-like peptide 1 receptor agonist, _SGLT-2 I_ sodium–glucose cotransporter 2 inhibitorIn the Japan Diabetes Optimal Treatment study for three major risk factors of CVD (J-DOIT3), researchers compared the effects of intensive versus conventional control of multiple risk factors in Japanese patients with T2D (including glycaemia, hypertension, and/or dyslipidaemia) on clinical outcomes [[30](/article/10.1007/s13300-023-01386-5#ref-CR30 "Ueki K, Sasako T, Okazaki Y, et al. Effect of an intensified multifactorial intervention on cardiovascular outcomes and mortality in type 2 diabetes (J-DOIT3): an open-label, randomised controlled trial. Lancet Diabetes Endocrinol. 2017;5(12):951–64. https://doi.org/10.1016/S2213-8587(17)30327-3
.")\]. A total of 2542 patients were randomized to intensive treatment of blood glucose (target HbA1c < 6.2%), blood pressure (target < 120/75 mmHg), and lipids (target low density lipoprotein \[LDL\] cholesterol < 80 mg/dL or < 70 mg/dL in the presence of CAD) or conventional treatment (target HbA1c < 6.9%, blood pressure < 130/80 mmHg and LDL cholesterol < 120 mg/dL or < 100 mg/dL in the presence of CAD). After a median follow-up of 8.5 years, the primary composite outcome (myocardial infarction, stroke, revascularisation, or all-cause mortality) occurred in 109 patients in the intensive treatment group compared with 133 in the conventional treatment group with a non-significant HR of 0.81 (95% CI 0.63, 1.04; _p_ \= 0.094) \[[30](/article/10.1007/s13300-023-01386-5#ref-CR30 "Ueki K, Sasako T, Okazaki Y, et al. Effect of an intensified multifactorial intervention on cardiovascular outcomes and mortality in type 2 diabetes (J-DOIT3): an open-label, randomised controlled trial. Lancet Diabetes Endocrinol. 2017;5(12):951–64.
https://doi.org/10.1016/S2213-8587(17)30327-3
.")\]. However, there was a significant risk reduction in incident stroke (HR 0.42; 95% CI 0.24, 0.74; _p_ \= 0.002) \[[30](/article/10.1007/s13300-023-01386-5#ref-CR30 "Ueki K, Sasako T, Okazaki Y, et al. Effect of an intensified multifactorial intervention on cardiovascular outcomes and mortality in type 2 diabetes (J-DOIT3): an open-label, randomised controlled trial. Lancet Diabetes Endocrinol. 2017;5(12):951–64.
https://doi.org/10.1016/S2213-8587(17)30327-3
.")\] and new-onset or worsening of chronic kidney disease (CKD) (HR 0.68; 95% CI 0.56, 0.82; _p_ < 0.0001) in favour of the intensive treatment group \[[31](/article/10.1007/s13300-023-01386-5#ref-CR31 "Ueki K, Sasako T, Okazaki Y, et al. Multifactorial intervention has a significant effect on diabetic kidney disease in patients with type 2 diabetes. Kidney Int. 2021;99(1):256–66.
https://doi.org/10.1016/j.kint.2020.08.012
.")\].Early Glycaemic Control in T2D: The ‘Legacy’ Effect
In the post-trial monitoring period of the UKPDS, there was an early loss of glycaemic difference between the comparator regimens 1 year after trial discontinuation [[32](/article/10.1007/s13300-023-01386-5#ref-CR32 "Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359(15):1577–89. https://doi.org/10.1056/NEJMoa0806470
.")\]. However, compared with the conventionally treated group, patients with T2D who had lower risk of microvascular complications following intensive glucose management (SU–insulin) continued to have reduced risk in microvascular complications (24%, _p_ \= 0.001) with emergent risk reduction for myocardial infarction (15%, _p_ \= 0.01), diabetes-related death (17%, _p_ \= 0.01), and death from any cause (13%, _p_ \= 0.007) during the 10-year observational period, the so-called legacy effect (Fig. [2](/article/10.1007/s13300-023-01386-5#Fig2)). Among overweight patients treated with metformin, there was also persistent risk reduction for any diabetes-related endpoint (21%, _p_ \= 0.01), myocardial infarction (33%, _p_ \= 0.005), and death from any cause (27%, _p_ \= 0.002) \[[32](/article/10.1007/s13300-023-01386-5#ref-CR32 "Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359(15):1577–89.
https://doi.org/10.1056/NEJMoa0806470
.")\].Fig. 2
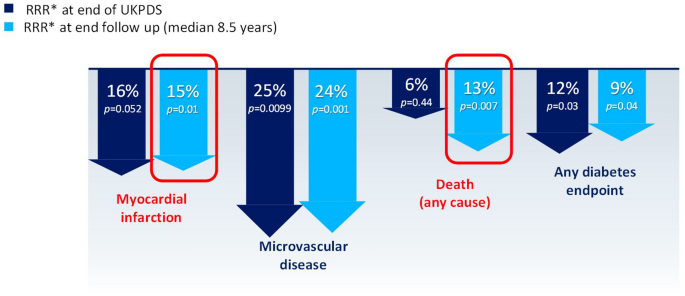
Positive ‘legacy effect’ of intensive glycaemic control [[32](/article/10.1007/s13300-023-01386-5#ref-CR32 "Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359(15):1577–89. https://doi.org/10.1056/NEJMoa0806470
.")\]. Relative risk reductions persisted over the 10-year post-trial period for any diabetes-related endpoints and microvascular complications in patients with type 2 diabetes treated intensively with sulfonylurea–insulin versus conventional treatment in the UKPDS, while risk reductions for myocardial infarction and death from any cause emerged over time, as more events occurred. _RRR_ relative risk reduction, _UKPDS_ United Kingdom Prospective Diabetes StudyThe Vildagliptin Efficacy in combination with metfoRmIn For earlY treatment of T2D (VERIFY) study compared the effects of early dipeptidyl peptidase 4 (DPP4) inhibitor (vildagliptin)–metformin combination therapy versus standard metformin monotherapy on durable glycaemic control in patients with newly or recently diagnosed T2D with 18.6% of patients being of Asian descent [[33](/article/10.1007/s13300-023-01386-5#ref-CR33 "Matthews DR, Paldánius PM, Proot P, et al. Glycaemic durability of an early combination therapy with vildagliptin and metformin versus sequential metformin monotherapy in newly diagnosed type 2 diabetes (VERIFY): a 5-year, multicentre, randomised, double-blind trial. Lancet. 2019;394(10208):1519–29. https://doi.org/10.1016/S0140-6736(19)32131-2
.")\]. In this 5-year study, the intervention group achieved a more durable attainment of HbA1c < 7.0% with lower risk of glycaemic deterioration (HbA1c ≥ 7.0% at two consecutive scheduled visits, 3 months apart) and treatment escalation including insulin than patients treated with initial metformin monotherapy (HR 0.51; 95% CI 0.45, 0.58; _p_ < 0.0001). Subgroup analyses confirmed similar results in Southeast or East Asia, Europe, Latin America, and Africa \[[33](/article/10.1007/s13300-023-01386-5#ref-CR33 "Matthews DR, Paldánius PM, Proot P, et al. Glycaemic durability of an early combination therapy with vildagliptin and metformin versus sequential metformin monotherapy in newly diagnosed type 2 diabetes (VERIFY): a 5-year, multicentre, randomised, double-blind trial. Lancet. 2019;394(10208):1519–29.
https://doi.org/10.1016/S0140-6736(19)32131-2
.")\]. In a sub-analysis of the VERIFY study, the benefit of early combination therapy was observed in both patients with early or late onset of diabetes \[[34](/article/10.1007/s13300-023-01386-5#ref-CR34 "Chan JCN, Paldánius PM, Mathieu C, Stumvoll M, Matthews DR, Del Prato S. Early combination therapy delayed treatment escalation in newly diagnosed young-onset type 2 diabetes: a subanalysis of the VERIFY study. Diabetes Obes Metab. 2021;23(1):245–51.
https://doi.org/10.1111/dom.14192
.")\]. While data from the VERIFY study suggested a risk reduction in time to first adjudicated macrovascular event with vildagliptin–metformin treatment (HR 0.71; 95% CI 0.42, 1.19; _p_ \= 0.19), this trend was based on a small number of events with wide CIs \[[33](/article/10.1007/s13300-023-01386-5#ref-CR33 "Matthews DR, Paldánius PM, Proot P, et al. Glycaemic durability of an early combination therapy with vildagliptin and metformin versus sequential metformin monotherapy in newly diagnosed type 2 diabetes (VERIFY): a 5-year, multicentre, randomised, double-blind trial. Lancet. 2019;394(10208):1519–29.
https://doi.org/10.1016/S0140-6736(19)32131-2
."), [35](/article/10.1007/s13300-023-01386-5#ref-CR35 "Matthews DR, Paldánius PM, Stumvoll M, et al. A pre-specified statistical analysis plan for the VERIFY study: Vildagliptin efficacy in combination with metformin for early treatment of T2DM. Diabetes Obes Metab. 2019;21(10):2240–7.
https://doi.org/10.1111/dom.13800
.")\].The Diabetes and Aging study examined the legacy effect of early glycaemic control on complications and 10-year survival in patients with newly diagnosed T2D in a managed care setting in the USA, which included 6351 Asians (18.3% of the study population) [[36](/article/10.1007/s13300-023-01386-5#ref-CR36 "Laiteerapong N, Ham SA, Gao Y, et al. The legacy effect in type 2 diabetes: impact of early glycemic control on future complications (The Diabetes & Aging Study). Diabetes Care. 2019;42(3):416–26. https://doi.org/10.2337/dc17-1144
.")\]. In this study, an HbA1c ≥ 6.5% during the first year of diagnosis was associated with increased microvascular and macrovascular events in the ensuing 9-year follow-up period compared with an HbA1c < 6.5%, while levels ≥ 7.0% were associated with increased risk of mortality (Fig. [3](/article/10.1007/s13300-023-01386-5#Fig3)) \[[36](/article/10.1007/s13300-023-01386-5#ref-CR36 "Laiteerapong N, Ham SA, Gao Y, et al. The legacy effect in type 2 diabetes: impact of early glycemic control on future complications (The Diabetes & Aging Study). Diabetes Care. 2019;42(3):416–26.
https://doi.org/10.2337/dc17-1144
.")\]. These risk associations had been adjusted for race/ethnicity and other demographic/risk factors. Prolonged exposure to HbA1c levels ≥ 8.0% was associated with substantial increase in risk of microvascular events and mortality. These findings highlight the importance of early and intensive treatment in newly diagnosed patients with T2D to maximize long-term protection \[[36](/article/10.1007/s13300-023-01386-5#ref-CR36 "Laiteerapong N, Ham SA, Gao Y, et al. The legacy effect in type 2 diabetes: impact of early glycemic control on future complications (The Diabetes & Aging Study). Diabetes Care. 2019;42(3):416–26.
https://doi.org/10.2337/dc17-1144
.")\].Fig. 3
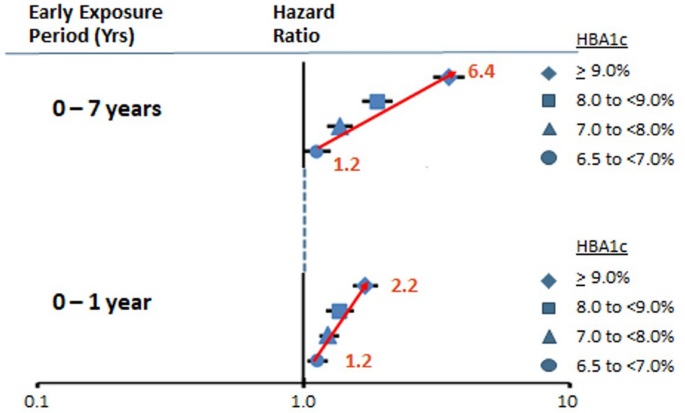
Impact of early glycaemic control in patients with type 2 diabetes on microvascular events [[36](/article/10.1007/s13300-023-01386-5#ref-CR36 "Laiteerapong N, Ham SA, Gao Y, et al. The legacy effect in type 2 diabetes: impact of early glycemic control on future complications (The Diabetes & Aging Study). Diabetes Care. 2019;42(3):416–26. https://doi.org/10.2337/dc17-1144
.")\]. HbA1c < 6.5% was the reference group. During the first year following diagnosis, HbA1c levels ≥ 6.5% were associated with increased microvascular events (based on adjusted hazard ratios shown in red) compared with HbA1c < 6.5%, which persisted during long-term follow-up. Used with permission of American Diabetes Association, from The Legacy Effect in Type 2 Diabetes: Impact of Early Glycemic Control on Future Complications (The Diabetes & Aging Study), Laiteerapong N, et al., Diabetes Care, 42(3) 2019; permission conveyed through Copyright Clearance Center, Inc. _HbA_ _1c_ glycated haemoglobin, _yrs_ yearsThe glycaemic legacy effects on clinical outcomes in T2D was predominantly due to historical HbA1c values, which had greater impact than recent values of HbA1c [[37](/article/10.1007/s13300-023-01386-5#ref-CR37 "Lind M, Imberg H, Coleman RL, Nerman O, Holman RR. Historical HbA1c values may explain the type 2 diabetes legacy effect: UKPDS 88. Diabetes Care. 2021;44(10):2231–7. https://doi.org/10.2337/dc20-2439
.")\]. In an analysis of 20 years of data from 3802 patients with T2D (UKPDS 88), 1% lower HbA1c from diagnosis was associated with an 18.8% (95% CI 21.1, 16.0) risk reduction in all-cause mortality 10–15 years later (Fig. [4](/article/10.1007/s13300-023-01386-5#Fig4)). In contrast, delaying this reduction in HbA1c until 10 years after diagnosis showed seven times lower risk reduction of 2.7% (95% CI 3.1, 2.3). Corresponding risk reduction for myocardial infarction was 19.7% (95% CI 22.4, 16.5) for lowering HbA1c at diagnosis versus 6.5% (95% CI 7.4, 5.3) for achieving glycaemic control 10 years later \[[37](/article/10.1007/s13300-023-01386-5#ref-CR37 "Lind M, Imberg H, Coleman RL, Nerman O, Holman RR. Historical HbA1c values may explain the type 2 diabetes legacy effect: UKPDS 88. Diabetes Care. 2021;44(10):2231–7.
https://doi.org/10.2337/dc20-2439
.")\]. Data from the Diabetes Control and Complications Trial (DCCT) and post-trial Epidemiology of Diabetes Interventions and Complications (EDIC) study also confirmed the legacy effects of early versus late glycaemic control in patients with type 1 diabetes (T1D) \[[38](/article/10.1007/s13300-023-01386-5#ref-CR38 "Lachin JM, Bebu I, Nathan DM, DCCT/EDIC Research Group. The beneficial effects of earlier versus later implementation of intensive therapy in type 1 diabetes. Diabetes Care. 2021;44(10):2225–30.
https://doi.org/10.2337/dc21-1331
.")\].Fig. 4
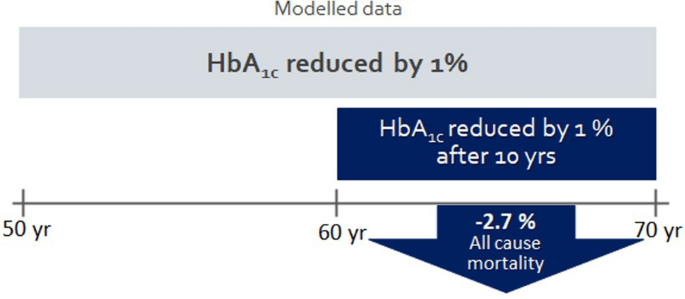
UKPDS 88: Historical HbA1c might explain legacy effect [[37](/article/10.1007/s13300-023-01386-5#ref-CR37 "Lind M, Imberg H, Coleman RL, Nerman O, Holman RR. Historical HbA1c values may explain the type 2 diabetes legacy effect: UKPDS 88. Diabetes Care. 2021;44(10):2231–7. https://doi.org/10.2337/dc20-2439
.")\]. Delayed reduction of HbA1c until 10 years after diagnosis resulted in a seven-fold lower risk reduction (2.7%) of all-cause mortality versus an 18.8% risk reduction achieved by reducing HbA1c by 1% early after diagnosis. _HbA_ _1c_ glycated haemoglobin, _UKPDS_ United Kingdom Prospective Diabetes Study, _yr(s)_ year(s)That said, not all data in patients with T2D supported the legacy effect of early glycaemic control on cardiovascular outcomes, likely owing to differences in study design, settings, interventions, and patient profiles. Other studies, such as Action to Control Cardiovascular Risk in Diabetes (ACCORD), ADVANCE-ON, and the Veterans Affairs Diabetes Trial (VADT), showed less consistent results, although the legacy effects were observed for microvascular complications [[39](#ref-CR39 "Action to Control Cardiovascular Risk in Diabetes Follow-On Eye Study Group. Persistent effects of intensive glycemic control on retinopathy in type 2 diabetes in the Action to Control CardiOvascular Risk in Diabetes (ACCORD) follow-on study. Diabetes Care. 2016;39(7):1089–100. https://doi.org/10.2337/dc16-0024
."),[40](#ref-CR40 "Hayward RA, Reaven PD, Wiitala WL, et al. Follow-up of glycemic control and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2015;372(23):2197–206.
https://doi.org/10.1056/NEJMoa1414266
."),[41](/article/10.1007/s13300-023-01386-5#ref-CR41 "Zoungas S, Chalmers J, Neal B, et al. Follow-up of blood-pressure lowering and glucose control in type 2 diabetes. N Engl J Med. 2014;371(15):1392–406.
https://doi.org/10.1056/NEJMoa1407963
.")\]. In the 10-year post-trial period of VADT, patients with T2D assigned to intensive glycaemic control for 5.6 years had a 17% lower risk of MACE than those assigned to standard therapy, although there was no significant effect on mortality \[[40](/article/10.1007/s13300-023-01386-5#ref-CR40 "Hayward RA, Reaven PD, Wiitala WL, et al. Follow-up of glycemic control and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2015;372(23):2197–206.
https://doi.org/10.1056/NEJMoa1414266
.")\]. In the ADVANCE-ON study, with 37.1% of patients coming from Asia, a risk reduction in all-cause and cardiovascular death in the intensive blood pressure control group persisted, albeit attenuated, in the 6-year post-trial follow-up period \[[41](/article/10.1007/s13300-023-01386-5#ref-CR41 "Zoungas S, Chalmers J, Neal B, et al. Follow-up of blood-pressure lowering and glucose control in type 2 diabetes. N Engl J Med. 2014;371(15):1392–406.
https://doi.org/10.1056/NEJMoa1407963
.")\]. There was no difference in death or macrovascular event rates between the intensive versus standard glycaemic control groups \[[41](/article/10.1007/s13300-023-01386-5#ref-CR41 "Zoungas S, Chalmers J, Neal B, et al. Follow-up of blood-pressure lowering and glucose control in type 2 diabetes. N Engl J Med. 2014;371(15):1392–406.
https://doi.org/10.1056/NEJMoa1407963
.")\].In the post-trial ACCORDION Study, prior intensive glycaemic control during the ACCORD study was associated with a sustained 58% risk reduction in progression diabetic retinopathy compared with standard therapy despite similar HbA1c levels in the post-trial period [[39](/article/10.1007/s13300-023-01386-5#ref-CR39 "Action to Control Cardiovascular Risk in Diabetes Follow-On Eye Study Group. Persistent effects of intensive glycemic control on retinopathy in type 2 diabetes in the Action to Control CardiOvascular Risk in Diabetes (ACCORD) follow-on study. Diabetes Care. 2016;39(7):1089–100. https://doi.org/10.2337/dc16-0024
.")\]. In the ACCORD study, which enrolled high-risk patients with long disease duration \[[42](/article/10.1007/s13300-023-01386-5#ref-CR42 "Action to Control Cardiovascular Risk in Diabetes Study Group, Gerstein HC, Miller ME, et al. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med. 2008;358(24):2545–59.
https://doi.org/10.1056/NEJMoa0802743
.")\], the 22% excess of all-cause mortality and three times higher rates of severe hypoglycaemia with similar MACE at 3.5 years compared with the standard treatment group led to the recommendation of premature trial discontinuation by the Data Safety and Monitoring Committee. The underlying cause for the increased risk of mortality associated with intensive glycaemic control, with some patients receiving five oral GLDs (OGLDs) in addition to insulin, remained to be clarified \[[43](/article/10.1007/s13300-023-01386-5#ref-CR43 "Riddle MC. Counterpoint: intensive glucose control and mortality in ACCORD—still looking for clues. Diabetes Care. 2010;33(12):2722–4.
https://doi.org/10.2337/dc10-1658
.")\]. Meanwhile, results from ACCORD have emphasized the importance of individualized treatment that takes into consideration the risk-to-benefit ratio, especially in high-risk patients.Cardiorenal Risk Reduction in Management of T2D
The cardiorenal protective effects of some GLDs might be mediated by extra-glycaemic mechanisms [[1](/article/10.1007/s13300-023-01386-5#ref-CR1 "Lim LL, Chow E, Chan JCN. Cardiorenal diseases in type 2 diabetes mellitus: clinical trials and real-world practice. Nat Rev Endocrinol. 2023;19(3):151–63. https://doi.org/10.1038/s41574-022-00776-2
.")\], as suggested by exploratory mediation analyses \[[8](/article/10.1007/s13300-023-01386-5#ref-CR8 "Buse JB, Bain SC, Mann JFE, et al. Cardiovascular risk reduction with liraglutide: an exploratory mediation analysis of the LEADER trial. Diabetes Care. 2020;43(7):1546–52.
https://doi.org/10.2337/dc19-2251
."), [10](/article/10.1007/s13300-023-01386-5#ref-CR10 "Konig M, Riddle MC, Colhoun HM, et al. Exploring potential mediators of the cardiovascular benefit of dulaglutide in type 2 diabetes patients in REWIND. Cardiovasc Diabetol. 2021;20(1):194.
https://doi.org/10.1186/s12933-021-01386-4
.")\]. Using data from the Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER) study, it was estimated that HbA1c reduction mediated only 41% of the beneficial effects of liraglutide, a GLP-1 receptor agonist, on MACE with urinary albumin-to-creatinine ratio being another important contributor \[[8](/article/10.1007/s13300-023-01386-5#ref-CR8 "Buse JB, Bain SC, Mann JFE, et al. Cardiovascular risk reduction with liraglutide: an exploratory mediation analysis of the LEADER trial. Diabetes Care. 2020;43(7):1546–52.
https://doi.org/10.2337/dc19-2251
.")\]. In the LEADER study, 10% of patients were of Asian ethnicity and 9% of the study population were enrolled in Asia \[[44](/article/10.1007/s13300-023-01386-5#ref-CR44 "Marso SP, Poulter NR, Nissen SE, et al. Design of the liraglutide effect and action in diabetes: evaluation of cardiovascular outcome results (LEADER) trial. Am Heart J. 2013;166(5):823-30 e5.
https://doi.org/10.1016/j.ahj.2013.07.012
.")\]. In the Researching Cardiovascular Events With a Weekly Incretin in Diabetes (REWIND) Study, treatment with dulaglutide, another GLP-1 receptor agonist, reduced MACE by 36.1% compared with placebo, with reduced HbA1c being a partial mediator for these benefits \[[10](/article/10.1007/s13300-023-01386-5#ref-CR10 "Konig M, Riddle MC, Colhoun HM, et al. Exploring potential mediators of the cardiovascular benefit of dulaglutide in type 2 diabetes patients in REWIND. Cardiovasc Diabetol. 2021;20(1):194.
https://doi.org/10.1186/s12933-021-01386-4
.")\]. In this study, 1.5% of the study population came from Asia \[[45](/article/10.1007/s13300-023-01386-5#ref-CR45 "Gerstein HC, Colhoun HM, Dagenais GR, et al. Design and baseline characteristics of participants in the Researching cardiovascular Events with a Weekly INcretin in Diabetes (REWIND) trial on the cardiovascular effects of dulaglutide. Diabetes Obes Metab. 2018;20(1):42–9.
https://doi.org/10.1111/dom.13028
.")\].In an earlier meta-analysis of CVOTs, both SGLT2 inhibitors and GLP-1 receptor agonists were associated with a 14% reduction in MACE in patients with T2D, with the benefit limited to those with established CVD [[46](/article/10.1007/s13300-023-01386-5#ref-CR46 "Giugliano D, Maiorino MI, Bellastella G, Chiodini P, Esposito K. Glycemic control, preexisting cardiovascular disease, and risk of major cardiovascular events in patients with type 2 diabetes mellitus: systematic review with meta-analysis of cardiovascular outcome trials and intensive glucose control trials. J Am Heart Assoc. 2019;8(12):e012356. https://doi.org/10.1161/JAHA.119.012356
.")\]. Subsequent meta-analyses including more studies confirmed that SGLT2 inhibitors reduced the risk of MACE by 10% (HR 0.90; 95% CI 0.85, 0.95) \[[47](/article/10.1007/s13300-023-01386-5#ref-CR47 "McGuire DK, Shih WJ, Cosentino F, et al. Association of SGLT2 inhibitors with cardiovascular and kidney outcomes in patients with type 2 diabetes: a meta-analysis. JAMA Cardiol. 2021;6(2):148–58.
https://doi.org/10.1001/jamacardio.2020.4511
.")\] and GLP-1 receptor agonists by 14% (HR 0.86, 95% CI 0.79, 0.94; _p_ \= 0.006) \[[9](/article/10.1007/s13300-023-01386-5#ref-CR9 "Giugliano D, Scappaticcio L, Longo M, et al. GLP-1 receptor agonists and cardiorenal outcomes in type 2 diabetes: an updated meta-analysis of eight CVOTs. Cardiovasc Diabetol. 2021;20(1):189.
https://doi.org/10.1186/s12933-021-01366-8
.")\]. A sub-analysis suggested that GLP-1 receptor agonists might confer greater therapeutic benefits in patients with CVD, who had a relative risk reduction of 16% compared with 6% in those without CVD \[[9](/article/10.1007/s13300-023-01386-5#ref-CR9 "Giugliano D, Scappaticcio L, Longo M, et al. GLP-1 receptor agonists and cardiorenal outcomes in type 2 diabetes: an updated meta-analysis of eight CVOTs. Cardiovasc Diabetol. 2021;20(1):189.
https://doi.org/10.1186/s12933-021-01366-8
.")\]. In a meta-analysis performed in Asian patients, both SGLT2 inhibitors and GLP-1 receptor agonists reduced the risk of MACE, with SGLT2 inhibitors conferring greater risk reduction for renal events in Asian patients than in non-Asian patients \[[48](/article/10.1007/s13300-023-01386-5#ref-CR48 "Kadowaki T, Yamamoto F, Taneda Y, et al. Effects of anti-diabetes medications on cardiovascular and kidney outcomes in Asian patients with type 2 diabetes: a rapid evidence assessment and narrative synthesis. Expert Opin Drug Saf. 2021;20(6):707–20.
https://doi.org/10.1080/14740338.2021.1898585
.")\].Despite these encouraging results, the cardiorenal risk reduction approach to the management of T2D needs to be interpreted in a broader context. Results from these CVOTs have limited generalisability since the majority of trial participants had CVD or multiple cardiovascular risk factors, which is not representative of the wider diabetes population. These CVOTs provided only a short timeline for assessing benefits and harm. Studies lasting less than 5 years were unlikely to detect risks that might emerge only after many years, especially for drugs with complex mechanisms of action. Importantly, both the intervention and control groups had similar glycaemic control, which did not allow evaluation of the HbA1c-reducing effects of different GLDs in reducing clinical outcomes [[49](/article/10.1007/s13300-023-01386-5#ref-CR49 "Cefalu WT, Kaul S, Gerstein HC, et al. Cardiovascular outcomes trials in type 2 diabetes: where do we go from here? Reflections from a Diabetes Care Editors’ Expert Forum. Diabetes Care. 2018;41(1):14–31. https://doi.org/10.2337/dci17-0057
.")\].Need for a Balanced Treatment Approach in T2D
Given that the majority of patients with diabetes have not yet developed cardiorenal events and on the basis of consistent evidence from randomized clinical trials (RCTs) and epidemiological analysis, notably that from UKPDS [[4](/article/10.1007/s13300-023-01386-5#ref-CR4 "Stratton IM, Adler AI, Neil HA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321(7258):405–12. https://doi.org/10.1136/bmj.321.7258.405
."), [20](/article/10.1007/s13300-023-01386-5#ref-CR20 "UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352(9131):837–53."), [26](/article/10.1007/s13300-023-01386-5#ref-CR26 "UK Prospective Diabetes Study Group. Ethnicity and cardiovascular disease. The incidence of myocardial infarction in white, South Asian, and Afro-Caribbean patients with type 2 diabetes (U.K. Prospective Diabetes Study 32). Diabetes Care. 1998;21(8):1271–7.
https://doi.org/10.2337/diacare.21.8.1271
."), [32](/article/10.1007/s13300-023-01386-5#ref-CR32 "Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359(15):1577–89.
https://doi.org/10.1056/NEJMoa0806470
."), [37](/article/10.1007/s13300-023-01386-5#ref-CR37 "Lind M, Imberg H, Coleman RL, Nerman O, Holman RR. Historical HbA1c values may explain the type 2 diabetes legacy effect: UKPDS 88. Diabetes Care. 2021;44(10):2231–7.
https://doi.org/10.2337/dc20-2439
.")\], ADVANCE \[[23](/article/10.1007/s13300-023-01386-5#ref-CR23 "Perkovic V, Heerspink HL, Chalmers J, et al. Intensive glucose control improves kidney outcomes in patients with type 2 diabetes. Kidney Int. 2013;83(3):517–23.
https://doi.org/10.1038/ki.2012.401
."), [25](/article/10.1007/s13300-023-01386-5#ref-CR25 "Zoungas S, Chalmers J, Ninomiya T, et al. Association of HbA1c levels with vascular complications and death in patients with type 2 diabetes: evidence of glycaemic thresholds. Diabetologia. 2012;55(3):636–43.
https://doi.org/10.1007/s00125-011-2404-1
."), [27](/article/10.1007/s13300-023-01386-5#ref-CR27 "ADVANCE Collaborative Group, Patel A, MacMahon S, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358(24):2560–72.
https://doi.org/10.1056/NEJMoa0802987
.")\], and VERIFY \[[33](#ref-CR33 "Matthews DR, Paldánius PM, Proot P, et al. Glycaemic durability of an early combination therapy with vildagliptin and metformin versus sequential metformin monotherapy in newly diagnosed type 2 diabetes (VERIFY): a 5-year, multicentre, randomised, double-blind trial. Lancet. 2019;394(10208):1519–29.
https://doi.org/10.1016/S0140-6736(19)32131-2
."),[34](#ref-CR34 "Chan JCN, Paldánius PM, Mathieu C, Stumvoll M, Matthews DR, Del Prato S. Early combination therapy delayed treatment escalation in newly diagnosed young-onset type 2 diabetes: a subanalysis of the VERIFY study. Diabetes Obes Metab. 2021;23(1):245–51.
https://doi.org/10.1111/dom.14192
."),[35](/article/10.1007/s13300-023-01386-5#ref-CR35 "Matthews DR, Paldánius PM, Stumvoll M, et al. A pre-specified statistical analysis plan for the VERIFY study: Vildagliptin efficacy in combination with metformin for early treatment of T2DM. Diabetes Obes Metab. 2019;21(10):2240–7.
https://doi.org/10.1111/dom.13800
.")\], glycaemic control should be achieved early and safely with treatment goals close to near normal value. All patients with diabetes should receive a structured education program on lifestyle modification, notably diet and exercise, and self-management. In obese people with T2D diagnosed for less than 6 years, weight loss of at least 15 kg might lead to remission of diabetes for 2 years \[[50](/article/10.1007/s13300-023-01386-5#ref-CR50 "Lean MEJ, Leslie WS, Barnes AC, et al. Durability of a primary care-led weight-management intervention for remission of type 2 diabetes: 2-year results of the DiRECT open-label, cluster-randomised trial. Lancet Diabetes Endocrinol. 2019;7(5):344–55.
https://doi.org/10.1016/S2213-8587(19)30068-3
.")\]. However, the majority of patients with T2D, especially those with long disease duration, will need medications to control glycaemia. Here, metformin, SUs, DPP4 inhibitors, SGLT2 inhibitors, and GLP-1 receptor agonists have all been proven to be safe, efficacious, and effective in reducing blood glucose \[[51](/article/10.1007/s13300-023-01386-5#ref-CR51 "American Diabetes Association Professional Practice Committee. 9. Pharmacologic approaches to glycemic treatment: standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S125–S43.
https://doi.org/10.2337/dc22-S009
.")\], although the newer GLDs are substantially more expensive. Thus, in patients without cardiorenal complications, physicians should consider selecting GLDs with the lowest acquisition cost to increase accessibility and affordability, even in patients with multiple risk factors or complications, such as those enrolled in the CVOTs, in which the benefits of newer GLDs were evaluated against background therapies, such as metformin, SUs, statins, and renin–angiotensin–aldosterone system inhibitors. These drugs are affordable and have proven to confer organ-protective effects, which contributed to the improved outcomes in these CVOTs \[[52](/article/10.1007/s13300-023-01386-5#ref-CR52 "Harris SB, Cheng AYY, Davies MJ, Gerstein HC, Green JB, Skolnik N. In person-centered, outcomes-driven treatment: a new paradigm for type 2 diabetes in primary care. Arlington: American Diabetes Association; 2020.")\]. The effectiveness of these background therapies was supported by real-world evidence in Asian patients \[[53](/article/10.1007/s13300-023-01386-5#ref-CR53 "Yang A, Lau ESH, Wu H, et al. Attenuated risk association of end-stage kidney disease with metformin in type 2 diabetes with eGFR categories 1–4. Pharmaceuticals (Basel). 2022;15(9):1140.
https://doi.org/10.3390/ph15091140
."), [54](/article/10.1007/s13300-023-01386-5#ref-CR54 "Yang A, Shi M, Lau ESH, et al. Clinical outcomes following discontinuation of renin-angiotensin-system inhibitors in patients with type 2 diabetes and advanced chronic kidney disease: a prospective cohort study. EClinicalMedicine. 2023;55: 101751.
https://doi.org/10.1016/j.eclinm.2022.101751
.")\]. Using an RCT design, the J-DOIT3 study also confirmed that by using these highly affordable medications to effectively control HbA1c, blood pressure, and lipids, it was possible to achieve extremely low cardiovascular and renal event rates in Asian patients with T2D \[[30](/article/10.1007/s13300-023-01386-5#ref-CR30 "Ueki K, Sasako T, Okazaki Y, et al. Effect of an intensified multifactorial intervention on cardiovascular outcomes and mortality in type 2 diabetes (J-DOIT3): an open-label, randomised controlled trial. Lancet Diabetes Endocrinol. 2017;5(12):951–64.
https://doi.org/10.1016/S2213-8587(17)30327-3
."), [31](/article/10.1007/s13300-023-01386-5#ref-CR31 "Ueki K, Sasako T, Okazaki Y, et al. Multifactorial intervention has a significant effect on diabetic kidney disease in patients with type 2 diabetes. Kidney Int. 2021;99(1):256–66.
https://doi.org/10.1016/j.kint.2020.08.012
.")\].Practice guidelines from the American Diabetes Association (ADA), the European Association for the Study of Diabetes (EASD), and the Korean Diabetes Association recommend that selection of second-line therapy for T2D (following first-line metformin and lifestyle changes) should be based on patient assessment for atherosclerosis and CVD (ASCVD), heart failure, or CKD [[14](/article/10.1007/s13300-023-01386-5#ref-CR14 "Davies MJ, Aroda VR, Collins BS, et al. Management of hyperglycemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022;45(11):2753–86. https://doi.org/10.2337/dci22-0034
."), [51](/article/10.1007/s13300-023-01386-5#ref-CR51 "American Diabetes Association Professional Practice Committee. 9. Pharmacologic approaches to glycemic treatment: standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S125–S43.
https://doi.org/10.2337/dc22-S009
."), [55](/article/10.1007/s13300-023-01386-5#ref-CR55 "Hur KY, Moon MK, Park JS, et al. 2021 clinical practice guidelines for diabetes mellitus of the Korean Diabetes Association. Diabetes Metab J. 2021;45(4):461–81.
https://doi.org/10.4093/dmj.2021.0156
.")\]. Updated ADA practice guidelines are shown in Fig. [5](/article/10.1007/s13300-023-01386-5#Fig5). For patients with ASCVD, an SGLT2 inhibitor or GLP-1 receptor agonist is recommended, while an SGLT2 inhibitor is recommended for those with CKD or heart failure, independent of metformin use and HbA1c at baseline \[[14](/article/10.1007/s13300-023-01386-5#ref-CR14 "Davies MJ, Aroda VR, Collins BS, et al. Management of hyperglycemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022;45(11):2753–86.
https://doi.org/10.2337/dci22-0034
."), [51](/article/10.1007/s13300-023-01386-5#ref-CR51 "American Diabetes Association Professional Practice Committee. 9. Pharmacologic approaches to glycemic treatment: standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S125–S43.
https://doi.org/10.2337/dc22-S009
.")\]. The Kidney Disease: Improving Global Outcomes (KDIGO) Diabetes Work Group also recommend that SGLT2 inhibitors in combination with metformin should be considered as first-line therapy in patients with T2D and CKD, with additional drug therapy for glycaemic control as needed \[[56](/article/10.1007/s13300-023-01386-5#ref-CR56 "Rossing P, Caramori ML, Chan JCN, et al. Executive summary of the KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease: an update based on rapidly emerging new evidence. Kidney Int. 2022;102(5):990–9.
https://doi.org/10.1016/j.kint.2022.06.013
.")\].Fig. 5
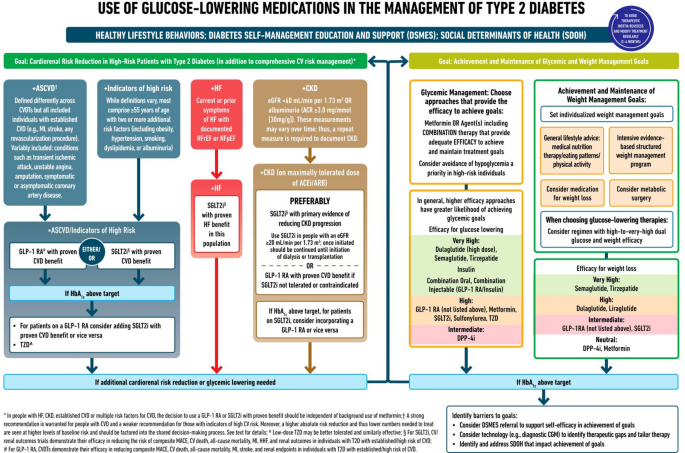
Use of glucose-lowering medications in the management of T2D [[14](/article/10.1007/s13300-023-01386-5#ref-CR14 "Davies MJ, Aroda VR, Collins BS, et al. Management of hyperglycemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022;45(11):2753–86. https://doi.org/10.2337/dci22-0034
.")\]. _ACEi_ angiotensin-converting enzyme inhibitor, _ACR_ albumin/creatinine ratio, _ARB_ angiotensin receptor blocker, _ASCVD_ atherosclerotic cardiovascular disease, _CGM_ continuous glucose monitoring, _CKD_ chronic kidney disease, _CV_ cardiovascular, _CVD_ cardiovascular disease, _CVOT_ cardiovascular outcomes trial, _DPP-4i_ dipeptidyl peptidase 4 inhibitor, _eGFR_ estimated glomerular filtration rate, _GLP-1 RA_ glucagon-like peptide 1 receptor agonist, _HbA_ _1c_ glycated haemoglobin, _HF_ heart failure, _HFpEF_ heart failure with preserved ejection fraction, _HFrEF_ heart failure with reduced ejection fraction, _HHF_ hospitalization for heart failure, _MACE_ major adverse cardiovascular events, _MI_ myocardial infarction, _SDOH_ social determinants of health, _SGLT2i_ sodium–glucose cotransporter 2 inhibitor, _T2D_ type 2 diabetes, _TZD_ thiazolidinedione. Used with permission of American Diabetes Association and the European Association for the Study of Diabetes, from Management of Hyperglycemia in Type 2 Diabetes, 2022\. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD), Davies MJ, et al., Diabetes Care, 45(11) 2022; permission conveyed through Copyright Clearance Center, Inc.The International Diabetes Federation (IDF) has adopted a pragmatic approach by reviewing available guidelines and integrating the recommendations applicable to primary care settings around the world [[15](/article/10.1007/s13300-023-01386-5#ref-CR15 "International Diabetes Federation. IDF clinical practice recommendations for managing type 2 diabetes in primary care. 2017. https://idf.org/e-library/guidelines/128-idf-clinical-practice-recommendations-for-managing-type-2-diabetes-in-primary-care.html
. Accessed 19 Jan 2023.")\]. The IDF practice guidelines recommended using the A-B-C-D approach for choosing second-line treatment after metformin, where A stands for age (young patients might benefit from lower HbA1c goals); B for body weight (overweight/obese patients might benefit from treatments with weight-neutral or weight-loss effects); C for complications (patients with CKD or CVD might benefit from treatments with organ-protective effects); and D for duration (patients with long disease duration are likely to have complications and required treatment adjustment, including the use of insulin) \[[15](/article/10.1007/s13300-023-01386-5#ref-CR15 "International Diabetes Federation. IDF clinical practice recommendations for managing type 2 diabetes in primary care. 2017.
https://idf.org/e-library/guidelines/128-idf-clinical-practice-recommendations-for-managing-type-2-diabetes-in-primary-care.html
. Accessed 19 Jan 2023.")\]. This tailored approach is also supported by the recommendations of the Japanese \[[17](/article/10.1007/s13300-023-01386-5#ref-CR17 "Araki E, Goto A, Kondo T, et al. Japanese clinical practice guideline for diabetes 2019. Diabetol Int. 2020;11(3):165–223.
https://doi.org/10.1007/s13340-020-00439-5
.")\], Chinese \[[16](/article/10.1007/s13300-023-01386-5#ref-CR16 "Jia W, Weng J, Zhu D, et al. Standards of medical care for type 2 diabetes in China 2019. Diabetes Metab Res Rev. 2019;35(6):e3158.
https://doi.org/10.1002/dmrr.3158
.")\], and Korean \[[55](/article/10.1007/s13300-023-01386-5#ref-CR55 "Hur KY, Moon MK, Park JS, et al. 2021 clinical practice guidelines for diabetes mellitus of the Korean Diabetes Association. Diabetes Metab J. 2021;45(4):461–81.
https://doi.org/10.4093/dmj.2021.0156
.")\] practice guidelines (Table [2](/article/10.1007/s13300-023-01386-5#Tab2)).Table 2 Individual considerations when choosing glucose-lowering therapy, according to practice guidelines from the International Diabetes Federation [[15](/article/10.1007/s13300-023-01386-5#ref-CR15 "International Diabetes Federation. IDF clinical practice recommendations for managing type 2 diabetes in primary care. 2017. https://idf.org/e-library/guidelines/128-idf-clinical-practice-recommendations-for-managing-type-2-diabetes-in-primary-care.html
. Accessed 19 Jan 2023.")], Japan [[17](/article/10.1007/s13300-023-01386-5#ref-CR17 "Araki E, Goto A, Kondo T, et al. Japanese clinical practice guideline for diabetes 2019. Diabetol Int. 2020;11(3):165–223. https://doi.org/10.1007/s13340-020-00439-5
.")], China [[16](/article/10.1007/s13300-023-01386-5#ref-CR16 "Jia W, Weng J, Zhu D, et al. Standards of medical care for type 2 diabetes in China 2019. Diabetes Metab Res Rev. 2019;35(6):e3158. https://doi.org/10.1002/dmrr.3158
.")] and Korea [[55](/article/10.1007/s13300-023-01386-5#ref-CR55 "Hur KY, Moon MK, Park JS, et al. 2021 clinical practice guidelines for diabetes mellitus of the Korean Diabetes Association. Diabetes Metab J. 2021;45(4):461–81. https://doi.org/10.4093/dmj.2021.0156
.")] using an ‘ABCD’ approach taking into consideration the risk of hypoglycaemia
New Real-World Evidence on Use of SUs in Asia: The JADE Register
Establishing diabetes registers can identify care gaps, prioritise interventions, benchmark performance, and promote collaborative research [[57](/article/10.1007/s13300-023-01386-5#ref-CR57 "Chan JCN, Lim LL, Luk AOY, et al. From Hong Kong Diabetes register to JADE program to RAMP-DM for data-driven actions. Diabetes Care. 2019;42(11):2022–31. https://doi.org/10.2337/dci19-0003
."), [58](/article/10.1007/s13300-023-01386-5#ref-CR58 "Lim LL, Lau ESH, Ozaki R, et al. Association of technologically assisted integrated care with clinical outcomes in type 2 diabetes in Hong Kong using the prospective JADE Program: a retrospective cohort analysis. PLoS Med. 2020;17(10):e1003367.
https://doi.org/10.1371/journal.pmed.1003367
.")\]. The Joint Asia Diabetes Evaluation (JADE) Register comprises a web-based portal with protocols to guide data collection during structured comprehensive assessment (blood/urine tests and eye/foot examination), performed every 12–24 months, as recommended by most practice guidelines \[[57](/article/10.1007/s13300-023-01386-5#ref-CR57 "Chan JCN, Lim LL, Luk AOY, et al. From Hong Kong Diabetes register to JADE program to RAMP-DM for data-driven actions. Diabetes Care. 2019;42(11):2022–31.
https://doi.org/10.2337/dci19-0003
."), [58](/article/10.1007/s13300-023-01386-5#ref-CR58 "Lim LL, Lau ESH, Ozaki R, et al. Association of technologically assisted integrated care with clinical outcomes in type 2 diabetes in Hong Kong using the prospective JADE Program: a retrospective cohort analysis. PLoS Med. 2020;17(10):e1003367.
https://doi.org/10.1371/journal.pmed.1003367
.")\]. Since 2007, the JADE Register had enrolled at least 120,000 patients from 11 Asian countries/areas, including China, India, Thailand, Malaysia, Singapore, Korea, Taiwan, Hong Kong, Vietnam, Philippines, and Indonesia \[[59](/article/10.1007/s13300-023-01386-5#ref-CR59 "Lim LL, Lau ESH, Cheung JTK, et al. Real-world usage of sulphonylureas in Asian patients with type 2 diabetes using the Joint Asia Diabetes Evaluation (JADE) register. Diabetes Obes Metab. 2023;25(1):208–21.
https://doi.org/10.1111/dom.14865
.")\].In a retrospective cross-sectional analysis of the JADE Register, researchers closed the data gap regarding the pattern of SU usage and related patient profiles in Asia (Fig. 6) [[59](/article/10.1007/s13300-023-01386-5#ref-CR59 "Lim LL, Lau ESH, Cheung JTK, et al. Real-world usage of sulphonylureas in Asian patients with type 2 diabetes using the Joint Asia Diabetes Evaluation (JADE) register. Diabetes Obes Metab. 2023;25(1):208–21. https://doi.org/10.1111/dom.14865
.")\]. After exclusion of patients with T1D, patients with T2D treated with insulin or injectable GLP-1 receptor agonists, and patients without information on medications, 62,512 patients with T2D enrolled between 2007 and 2019 were analysed. Of these, 54,783 were treated with OGLDs and 7729 with lifestyle modification only. Patients treated with OGLDs had a mean age at registration of 57.3 years, a median disease duration of 5 years, and 54% were men. At enrolment, 42% of patients had an HbA1c < 7.0%, 14% had CKD, and 9% had CAD. Fewer than 10% of patients reported hypoglycaemic events at least monthly in the 3 months prior to registration. Approximately 60% of patients were treated with SUs (_n_ \= 32,558). Amongst all patients treated with OGLDs, SUs were used alone (9.0%) or in combination with other OGLDs (50.4%), mainly metformin (30.6%) or metformin plus DPP4 inhibitors (9.2%) \[[59](/article/10.1007/s13300-023-01386-5#ref-CR59 "Lim LL, Lau ESH, Cheung JTK, et al. Real-world usage of sulphonylureas in Asian patients with type 2 diabetes using the Joint Asia Diabetes Evaluation (JADE) register. Diabetes Obes Metab. 2023;25(1):208–21.
https://doi.org/10.1111/dom.14865
.")\]. In these patients, who were recruited by more than 300 practitioners from a broad range of care settings in Asia, gliclazide was used in almost half of the SU users. Gliclazide was the most commonly used SU in Hong Kong, Malaysia, and Singapore. Glimepiride was most commonly used in India, Indonesia, and Taiwan. Both gliclazide and glimepiride were equally used in China, while glibenclamide and glipizide were commonly used in Thailand. Amongst patients treated with gliclazide (_n_ \= 15,312), 40% had an HbA1c < 7.0%, 18% had CKD, and 10% had CAD at registration. Of the gliclazide users, two-thirds had received two OGLDs, with 78% receiving concomitant metformin. Amongst SU-treated patients, gliclazide users were 9% more likely to have an HbA1c < 7% and had a 19% lower risk of self-reported hypoglycaemia (after adjustment for covariables such as countries/areas and year of recruitment) (Fig. [6](/article/10.1007/s13300-023-01386-5#Fig6)) \[[59](/article/10.1007/s13300-023-01386-5#ref-CR59 "Lim LL, Lau ESH, Cheung JTK, et al. Real-world usage of sulphonylureas in Asian patients with type 2 diabetes using the Joint Asia Diabetes Evaluation (JADE) register. Diabetes Obes Metab. 2023;25(1):208–21.
https://doi.org/10.1111/dom.14865
.")\].Fig. 6
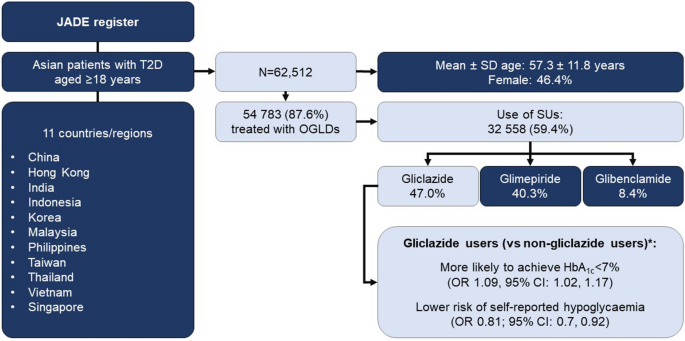
Summary of real-world evidence on the use of sulfonylureas in Asian patients with type 2 diabetes from the Joint Asia Diabetes Evaluation (JADE) Register [[59](/article/10.1007/s13300-023-01386-5#ref-CR59 "Lim LL, Lau ESH, Cheung JTK, et al. Real-world usage of sulphonylureas in Asian patients with type 2 diabetes using the Joint Asia Diabetes Evaluation (JADE) register. Diabetes Obes Metab. 2023;25(1):208–21. https://doi.org/10.1111/dom.14865
.")\]. \*Adjusted for sociodemographic factors, cardiometabolic risk factors, medication use, country/region, and year of registration. _CI_ confidence interval, _HbA_ _1c_ glycated haemoglobin, _OGLD_ oral glucose-lowering drugs, _OR_ odds ratio, _SD_ standard deviation, _SUs_ sulfonylureas, _T2D_ type 2 diabetesConclusions
In patients with T2D, hyperglycaemia increases the risks of complications and premature mortality. Early glycaemic control, especially with the use of combination therapy, has legacy effects in preventing complications and premature mortality in later life. Both glucocentric and cardiorenal risk reduction approaches are needed to alter the trajectory of T2D, improve outcomes, and preserve quality of life. Every person with diabetes has a unique risk profile, highlighting the need for individualization of glucose-lowering regimens and treatment targets, as recommended by most practice guidelines, including those from Asia where treatment affordability is an important consideration. While newer GLDs have been proven to reduce cardiorenal events in high-risk patients, older GLDs such as metformin and SUs (e.g. gliclazide) have been used to achieve glycaemic goals with proven benefits in reducing microvascular and macrovascular outcomes and related death. Given the large population affected by T2D, older GLDs, which are affordable even in resource-limited settings and endorsed by the World Health Organization (WHO) [[60](/article/10.1007/s13300-023-01386-5#ref-CR60 "World Health Organization. Global report on diabetes: executive summary. 2016. https://www.who.int/publications/i/item/9789241565257
. Accessed 7 Feb 2023.")\], are important components of the armamentarium for the management of T2D. This is further supported by the new real-world data from the JADE Register, where SUs were commonly used (often in combination with metformin) and the use of gliclazide was associated with an increased likelihood of achieving an HbA1c < 7.0% and a lower risk of self-reported hypoglycaemia compared with other SUs. Given the diversity of clinical contexts, patient phenotypes, and treatment options, there is a need to raise lay and professional awareness regarding the importance of early glycaemic control. Furthermore, there is an urgent need to improve care delivery to assess patients, gather data systematically, and personalize treatment taking into consideration risks, benefits, treatment costs, and patient preference, to improve outcomes \[[61](/article/10.1007/s13300-023-01386-5#ref-CR61 "Chan JCN, Lim LL, Wareham NJ, et al. The Lancet Commission on diabetes: using data to transform diabetes care and patient lives. Lancet. 2021;396(10267):2019–82.
https://doi.org/10.1016/S0140-6736(20)32374-6
.")\].References
- Lim LL, Chow E, Chan JCN. Cardiorenal diseases in type 2 diabetes mellitus: clinical trials and real-world practice. Nat Rev Endocrinol. 2023;19(3):151–63. https://doi.org/10.1038/s41574-022-00776-2.
Article CAS PubMed Google Scholar - International Diabetes Federation. IDF Diabetes Atlas, 10th ed. 2021. https://diabetesatlas.org/. Accessed 20 Jan 2023.
- Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H, Al Kaabi J. Epidemiology of type 2 diabetes—global burden of disease and forecasted trends. J Epidemiol Glob Health. 2020;10(1):107–11. https://doi.org/10.2991/jegh.k.191028.001.
Article PubMed PubMed Central Google Scholar - Stratton IM, Adler AI, Neil HA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321(7258):405–12. https://doi.org/10.1136/bmj.321.7258.405.
Article CAS PubMed PubMed Central Google Scholar - Aschner P, Gagliardino JJ, Ilkova H, et al. Persistent poor glycaemic control in individuals with type 2 diabetes in developing countries: 12 years of real-world evidence of the International Diabetes Management Practices Study (IDMPS). Diabetologia. 2020;63(4):711–21. https://doi.org/10.1007/s00125-019-05078-3.
Article CAS PubMed PubMed Central Google Scholar - Einarson TR, Acs A, Ludwig C, Panton UH. Prevalence of cardiovascular disease in type 2 diabetes: a systematic literature review of scientific evidence from across the world in 2007–2017. Cardiovasc Diabetol. 2018;17(1):83. https://doi.org/10.1186/s12933-018-0728-6.
Article PubMed PubMed Central Google Scholar - Smith RJ, Goldfine AB, Hiatt WR. Evaluating the cardiovascular safety of new medications for type 2 diabetes: time to reassess? Diabetes Care. 2016;39(5):738–42. https://doi.org/10.2337/dc15-2237.
Article PubMed Google Scholar - Buse JB, Bain SC, Mann JFE, et al. Cardiovascular risk reduction with liraglutide: an exploratory mediation analysis of the LEADER trial. Diabetes Care. 2020;43(7):1546–52. https://doi.org/10.2337/dc19-2251.
Article CAS PubMed PubMed Central Google Scholar - Giugliano D, Scappaticcio L, Longo M, et al. GLP-1 receptor agonists and cardiorenal outcomes in type 2 diabetes: an updated meta-analysis of eight CVOTs. Cardiovasc Diabetol. 2021;20(1):189. https://doi.org/10.1186/s12933-021-01366-8.
Article CAS PubMed PubMed Central Google Scholar - Konig M, Riddle MC, Colhoun HM, et al. Exploring potential mediators of the cardiovascular benefit of dulaglutide in type 2 diabetes patients in REWIND. Cardiovasc Diabetol. 2021;20(1):194. https://doi.org/10.1186/s12933-021-01386-4.
Article CAS PubMed PubMed Central Google Scholar - Khunti K, Bellary S, Karamat MA, et al. Representation of people of South Asian origin in cardiovascular outcome trials of glucose-lowering therapies in type 2 diabetes. Diabet Med. 2017;34(1):64–8. https://doi.org/10.1111/dme.13103.
Article CAS PubMed Google Scholar - Lee MMY, Ghouri N, McGuire DK, Rutter MK, Sattar N. Meta-analyses of results from randomized outcome trials comparing cardiovascular effects of SGLT2is and GLP-1RAs in Asian versus White patients with and without type 2 diabetes. Diabetes Care. 2021;44(5):1236–41. https://doi.org/10.2337/dc20-3007.
Article CAS PubMed Google Scholar - American Diabetes Association Professional Practice Committee. 6. Glycemic targets: Standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S83–S96. https://doi.org/10.2337/dc22-S006.
- Davies MJ, Aroda VR, Collins BS, et al. Management of hyperglycemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022;45(11):2753–86. https://doi.org/10.2337/dci22-0034.
Article CAS PubMed Google Scholar - International Diabetes Federation. IDF clinical practice recommendations for managing type 2 diabetes in primary care. 2017. https://idf.org/e-library/guidelines/128-idf-clinical-practice-recommendations-for-managing-type-2-diabetes-in-primary-care.html. Accessed 19 Jan 2023.
- Jia W, Weng J, Zhu D, et al. Standards of medical care for type 2 diabetes in China 2019. Diabetes Metab Res Rev. 2019;35(6):e3158. https://doi.org/10.1002/dmrr.3158.
Article PubMed Google Scholar - Araki E, Goto A, Kondo T, et al. Japanese clinical practice guideline for diabetes 2019. Diabetol Int. 2020;11(3):165–223. https://doi.org/10.1007/s13340-020-00439-5.
Article PubMed PubMed Central Google Scholar - Khunti K, Davies M, Majeed A, Thorsted BL, Wolden ML, Paul SK. Hypoglycemia and risk of cardiovascular disease and all-cause mortality in insulin-treated people with type 1 and type 2 diabetes: a cohort study. Diabetes Care. 2015;38(2):316–22. https://doi.org/10.2337/dc14-0920.
Article PubMed Google Scholar - Mohan V, Khunti K, Chan SP, et al. Management of type 2 diabetes in developing countries: balancing optimal glycaemic control and outcomes with affordability and accessibility to treatment. Diabetes Ther. 2020;11(1):15–35. https://doi.org/10.1007/s13300-019-00733-9.
Article PubMed Google Scholar - UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352(9131):837–53.
- Chen YY, Lin YJ, Chong E, et al. The impact of diabetes mellitus and corresponding HbA1c levels on the future risks of cardiovascular disease and mortality: a representative cohort study in Taiwan. PLoS ONE. 2015;10(4):e0123116. https://doi.org/10.1371/journal.pone.0123116.
Article CAS PubMed PubMed Central Google Scholar - Elley CR, Kenealy T, Robinson E, Drury PL. Glycated haemoglobin and cardiovascular outcomes in people with type 2 diabetes: a large prospective cohort study. Diabet Med. 2008;25(11):1295–301. https://doi.org/10.1111/j.1464-5491.2008.02581.x.
Article CAS PubMed Google Scholar - Perkovic V, Heerspink HL, Chalmers J, et al. Intensive glucose control improves kidney outcomes in patients with type 2 diabetes. Kidney Int. 2013;83(3):517–23. https://doi.org/10.1038/ki.2012.401.
Article CAS PubMed Google Scholar - Sakurai M, Saitoh S, Miura K, et al. HbA1c and the risks for all-cause and cardiovascular mortality in the general Japanese population: NIPPON DATA90. Diabetes Care. 2013;36(11):3759–65. https://doi.org/10.2337/dc12-2412.
Article CAS PubMed PubMed Central Google Scholar - Zoungas S, Chalmers J, Ninomiya T, et al. Association of HbA1c levels with vascular complications and death in patients with type 2 diabetes: evidence of glycaemic thresholds. Diabetologia. 2012;55(3):636–43. https://doi.org/10.1007/s00125-011-2404-1.
Article CAS PubMed Google Scholar - UK Prospective Diabetes Study Group. Ethnicity and cardiovascular disease. The incidence of myocardial infarction in white, South Asian, and Afro-Caribbean patients with type 2 diabetes (U.K. Prospective Diabetes Study 32). Diabetes Care. 1998;21(8):1271–7. https://doi.org/10.2337/diacare.21.8.1271.
- ADVANCE Collaborative Group, Patel A, MacMahon S, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358(24):2560–72. https://doi.org/10.1056/NEJMoa0802987.
- Colagiuri S, Lee CM, Wong TY, et al. Glycemic thresholds for diabetes-specific retinopathy: implications for diagnostic criteria for diabetes. Diabetes Care. 2011;34(1):145–50. https://doi.org/10.2337/dc10-1206.
Article PubMed Google Scholar - Nauck MA, Quast DR, Wefers J, Meier JJ. GLP-1 receptor agonists in the treatment of type 2 diabetes—state-of-the-art. Mol Metab. 2021;46:101102. https://doi.org/10.1016/j.molmet.2020.101102.
Article CAS PubMed Google Scholar - Ueki K, Sasako T, Okazaki Y, et al. Effect of an intensified multifactorial intervention on cardiovascular outcomes and mortality in type 2 diabetes (J-DOIT3): an open-label, randomised controlled trial. Lancet Diabetes Endocrinol. 2017;5(12):951–64. https://doi.org/10.1016/S2213-8587(17)30327-3.
Article PubMed Google Scholar - Ueki K, Sasako T, Okazaki Y, et al. Multifactorial intervention has a significant effect on diabetic kidney disease in patients with type 2 diabetes. Kidney Int. 2021;99(1):256–66. https://doi.org/10.1016/j.kint.2020.08.012.
Article CAS PubMed Google Scholar - Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359(15):1577–89. https://doi.org/10.1056/NEJMoa0806470.
Article CAS PubMed Google Scholar - Matthews DR, Paldánius PM, Proot P, et al. Glycaemic durability of an early combination therapy with vildagliptin and metformin versus sequential metformin monotherapy in newly diagnosed type 2 diabetes (VERIFY): a 5-year, multicentre, randomised, double-blind trial. Lancet. 2019;394(10208):1519–29. https://doi.org/10.1016/S0140-6736(19)32131-2.
Article CAS PubMed Google Scholar - Chan JCN, Paldánius PM, Mathieu C, Stumvoll M, Matthews DR, Del Prato S. Early combination therapy delayed treatment escalation in newly diagnosed young-onset type 2 diabetes: a subanalysis of the VERIFY study. Diabetes Obes Metab. 2021;23(1):245–51. https://doi.org/10.1111/dom.14192.
Article CAS PubMed Google Scholar - Matthews DR, Paldánius PM, Stumvoll M, et al. A pre-specified statistical analysis plan for the VERIFY study: Vildagliptin efficacy in combination with metformin for early treatment of T2DM. Diabetes Obes Metab. 2019;21(10):2240–7. https://doi.org/10.1111/dom.13800.
Article PubMed PubMed Central Google Scholar - Laiteerapong N, Ham SA, Gao Y, et al. The legacy effect in type 2 diabetes: impact of early glycemic control on future complications (The Diabetes & Aging Study). Diabetes Care. 2019;42(3):416–26. https://doi.org/10.2337/dc17-1144.
Article CAS PubMed Google Scholar - Lind M, Imberg H, Coleman RL, Nerman O, Holman RR. Historical HbA1c values may explain the type 2 diabetes legacy effect: UKPDS 88. Diabetes Care. 2021;44(10):2231–7. https://doi.org/10.2337/dc20-2439.
Article CAS PubMed PubMed Central Google Scholar - Lachin JM, Bebu I, Nathan DM, DCCT/EDIC Research Group. The beneficial effects of earlier versus later implementation of intensive therapy in type 1 diabetes. Diabetes Care. 2021;44(10):2225–30. https://doi.org/10.2337/dc21-1331.
- Action to Control Cardiovascular Risk in Diabetes Follow-On Eye Study Group. Persistent effects of intensive glycemic control on retinopathy in type 2 diabetes in the Action to Control CardiOvascular Risk in Diabetes (ACCORD) follow-on study. Diabetes Care. 2016;39(7):1089–100. https://doi.org/10.2337/dc16-0024.
- Hayward RA, Reaven PD, Wiitala WL, et al. Follow-up of glycemic control and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2015;372(23):2197–206. https://doi.org/10.1056/NEJMoa1414266.
Article CAS PubMed Google Scholar - Zoungas S, Chalmers J, Neal B, et al. Follow-up of blood-pressure lowering and glucose control in type 2 diabetes. N Engl J Med. 2014;371(15):1392–406. https://doi.org/10.1056/NEJMoa1407963.
Article CAS PubMed Google Scholar - Action to Control Cardiovascular Risk in Diabetes Study Group, Gerstein HC, Miller ME, et al. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med. 2008;358(24):2545–59. https://doi.org/10.1056/NEJMoa0802743.
- Riddle MC. Counterpoint: intensive glucose control and mortality in ACCORD—still looking for clues. Diabetes Care. 2010;33(12):2722–4. https://doi.org/10.2337/dc10-1658.
- Marso SP, Poulter NR, Nissen SE, et al. Design of the liraglutide effect and action in diabetes: evaluation of cardiovascular outcome results (LEADER) trial. Am Heart J. 2013;166(5):823-30 e5. https://doi.org/10.1016/j.ahj.2013.07.012.
Article CAS PubMed Google Scholar - Gerstein HC, Colhoun HM, Dagenais GR, et al. Design and baseline characteristics of participants in the Researching cardiovascular Events with a Weekly INcretin in Diabetes (REWIND) trial on the cardiovascular effects of dulaglutide. Diabetes Obes Metab. 2018;20(1):42–9. https://doi.org/10.1111/dom.13028.
Article CAS PubMed Google Scholar - Giugliano D, Maiorino MI, Bellastella G, Chiodini P, Esposito K. Glycemic control, preexisting cardiovascular disease, and risk of major cardiovascular events in patients with type 2 diabetes mellitus: systematic review with meta-analysis of cardiovascular outcome trials and intensive glucose control trials. J Am Heart Assoc. 2019;8(12):e012356. https://doi.org/10.1161/JAHA.119.012356.
Article CAS PubMed PubMed Central Google Scholar - McGuire DK, Shih WJ, Cosentino F, et al. Association of SGLT2 inhibitors with cardiovascular and kidney outcomes in patients with type 2 diabetes: a meta-analysis. JAMA Cardiol. 2021;6(2):148–58. https://doi.org/10.1001/jamacardio.2020.4511.
Article PubMed Google Scholar - Kadowaki T, Yamamoto F, Taneda Y, et al. Effects of anti-diabetes medications on cardiovascular and kidney outcomes in Asian patients with type 2 diabetes: a rapid evidence assessment and narrative synthesis. Expert Opin Drug Saf. 2021;20(6):707–20. https://doi.org/10.1080/14740338.2021.1898585.
Article CAS PubMed Google Scholar - Cefalu WT, Kaul S, Gerstein HC, et al. Cardiovascular outcomes trials in type 2 diabetes: where do we go from here? Reflections from a Diabetes Care Editors’ Expert Forum. Diabetes Care. 2018;41(1):14–31. https://doi.org/10.2337/dci17-0057.
Article CAS PubMed Google Scholar - Lean MEJ, Leslie WS, Barnes AC, et al. Durability of a primary care-led weight-management intervention for remission of type 2 diabetes: 2-year results of the DiRECT open-label, cluster-randomised trial. Lancet Diabetes Endocrinol. 2019;7(5):344–55. https://doi.org/10.1016/S2213-8587(19)30068-3.
Article PubMed Google Scholar - American Diabetes Association Professional Practice Committee. 9. Pharmacologic approaches to glycemic treatment: standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S125–S43. https://doi.org/10.2337/dc22-S009.
- Harris SB, Cheng AYY, Davies MJ, Gerstein HC, Green JB, Skolnik N. In person-centered, outcomes-driven treatment: a new paradigm for type 2 diabetes in primary care. Arlington: American Diabetes Association; 2020.
Google Scholar - Yang A, Lau ESH, Wu H, et al. Attenuated risk association of end-stage kidney disease with metformin in type 2 diabetes with eGFR categories 1–4. Pharmaceuticals (Basel). 2022;15(9):1140. https://doi.org/10.3390/ph15091140.
Article CAS PubMed Google Scholar - Yang A, Shi M, Lau ESH, et al. Clinical outcomes following discontinuation of renin-angiotensin-system inhibitors in patients with type 2 diabetes and advanced chronic kidney disease: a prospective cohort study. EClinicalMedicine. 2023;55: 101751. https://doi.org/10.1016/j.eclinm.2022.101751.
Article PubMed Google Scholar - Hur KY, Moon MK, Park JS, et al. 2021 clinical practice guidelines for diabetes mellitus of the Korean Diabetes Association. Diabetes Metab J. 2021;45(4):461–81. https://doi.org/10.4093/dmj.2021.0156.
Article PubMed PubMed Central Google Scholar - Rossing P, Caramori ML, Chan JCN, et al. Executive summary of the KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease: an update based on rapidly emerging new evidence. Kidney Int. 2022;102(5):990–9. https://doi.org/10.1016/j.kint.2022.06.013.
Article PubMed Google Scholar - Chan JCN, Lim LL, Luk AOY, et al. From Hong Kong Diabetes register to JADE program to RAMP-DM for data-driven actions. Diabetes Care. 2019;42(11):2022–31. https://doi.org/10.2337/dci19-0003.
Article PubMed Google Scholar - Lim LL, Lau ESH, Ozaki R, et al. Association of technologically assisted integrated care with clinical outcomes in type 2 diabetes in Hong Kong using the prospective JADE Program: a retrospective cohort analysis. PLoS Med. 2020;17(10):e1003367. https://doi.org/10.1371/journal.pmed.1003367.
Article PubMed PubMed Central Google Scholar - Lim LL, Lau ESH, Cheung JTK, et al. Real-world usage of sulphonylureas in Asian patients with type 2 diabetes using the Joint Asia Diabetes Evaluation (JADE) register. Diabetes Obes Metab. 2023;25(1):208–21. https://doi.org/10.1111/dom.14865.
Article CAS PubMed Google Scholar - World Health Organization. Global report on diabetes: executive summary. 2016. https://www.who.int/publications/i/item/9789241565257. Accessed 7 Feb 2023.
- Chan JCN, Lim LL, Wareham NJ, et al. The Lancet Commission on diabetes: using data to transform diabetes care and patient lives. Lancet. 2021;396(10267):2019–82. https://doi.org/10.1016/S0140-6736(20)32374-6.
Article PubMed Google Scholar