Colon Cancer Treatment & Management: Approach Considerations, Surgical Care, Ablation (original) (raw)
Approach Considerations
Surgery is the only curative modality for localized colon cancer (stage I-III). Surgical resection potentially provides the only curative option for patients with limited metastatic disease in liver and/or lung (stage IV disease), but the proper use of elective colon resections in nonobstructed patients with stage IV disease is a source of continuing debate.
Adjuvant chemotherapy is standard for patients with stage III disease. Its use in stage II disease is controversial, but current guidelines recommend its use in selected patients with risk factors for recurrence. [1, 89] At present, the role of radiation therapy is limited to palliative therapy for selected metastatic sites such as bone or brain metastases.
Chemotherapy rather than surgery has been the standard management for patients with metastatic colorectal cancer. Biologic agents have assumed a major role in the treatment of metastatic cases, with selection increasingly guided by genetic analysis of the tumor. The proper use of elective colon/rectal resections in nonobstructed patients with stage IV disease is a source of continuing debate.
For more information, see Colon Cancer Treatment Protocols.
![]()
Surgical Care
Surgery is the only curative modality for localized colon cancer (stage I-III) and potentially provides the only curative option for patients with limited metastatic disease in liver and/or lung (stage IV disease). The general principles for all operations include removal of the primary tumor with adequate margins including areas of lymphatic drainage. Standard colectomies for adenocarcinoma of the colon are depicted in the image below.
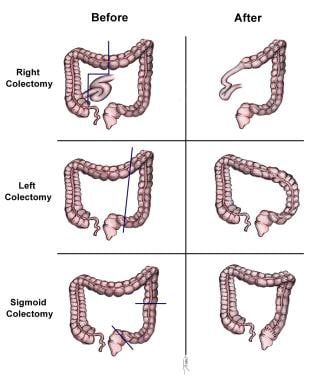
Standard colectomies for adenocarcinoma of the colon.
For lesions in the cecum and right colon, a right hemicolectomy is indicated. During a right hemicolectomy, the ileocolic, right colic, and right branch of the middle colic vessels are divided and removed. Care must be taken to identify the right ureter, the ovarian or testicular vessels, and the duodenum. If the omentum is attached to the tumor, it should be removed en bloc with the specimen.
For lesions in the proximal or middle transverse colon, an extended right hemicolectomy can be performed. In this procedure, the ileocolic, right colic, and middle colic vessels are divided and the specimen is removed with its mesentery.
For lesions in the splenic flexure and left colon, a left hemicolectomy is indicated. The left branch of the middle colic vessels, the inferior mesenteric vein, and the left colic vessels along with their mesenteries are included with the specimen.
For sigmoid colon lesions, a sigmoid colectomy is appropriate. The inferior mesenteric artery is divided at its origin, and dissection proceeds toward the pelvis until adequate margins are obtained. Care must be taken during dissection to identify the left ureter and the left ovarian or testicular vessels.
Total abdominal colectomy with ileorectal anastomosis may be required for patients with any of the following:
- Hereditary nonpolyposis colon cancer syndrome (HNPCC; Lynch syndrome)
- Attenuated familial adenomatous polyposis (FAP)
- Metachronous cancers in separate colon segments
Total abdominal colectomy may also be indicated for some patients with acute malignant colon obstructions in whom the status of the proximal bowel is unknown.
Laparoscopic surgery
The advent of laparoscopy has revolutionized the surgical approach to colonic resections for cancers. Large prospective randomized trials have found no significant differences between open and laparoscopic colectomy with regard to intraoperative or postoperative complications, perioperative mortality rates, readmission or reoperation rates, or rate of surgical wound recurrence. Oncologic outcomes (cause-specific survival, disease recurrence, number of lymph nodes harvested) are likewise comparable. [90, 91, 92, 93, 94, 95]
For example, the Clinical Outcomes of Surgical Therapy Study Group trial found no significant differences between laparoscopic-assisted colectomy (LAC) or open colectomy in terms of 5-year disease-free survival rate (69% versus 68% in the LAC and open colectomy groups, respectively) or overall survival (76% versus 75%). [91] In a study by Lacy et al with median followup of 95 months, LAC was more effective than open colectomy, although the tendency toward higher cancer-related and overall survival did not reach statistical significance. [94]
Surgery guidelines
American Society of Colon and Rectal Surgeons practice parameters for the management of colon cancer recommend colectomy as the primary treatment for localized resectable colon cancer. [96] Additional recommendations are as follows:
- The extent of resection of the colon should correspond to the lymphovascular drainage of the site of the colon cancer; the lymphadenectomy should be complete and en bloc with the bowel segment
- Clinically positive lymph nodes located outside the standard field of resection that are suspected to contain metastatic disease should be biopsied or removed at the time of primary resection
- Resection of involved adjacent organs should be en bloc
National Comprehensive Cancer Network (NCCN) guidelines also recommend colectomy, with en bloc removal of regional lymph nodes, for treatment of resectable, nonobstructing colon cancer. [78] In addition, for clinical T4b disease, neoadjuvant chemotherapy may be considered. The NCCN states that laparoscopic-assisted colectomy may be considered, based upon the following criteria:
- The surgeon has experience performing laparoscopically assisted colorectal operations
- No locally advanced disease, acute bowel obstruction, or perforation from cancer is present
- Thorough abdominal exploration is required
- Preoperative marking of small lesions should be considered
NCCN recommendations for lymphadenectomy are as follows [78] :
- Lymph nodes at the origin of feeding vessel should be identified for pathologic exam
- Clinically positive lymph nodes outside the field of resection that are considered suspicious should be biopsied or removed, if possible
- Positive nodes left behind indicate an incomplete (R2) resection
- A minimum of 12 lymph nodes need to be examined to establish N stage
European Society for Medical Oncology (ESMO) recommendations for surgical treatment of localized colon cancer include the following [97] :
- For noninvasive adenocarcinomas (pTis—ie, intraepithelial or intramucosal), en bloc endoscopic resection of the polyp is sufficient
- Invasive carcinoma (pT1) in a polyp requires a thorough review with the pathologist and surgeon. High-risk features mandating surgical resection with lymphadenectomy include lymphatic or venous invasion, grade 3 differentiation, and significant (grade >1) tumor budding
- Laparoscopic colectomy can be safe when technical expertise is available, in the absence of contraindications
- Obstructive colon cancers can be treated in one- or two-stage procedures, as indicated
Metastatic colorectal cancer
Chemotherapy rather than surgery has been the standard management for patients with metastatic colorectal cancer. The proper use of elective colon/rectal resections in nonobstructed patients with stage IV disease is a source of continuing debate.
Medical oncologists properly note that palliative resection has major drawbacks, such as loss of performance status and risks of surgical complications that potentially lead to delay in chemotherapy. However, surgeons understand that elective operations have lower morbidity than emergent operations on patients who are receiving chemotherapy.
There is a trend toward nonsurgical management of patients with asymptomatic, surgically incurable colorectal cancer, with studies showing that fewer than 10% of these patients subsequently require surgery for obstruction or perforation. [98, 99] A review by Venderbosch et al found that resection of the primary tumor appears to improve survival in patients with stage IV colorectal cancer, but these researchers concluded that prospective studies are warranted, given the potential bias of those results. [100]
Curative-intent resections of liver metastases have significantly improved long-term survival, with acceptable postoperative morbidity, including in older patients. [101] A study by Brouquet et al found that resection of colorectal liver metastases after a second-line chemotherapy regimen was safe and provided a modest hope for definitive cure, making this approach viable in patients with advanced colorectal liver metastases. [102]
Hepatic arterial infusion (HAI) of chemotherapeutic agents such as floxuridine (FUDR) is a consideration following partial hepatectomy. A study by House et al found that adjuvant HAI-FUDR combined with modern systemic chemotherapy resulted in improved survival compared with adjuvant chemotherapy alone. [103]
Colonic stents have introduced an effective method of palliation for obstruction in patients with unresectable liver metastasis. However, a study by van Hooft et al found that colonic stenting has no decisive clinical advantages compared with emergency surgery. Although it may be used as an alternative treatment in undefined sets of patients, concerns about tumor spread caused by perforations remains. [104]
![]()
Ablation
Although resection is the only potentially curative treatment for patients with colon metastases, other therapeutic options for those who are not surgical candidates include thermal ablation techniques. Cryotherapy uses probes to freeze tumors and surrounding hepatic parenchyma. It requires laparotomy and can potentially result in significant morbidity, including liver cracking, thrombocytopenia, and disseminated intravascular coagulation (DIC).
Radiofrequency ablation (RFA) uses probes that heat liver tumors and the surrounding margin of tissue to create coagulation necrosis. RFA can be performed percutaneously, laparoscopically, or through an open approach. Although RFA has minimal morbidity, local recurrence is a significant problem and correlates with tumor size.
![]()
Pharmacotherapy
Analysis of a data set assembled by the Adjuvant Colon Cancer Endpoints group showed that adjuvant chemotherapy provides a significant disease-free survival benefit in stage II and III colon cancer because it reduces the recurrence rate. The benefit was particularly evident within the first 2 years of adjuvant therapy but some benefit extended to years 3-4. [105]
The standard chemotherapy for patients with stage III and some patients with stage II colon cancer has for decades consisted of 5-fluorouracil (5-FU) in combination with adjuncts such as levamisole and leucovorin. [1, 2, 3, 4] This approach was tested in several large randomized trials and was shown to reduce individual 5-year risk of cancer recurrence and death by about 30%.
Capecitabine (Xeloda) has also become a standard option. Like 5-FU, capecitabine is a fluoropyrimidine, but is given orally rather than intravenously; it undergoes a three-step enzymatic conversion to 5-FU, with the last step occurring in the tumor cell. [1] The randomized X-ACT study demonstrated the noninferiority of capecitabine compared with 5-FU/leucovorin as adjuvant therapy for patients with stage III colon cancer, with efficacy benefits maintained at 5 years and in older patients. [106]
The addition of oxaliplatin to fluoropyrimidine-based therapy has also become standard. A phase III trial in 1886 patients with resected stage III colon cancer reported superior overall survival with capecitabine plus oxaliplatin (XELOX, or CapeOx) versus 5-FU/leucovorin (73% vs 67%, respectively; P = 0.04) after a median follow-up of almost 7 years. The results of that study suggested that low tumor expression of dihydropyrimidine dehydrogenase may be predictive for XELOX efficacy. [107] Similarly, the large MOSAIC trial demonstrated significant improvement in 5-year disease-free survival and 6-year disease-free survival for patients with stage III colon cancer when oxaliplatin was added to 5-FU/leucovorin (ie, FOLFOX4). [108]
Elderly patients
In an observational study of 1291 patients with stage III colon cancer, 56% of whom received adjuvant chemotherapy, van Erning et al concluded that adjuvant chemotherapy should be considered in elderly patients with stage III disease. Adjuvant chemotherapy reduced the risk of distant recurrence after surgery by about half in both elderly patients and younger ones. With adjuvant chemotherapy, hazard ratios for distant recurrence were 0.50 in patients < 75 years of age and 0.57 in those 75 years and older. [109]
Therapy duration
In the International Duration Evaluation of Adjuvant Chemotherapy (IDEA) trial (n=12,834), which compared 3 versus 6 months of FOLFOX (fluorouracil, leucovorin, and oxaliplatin) or XELOX, 3-year disease-free survival in the FOLFOX 3-month arm was lower than that in the 6-month arm by 0.9% (hazard ratio [HR], 1.07; 95% confidence interval [CI], 1.00 - 1.15). To meet the prespecified noninferiority threshold, the upper limit of the 95% CI had to be 1.12 or less, so noninferiority was not established. However, shorter therapy was associated with significantly less neurotoxicity. Rates of neurotoxicity were 17% versus 48% with 3 versus 6 months, respectively, of FOLFOX; comparable figures with XELOX were 15% and 45%, respectively; P < 0.0001). [110]
An American Society of Clinical Oncology (ASCO) guideline on adjuvant chemotherapy with oxaliplatin and a fluoropyrimidine for patients with resected stage III colon cancer recommends offering adjuvant chemotherapy for a duration of 6 months for patients at a high risk of recurrence (T4 and/or N2). For patients at a low risk of recurrence (T1, T2, or T3 and N1), either 6 months or 3 months of chemotherapy may be offered. [111]
For patients with stage III colon cancer, National Comprehensive Cancer Network (NCCN) guidelines also recommend basing adjuvant treatment duration on risk status, as follows [78] :
- Low-risk stage III (pathologic stages T1-3/N1): CapeOx for 3 months or FOLFOX for 3 to 6 months
- High-risk stage III disease (pathologic stages T4/N1-2 and anyT/N2): CapeOx for 3 to 6 months or FOLFOX for 6 months
Adjuvant therapy in stage II colon cancer
The role of adjuvant chemotherapy for stage II colon cancer is controversial. [1] Surgery alone is usually curative for stage II colon cancer, but approximately 20-30% of these patients develop tumor recurrence and ultimately die of metastatic disease.
A large European trial (QUASAR) demonstrated small but significant benefit (3.6%) in terms of absolute 5-year survival rate for those patients who received 5-FU/leucovorin versus those in the control group. [112] In contrast, a study by O’Connor et al found that in Medicare patients with stage II colon cancer, with or without poor prognostic features, overall survival was not substantially improved by adjuvant chemotherapy. [113]
ASCO recommends against the routine use of adjuvant chemotherapy in patients with stage II colon cancer who are at low risk of recurrence, including in younger patients. [89] However, ASCO recommends offering adjuvant chemotherapy to patients with stage IIB colon cancer (ie, T4) and stage IIC colon cancer (ie, lesions either penetrating visceral peritoneum or invasive of surrounding organ), with a discussion of the potential benefits and risks of harm. In addition, ASCO suggests offering adjuvant therapy to patients with stage IIA colon cancer who have any of the following high-risk factors (with consideration of the number of risk factors as part of the shared decision-making process, since the presence of more than one risk factor may increase the risk of recurrence):
- Sampling of fewer than 12 lymph nodes in the surgical specimen
- Perineural or lymphovascular invasion
- Poorly differentiated or undifferentiated tumor grade
- Intestinal obstruction
- Tumor perforation
- Grade BD3 tumor budding (≥ 10 buds)
ASCO guidelines do not routinely recommend the addition of oxaliplatin to fluoropyrimidine-based adjuvant therapy, but consider that it may be offered as a result of shared decision making. ASCO recommends against routinely offering adjuvant therapy to patients with mismatch repair deficiency/microsatellite instability (dMMR/MSI) tumors, but if the combination of dMMR/MSI and high-risk factors results in a decision to offer adjuvant therapy, ASCO recommends including oxaliplatin in the chemotherapy regimen.
A comparison of 3 versus 6 months of FOLFOX or CapeOx adjuvant chemotherapy in 1254 patients with high-risk stage II resected colorectal cancer found that neurotoxicity was approximately 5 times lower in the 3-month arm than the 6-month arm. Noninferiority of 3 months of therapy was not shown for 5-year relapse-free survival. However, a possible regimen effect was observed, suggesting that either 3 months of CapeOx or 6 months of FOLFOX therapy can be used when an oxaliplatin doublet is indicated for treatment of patients with stage II colorectal cancer. [114]
Ongoing adjuvant trials are investigating additional risk stratification of stage II colon cancer based on clinicopathological and molecular markers. For example, the ECOG 5202 trial is studying the addition of bevacizumab to adjuvant therapy with 5-FU, leucovorin, and oxaliplatin in high-risk patients, with low-risk patients undergoing observation only. In this trial, high-risk patients are defined as those with microsatellite stability (MSS) or low-frequency microsatellite instability (MSI-L) and loss of heterozygosity at 18q. Low-risk patients are those with MSS or MSI-L and retention of 18q, or high-frequency MSI with or without loss of heterozygosity at 18q.
Therapy for metastatic disease
Combination regimens provide improved efficacy and prolonged progression-free survival (PFS) in patients with metastatic colon cancer. The advent of new classes of active drugs and biologics for colorectal cancer has improved the expected survival for patients with metastatic disease.
In a phase III multicenter trial in patients with advanced colorectal carcinoma refractory to fluorouracil, overall survival did not significantly differ between patients treated with FOLFOX4 (n=246) compared with irinotecan (n=245); however, FOLFOX 4 improved response rate (RR) and time to progression (TTP) compared with irinotecan (P=0.0009 for each RR and TTP). FOLFOX4 was associated with more neutropenia and paresthesias. [115]
Although many patients with colorectal cancer are elderly, exclusion of these patients from randomized controlled trials has impeded the creation of evidence-based guidelines for this population. A study by Seymour et al demonstrated that elderly and frail patients with untreated metastatic colorectal cancer can participate in a randomized controlled trial. Study patients, who were considered unfit for full-dose chemotherapy, underwent a comprehensive health assessment and were started on chemotherapy at 80% of standard doses. [116]
In 2015, the US Food and Drug Administration (FDA) approved trifluridine/tipiracil (Lonsurf) for metastatic colorectal cancer. Trifluridine is a nucleoside analog that inhibits cell proliferation by incorporating into DNA and interering with DNA synthesis; tipiracil inhibits the metabolism of trifluridine. The efficacy and safety of trifluridine/tipiracil were evaluated in the phase III RECOURSE trial, an international, randomized, double-blind study involving 800 patients with previously treated metastatic colorectal cancer. Patients had received chemotherapy with a fluoropyrimidine, oxaliplatin, irinotecan, bevacizumab, and—for patients with KRAS wild-type tumors—cetuximab or panitumumab. The primary efficacy end point of the study was median overall survival, which was 7.1 months with trifluridine/tipiracil vs 5.3 months with placebo (P < 0.001). The secondary end point was PFS, which was 2 months with trifluridine/tipiracil vs 1.7 months with placebo. [117]
In 2023, the FDA approved trifluridine/tipiracil in combination with bevacizumab for metastatic colorectal cancer in adults previously treated with fluoropyrimidine-, oxaliplatin-, and irinotecan-based chemotherapy, an anti–vascular endothelial growth factor (VEGF) biologic therapy, and if RAS wild-type, anti–epidermal growth factor receptor (EGFR) therapy.
Approval was based on the results from the phase III SUNLIGHT trial, in which 246 patients received either trifluridine/tipiracil plus bevacizumab (combination group) or trifluridine–tipiracil alone (FTD–TPI group). The median overall survival was 10.8 months in the combination group and 7.5 months in the FTD–TPI group (P < 0.001). The median PFS was 5.6 months in the combination group and 2.4 months in the FTD–TPI group (P < 0.001). [118]
Biologic agents
Targeted therapy with biologic agents, based on molecular characteristics of the tumor, have become a standard part of treatment for metastatic colon cancer. Biologic agents used for targeted therapy include monoclonal antibodies against epidermal growth factor receptors (EGFR), vascular endothelial growth factor (VEGF), and cytotoxic T-lymphocyte antigen 4 (CTL4), as well as a variety of tyrosine kinase inhibitors. Such agents include the following:
- Bevacizumab (Avastin)
- Cetuximab (Erbitux)
- Encorafenib (Braftovi)
- Entrectinib (Rozlytrek)
- Fruquintinib (Fruzaqla)
- Ipilimumab (Yervoy)
- Larotrectinib (Vitrakvi)
- Panitumumab (Vectibix)
- Ramucirumab (Cyramza)
- Regorafenib (Stivarga)
- Tucatinib (Tukysa)
- Ziv-aflibercept (Zaltrap)
Detection of microsatellite instability (MSI) has also become important for treatment for metastatic colorectal cancers. Tumors with MSI tend to respond favorably to biologic therapy with immune checkpoint inhibitors (eg, pembrolizumab, nivolumab). These tumors typically have high expression of checkpoint proteins, including programmed death 1 (PD-1) and programmed death ligand 1 (PD-L1), which interfere with the body’s antitumor T-cell response. By disabling these proteins, checkpoint inhibitors enable T cells to kill tumor cells. [119]
For patients with deficient mismatch repair (dMMR)/MSI-H tumors who are not eligible for cytotoxic combinations, National Comprehensive Cancer Network (NCCN) guidelines recommend the following as first-line immunotherapy options [78] :
- Nivolumab
- Pembrolizumab
- Nivolumab plus ipilimumab
The NCCN recommends nivolumab with or without ipilimumab or pembrolizumab for the second- and third-line treatment of patients with dMMR/MSI-H colorectal cancer.
Besides determining the status of MMR and/or MSI, the NCCN has expanded its recommendation for biomarker testing to include KRAS/RAS or BRAF mutations, HER2 amplifications, and NTRK fusions in patients with metastatic colorectal cancer. The determination of these tumor markers provides more treatment options for these patients. [78]
Bevacizumab
Bevacizumab is a humanized monoclonal antibody to VEGF. It was the first anti-angiogenesis drug to be approved in clinical practice and its first indication was for metastatic colorectal cancer. Approval was based on a pivotal trial that demonstrated improved PFS and overall survival when bevacizumab was added to chemotherapy with irinotecan, 5-FU, and leucovorin (IFL).
Bevacizumab, in combination with fluorouracil-based chemotherapy, is indicated for first- and second-line treatment of metastatic colorectal carcinoma. Bevacizumab is also approved for second-line treatment in patients who have progressed on a first-line bevacizumab-containing regimen.
Approval for continuation treatment was based on a study that showed maintenance of VEGF inhibition with bevacizumab plus standard second-line chemotherapy. The risk of death was reduced by 19% for those who received bevacizumab in combination with standard chemotherapy in both the first- and second-line compared with those who received chemotherapy alone (hazard ratio [HR]=0.81, P=0.0057). PFS improved by 32% (HR=0.68, P < 0.0001). [120]
A pooled analysis of cohorts of older patients (aged 65 years or older) from two randomized clinical trials concluded that adding bevacizumab to fluorouracil-based chemotherapy for first-line treatment of metastatic colorectal cancer improved overall survival and PFS in older patients as it does in younger patients, without increased risks of treatment in the older age group. Median overall survival improved from 14.3 months to 19.3 months with the addition of bevacizumab, while median PFS improved from 6.2 months to 9.2 months. [121]
Results from the randomized CAIRO3 trial appear to show that, compared with observation, maintenance therapy with capecitabine and bevacizumab significantly delayed disease progression in 558 previously untreated patients with stable (or better) metastatic colorectal cancer after six cycles of induction therapy with capecitabine, oxaliplatin, and bevacizumab (CAPOX-B). [122] Patients in both groups were treated with CAPOX-B at first progression until second progression.
At a median follow-up of 48 months, CAPOX-B was restarted in 48% of those in the maintenance treatment group and 61% of patients in the observation group. [122] Median second progression after randomization occurred at 11.7 months in the maintenance group and 8.5 months in the observation group, and median first progression after randomization occurred at 8.5 months in the maintenance group compared with 4.1 months in the observation group. The most pronounced benefit of maintenance therapy was in patients with RAS/BRAF wild-type and BRAF V600E–mutant tumors. [122]
In a study by Tebbutt et al, bevacizumab was found to be associated with a modestly increased risk of arterial thromboembolism (ATE). However, safety was not significantly worse in older patients or those with a history of ATE or other vascular risk factors. [123]
Despite its role in the therapy of metastatic colon cancer, bevacizumab did not significantly prolong disease-free survival in patients with stage II and III colon cancer, when added to adjuvant chemotherapy (mFOLFOX6) in a randomized trial (NASBP C-08). [124]
In 2017, the FDA approved Mvasi (bevacizumab-awwb) as a biosimilar to Avastin (bevacizumab), to be used in combination with fluoropyrimidine-irinotecan–based or fluoropyrimidine-oxaliplatin–based chemotherapy for the second-line treatment of patients with metastatic colorectal cancer that has progressed on a first-line bevacizumab-product–containing regimen. The approval was based on evidence from animal study data, human pharmacokinetic and pharmacodynamics data, and clinical immunogenicity data that supported Mvasi as a biosimilar to Avastin. [125]
Cetuximab
Cetuximab is a chimeric monoclonal antibody against EGFR that is approved for treatment of KRAS mutation–negative (wild-type), EGFR-expressing, metastatic colorectal cancer. Cetuximab can be used as first-line therapy, in combination with FOLFIRI (irinotecan, 5-fluorouracil, leucovorin). [126, 127] Additionally, cetuximab may be used as monotherapy or in combination with irinotecan (Camptosar) in patients with metastatic colorectal cancer refractory to fluoropyrimidine and oxaliplatin therapy. [128]
KRAS mutations, which are present in about 40% of colon adenocarcinomas, affect sensitivity to anti-EGFR treatment. [81] The addition of anti-EGFR antibody treatment to standard chemotherapy regimens for patients with advanced colorectal cancer improves PFS for those with wild-type KRAS status, but not those with mutant KRAS. [129]
The CRYSTAL trial, a large international trial exploring the benefit of adding cetuximab to first-line chemotherapy with FOLFIRI, documented that only patients with wild-type KRAS derived clinical benefit from cetuximab. In patients with mutant KRAS, adding cetuximab to chemotherapy provided no clinical benefit and resulted only in unnecessary toxicity. [127]
Based on these results, testing for KRAS mutation was added to the cetuximab indication by the European Medicines Agency (EMA). The FDA approved the use of cetuximab in combination with FOLFIRI for first-line treatment of patients with wild-type KRAS metastatic colorectal cancer, as determined by FDA-approved tests, in 2012.
Panitumumab
Panitumumab is a fully human monoclonal antibody against EGFR. This agent was originally approved as monotherapy for patients with EGFR-expressing metastatic colorectal cancer in whom combination chemotherapy with regimens containing fluoropyrimidine, oxaliplatin, and irinotecan had failed or was not tolerated.
In 2014, the FDA approved panitumumab for first-line treatment of patients with wild-type KRAS (exon 2) metastatic colorectal carcinoma in combination with fluorouracil, leucovorin, and oxaliplatin (FOLFOX4). [130] Approval was based on results from the PRIME trial. [131]
The PRIME trial, a phase III study, showed that patients with wild-type KRAS tumors achieved statistically significant improvement in PFS with panitumumab and FOLFOX4 versus FOLFOX4 alone (9.6 versus 8.0 months, P=0.02) and a nonsignificant improvement in OS versus FOLFOX4 alone (23.9 versus 19.7 months, P =0.07). In contrast, patients with mutant KRAS had significantly reduced PFS with panitumumab-FOLFOX4. [131]
Thus, panitumumab becomes an option, or an alternative to cetuximab, for patients who have tumors with wild-type KRAS. [132, 133] However, Hecht et al reported that adding panitumumab to bevacizumab and chemotherapy (oxaliplatin- and irinotecan-based) as first-line treatment of metastatic colorectal cancer resulted in increased toxicity and decreased PFS. [134]
Douillard and colleagues reported that in addition to KRAS mutations in exon 2, additional RAS mutations (KRAS exon 3 or 4; NRAS exon 2, 3, or 4; or BRAF exon 15) are associated with inferior PFS and OS with panitumumab-FOLFOX4 treatment. [135] Other mutations that involve some of the kinases downstream from KRAS (such as BRAF and PI3K) are being investigated and may result in even more selective methods to identify patients that may benefit from EGFR inhibition.
In 2017, the FDA extended approval for panitumumab for use in wild-type RAS (both KRAS and NRAS) metastatic colorectal cancer. Approval was based on a retrospective analysis from the PRIME trial and prospective, pre-defined analyses from the phase 3 '0007 study. The '0007 study evaluated the efficacy of panitumumab plus best supportive care (BSC) versus BSC alone in patients with chemorefractory, wild-type KRAS metastatic colorectal cancer. [136] Key secondary endpoint data showed significant improvement in overall survival (OS) of 10 months in BSC with panitumumab, versus 6.9 months with BSC alone.
In January 2025 the FDA extended approval for panitumumab for use in combination with sotorasib for the treatment of patients with KRAS G12 –mutated metastatic colorectal cancer (mCRC), as determined by an FDA-approved test, who have received prior fluoropyrimidine-, oxaliplatin- and irinotecan-based chemotherapy. Approval was based on results of phase 3 CodeBreaK 300 study, in which this combination showed superior PFS compared with investigator-chosen standard-of-care treatment. [137]
Ramucirumab
Ramucirumab is a recombinant human monoclonal antibody that binds the VEGF receptor. The FDA approved ramucirumab for use in combination with FOLFIRI for the treatment of patients with metastatic colorectal cancer that has progressed on a first-line bevacizumab-, oxaliplatin- and fluoropyrimidine-containing regimen. Approval was based on the phase III RAISE trial, in which the ramucirumab-FOLFIRI combination improved OS and PFS (13.3 months, 5.7 months, respecttively) compared with placebo-FOLFIRI (11.7 months, 4.5 months, respectively) (P = 0.023 and < 0.001, respectively). [138]
Nivolumab
Nivolumab is a monoclonal antibody to programmed cell death-1 protein (PD-1). In the CheckMate 142 phase II study, nivolumab, with or without ipilimumab, appeared tolerable and demonstrated clinical activity in patients with microsatellite instability–high (MSI-H) metastatic colorectal cancer. The study enrolled deficient mismatch repair (dMMR) and MSI-H colorectal cancer patients whose disease had progressed on, or who were intolerant to, at least one prior line of therapy. The investigator-assessed objective response rate (ORR) in patients receiving nivolumab (the primary endpoint) was 31%; the disease control rate was 69%. [139]
One year after entering the trial, 48.4% of patients were still alive and disease-free. One-year OS was 73.8%. Treatment was well tolerated, with no safety signals. [140]
CheckMate 142 brought an accelerated approval to nivolumab in 2017 for the treatment of patients 12 years or older with dMMR and MSI-H metastatic colorectal cancer that has progressed following treatment with a fluoropyrimidine, oxaliplatin, and irinotecan. In 2018, nivolumab in combination with low-dose ipilimumab also received accelerated approval for this indication. Continued approval of nivolumab for this indication may be contingent upon the outcomes of confirmatory trials. [141]
Pembrolizumab
Pembrolizumab, which is a monoclonal antibody to PD-1, is approved for treatment of unresectable or metastatic colon cancer that has tested positive for MSI-H or dMMR and has progressed after treatment with a fluoropyrimidine, oxaliplatin, and irinotecan. It is also approved for any solid tumor that has tested positive for MSI-H or dMMR in patients who have had prior treatment and have no satisfactory alternative treatment options. [142] The multicenter, randomized KEYNOTE-177 trial found that treatment with pembrolizumab monotherapy significantly reduced the risk of disease progression or death by 40% (HR, 0.60; 95% CI, 0.45 - 0.80; P = 0.0004), with a median PFS of 16.5 months versus 8.2 months for chemotherapy, in patients with dMMR colorectal cancers. [142]
Regorafenib
Regorafenib, a kinase inhibitor, is approved for patients with metastatic colorectal cancer who have been previously treated with fluoropyrimidine-, oxaliplatin-, and irinotecan-based chemotherapy; anti-VEGF therapy (eg, bevacizumab, ziv-aflibercept); and, if KRAS wild type, anti-EGFR therapy (eg, cetuximab, panitumumab). [143]
Approval was based on a multicenter trial in 760 patients with metastatic colon cancer in whom all approved standard therapies had failed. Patients were randomized in a 2:1 ratio to receive regorafenib or placebo; all patients also received best supportive care. Statistically significant benefit in OS and PFS was observed for regorafenib over placebo. [144]
Fruquintinib
Fruquintinib (Fruzaqla), a selective and potent oral inhibitor of vascular endothelial growth factor receptors (VEGFRs) 1, 2, and 3, was approved by the FDA in November 2023 for adults with metastatic colorectal cancer who received prior fluoropyrimidine-, oxaliplatin-, and irinotecan-based chemotherapy, an anti-VEGF therapy, and, if RAS wild-type and medically appropriate, an anti-EGFR therapy.
Approval was based on results of the FRESCO and FRESCO-2 trials. [145, 146] OS was the major efficacy outcome in both trials. In FRESCO-2, median OS was 7.4 months in the fruquintinib group versus 4.8 months in the placebo group (hazard ratio [HR] 0.66, P < 0.0001). [146] In FRESCO, median OS was 9.3 months and 6.6 months (HR 0.65, P < 0.001). [145]
Ziv-aflibercept
Ziv-aflibercept is a fusion protein that acts as a decoy receptor for VEGF-A, VEGF-B, and placental growth factor (PlGF). This agent was approved for use in combination with FOLFIRI for the treatment of patients with metastatic colorectal cancer that is resistant to or has progressed after an oxaliplatin-containing fluoropyrimidine-based regimen. [147]
Approval was based on the Aflibercept Versus Placebo in Metastatic Colorectal Cancer (mCRC) After Failure of an Oxaliplatin-Based Regimen (VELOUR) trial that included 1226 patients. Results showed improved OS and PFS when ziv-aflibercept was used in combination with fluorouracil, leucovorin, and irinotecan (FOLFIRI). [148]
A phase III trial by Van Cutsem and colleagues in patients with metastatic colorectal cancer previously treated with an oxaliplatin-based regimen found that the addition of ziv-aflibercept to FOLFIRI improves survival. Median survival time was 13.5 months with ziv-aflibercept plus FOLFIRI versus 12.06 months with FOLFIRI alone (P = 0.0032); PFS was 6.90 versus 4.67 months, respectively (P < 0.0001). [149]
Larotrectinib
Larotrectinib is a highly selective inhibitor of tropomyosin receptor kinases A, B, and C (TRKA, TRKB, TRKC), which are encoded by NTRK genes.In 2018, the FDA granted tissue-agnostic approval for larotrectinib for adult and pediatric patients who meet the following criteria [150] :
- Have solid tumors that harbor an NTRK gene fusion without a known acquired resistance mutation (note that NTRK fusions can be hard to detect and are found in only about 1% of colorectal cancers)
- Have metastatic disease or disease that has progressed after treatment
- Are likely to experience severe morbidity as a result of surgery
- Lack alternative satisfactory treatments
Therapy for BRAF V600E–positive disease
In December 2024 the FDA granted accelerated approval for the BRAF inhibitor encorafenib, in combination with cetuximab and mFOLFOX6, for first-line treatment of BRAF V600E mutation–positive metastatic colorectal cancer. Approval was based on results of the active-controlled, open-label BREAKWATER trial, in which the objective response rate with this regimen was 61%, as compared with 40% in the control arm, in which patients received mFOLFOX6, FOLFOXIRI, or CAPOX, each with or without bevacizumab. Median duration of response was 13.9 versus 11.1 months, respectively. [151]
For advanced or metastatic colon cancer that is BRAF V600E mutation positive, NCCN guidelines include the following as second-line therapy options [78] :
- Dabrafenib plus trametinib plus either cetuximab or panitumumab
- Encorafenib plus either cetuximab or panitumumab, with or without binimetinib
In the open-label, phase III BEACON trial, therapy with encorafenib and the EGFR inhibitor monoclonal antibody cetuximab, with or without the MEK inhibitor binimetinib (ie, triplet or doublet therapy) provided an overall survival benefit for patients with metastatic colorectal cancer who had the BRAF V600E mutation. The BEACON trial enrolled 665 patients with BRAF V600E–mutated metastatic colorectal cancer who had disease progression after one or two previous regimens. [152]
Updated analysis of BEACON showed that median overall survival was 9.3 months in the triplet- and doublet-therapy groups, compared with 5.9 months for patients in the control group, who received standard-of-care therapy with cetuximab plus irinotecan or cetuximab plus FOLFIRI. The confirmed objective response rate (ORR) was 26.8% for triplet therapy, 19.5% for doublet therapy, and 1.8% for control. Thus, the increased toxicity from the addition of binimetinib can be avoided, while maintaing good outcomes. [153]
HER2-positive disease
HER2 is overexpressed in approximately 3% of colorectal cancers overall and in 5-14% of _RAS/BRAF_–wild type colorectal tumors. Experimental therapeutic approaches for tumors that have HER2 overexpression have included trastuzumab plus lapatinib and trastuzumab plus pertuzumab. [110]
In a phase II proof-of-concept study, 27 heavily pretreated patients with HER2-positive metastatic colon cancer showed good response to a therapy regimen that is commonly used to treat HER2-positive breast cancer and does not include a chemotherapy backbone. The 27 patients in the study were identified through screening of 914 patients with KRAS exon 2 (codons 12 & 13) wild-type metastatic colorectal cancer. [154]
Most of the patients had extensive metastatic disease and distal colon tumors. Almost 75% had received at least four prior treatment regimens and had spent a median total time of 20 months on previous treatments.
Patients were treated with a combination of trastuzumab and lapatinib. At 1 year, 12 of the 27 patients (45%) were still alive. At a median follow-up of 94 weeks, one patient (4%) had achieved a complete response, seven (26%) had achieved a partial response, and disease had stabilized in 12 patients (44%). [154]
Another regimen, tucatinib in combination with trastuzumab, was granted accelerated approval by the FDA in 2023 for RAS wild-type HER2-positive unresectable or metastatic colorectal cancer that has progressed after treatment with fluoropyrimidine-, oxaliplatin-, and irinotecan-based chemotherapy. Approval was based on results from the open-label, multicenter MOUNTAINEER study in 84 patients, in which treatment with tucatinib in combination with trastuzumab yielded an overall response rate of 35% (3.6% complete response; 35% partial response), with a median duration of response of 12.4 months. [155]
Neoadjuvant Therapy
Guidelines from the American Society of Colon and Rectal Surgeons include the following recommendations on neoadjuvant therapy for colon cancer [96] :
- In patients with locally advanced colon cancer, neoadjuvant chemotherapy or radiotherapy can result in tumor regression and may facilitate margin-negative excision of locally advanced cancers.
- In patients with initially resectable colon cancer liver metastasis, an individualized decision should be made on neoadjuvant chemotherapy followed by surgical resection or up-front surgery.
- Patients with initially unresectable colon cancer liver metastasis should be considered for neoadjuvant chemotherapy to attempt to convert to resectability.
- Hepatic artery infusion of chemotherapy combined with systemic chemotherapy or immunotherapy may increase resectability of colon cancer liver metastasis, but should be performed only in centers with the appropriate expertise.
![]()
Radiation Therapy
Although radiation therapy remains a standard modality for patients with rectal cancer, it has only a limited role in colon cancer. Radiation therapy is not used in the adjuvant setting, and in metastatic settings it is used only for palliative care in selected sites such as bone or brain metastases.
Newer, more selective ways of administering radiation therapy, such as stereotactic radiotherapy (CyberKnife) and tomotherapy, are currently being investigated. In the future, these techniques may extend the indications for radiotherapy in the management of colon cancer.
A prospective, multicenter, randomized phase III study by Hendlisz et al showed that the addition of radioembolization with yttrium-90 significantly improved time to liver progression and median time to tumor progression in patients with unresectable, chemotherapy-refractory, liver-limited metastatic colorectal cancer. The study compared treatment with fluorouracil alone with fluorouracil plus yttrium-90 resin, which was injected into the hepatic artery. [156] The US Food and Drug Administration (FDA) has approved yttrium-90 resin microspheres (SIR-Spheres) for the treatment of unresectable metastatic liver tumors from primary colorectal cancer in combination with adjuvant intra–hepatic artery chemotherapy with floxuridine.
![]()
Diet
In a prospective cohort study that included 1575 healthcare professionals with stage I to III colorectal cancer, Song et al found that rates of colorectal cancer (CRC)–specific mortality and overall mortality were lower in patients who had higher intake of dietary fiber, especially from cereals. Survival rates were higher in patients who increased their fiber intake after diagnosis from levels before diagnosis, and in patients reporting higher intake of whole grains. [157]
After multivariable adjustment, each 5 g increment in daily fiber intake was associated with a 22% decrease in CRC-specific mortality and a 14% decrease in all-cause mortality. In patients who increased their fiber intake after diagnosis, each 5 g increase in daily fiber intake was associated with 18% lower CRC-specific mortality. The relationship between fiber intake after diagnosis and CRC-specific mortality reached a maximum at approximately 24 g/d, beyond which no further mortality reduction was found. [157]
Evaluation of the source of fiber showed that cereal fiber was associated with lower CRC-specific mortality (33% per 5-g/d increment) and all-cause mortality (22%); vegetable fiber was associated with 17% lower all-cause mortality but not with significantly lower CRC-specific; no association was found for fruit fiber. Whole grain intake was associated with lower CRC-specific mortality (28% decrease in risk per 20-g/day increment), although this beneficial association fell to 23% after adjusting for fiber intake. [157]
A prospective cohort study in 1011 patients with stage III colon cancer found that postdiagnosis intake of unprocessed red meat or processed meat was not associated with risk of recurrence or death. Van Blarigan et al reported that multivariable hazard ratios comparing the highest versus the lowest quartiles for cancer recurrence or death were 0.84 (95% CI, 0.58-1.23) for unprocessed red meat and 1.05 (95% CI, 0.75-1.47) for processed meat. [158]
![]()
Consultations
Colorectal cancer, especially early stage disease, can be cured surgically. Following diagnosis and staging, obtaining surgical consultation for the possibility of resection may be appropriate. After surgery, the stage of the tumor may be advanced depending on the operative findings (eg, lymph node involvement, palpable liver masses, peritoneal spread).
In the care of patients with colorectal cancer and isolated liver metastases, consider surgical consultation for possible resection. In some cases, resection of previously unresectable liver metastases may become feasible after cytoreduction with neoadjuvant chemotherapy. Therefore, ongoing involvement of the surgical oncologist is very important in patient care, even if the tumor is not considered resectable at the time of diagnosis. In patients with advanced disease, palliative surgery may be helpful in cases of bleeding or obstruction.
Gastroenterology (GI) consultation is critical for screening of high-risk individuals (ie, patients with a family history of colorectal cancer or polyposis syndromes) and those individuals who are found to be inappropriately iron deficient or to have occult blood on screening fecal examination. A colonoscopy or sigmoidoscopy is necessary to visualize the colon endoscopically, to obtain biopsies, or to resect polyps.
GI consultation may also be necessary in the management of advanced disease. The advent of colorectal stents allows a nonsurgical management of impending obstruction in patients who present with unresectable, metastatic disease.
GI consultation is necessary in the follow-up of patients after surgical resection and adjuvant chemotherapy. Patients must be screened for recurrent disease in the colon by colonoscopic examination at 1 year after surgery and then every 3 years.
![]()
Long-Term Monitoring
Pooled analysis from several large adjuvant trials showed that 85% of colon cancer recurrences occur within 3 years after resection of primary tumor, with 95% occurring within 5 years. Therefore, patients with resected colon cancer (stage II and III) should undergo regular surveillance for at least 5 years following resection. [159] Recommendations for post-treatment surveillance, from the European Society for Medical Oncology (ESMO), [160] the American Society for Clinical Oncology (ASCO), [159] and the National Comprehensive Cancer Network (NCCN) [78] are compared in Table 2, below.
Table 2. Surveillance recommendations for stage II and III colon cancer (Open Table in a new window)
| Parameter | Organization | ||
|---|---|---|---|
| ESMO [JSMO](2013) | ASCO (2013) | NCCN (2024) | |
| History and physical exam | Every 3-6 mo for 3 y, then every 6 -12 mo at 4 and 5 y | Every 3-6 mo for 3 y, then every 6 mo to 5 y | Every 3-6 mo for 2 y, then every 6 mo to 5 y |
| CEA | Every 3-6 mo for 3 y, then every 6 -12 mo at 4 and 5 y | Every 3 mo for 3 y* | Every 3-6 mo for 2 y, then every 6 mo to 5 y |
| Chest CT* | Every 6-12 mo for first 3 y | Every 1 y for 3 y | Every 6-12 mo for 5 y |
| Colonoscopy** | At y 1 after surgery, and every 3-5 y thereafter | At 1 y, then every 5 y, dictated by the findings on the previous colonoscopy | At 1 y, 3 y, then every 5 y if negative |
| Abdominal CT* | Every 6-12 mo for first 3 y | Every 1 y for 3 y | Every 6-12 mo for up to 5 y; scans to include chest and pelvis |
| ESMO = European Society of Medical Oncology; JSMO = Japanese Society of Medical Oncology; ASCO = American Society of Clinical Oncology; NCCN = National Comprehensive Cancer Network; CEA = carcinoembryonic antigen; CT = computed tomography* For patients at high risk for recurrence (eg, lymphatic or venous invasion, or poorly differentiated tumors).**Colonoscopy should be performed 3-6 mo postoperatively if preoperative colonoscopy was not done, due to an obstructing lesion; otherwise, colonoscopy in 1 y; if abnormal, repeat in 1 year; if no advanced adenoma (ie, villous polyp, polyp > 1 cm, or high-grade dysplasia), repeat in 3 y, then every 5 y. |
Followup should be guided by the patient’s presumed risk of recurrence and functional status. Testing at the more frequent end of the range should be considered for patients at high risk. Patients with severe comorbid conditions that make them ineligible for surgery or systemic therapy should not undergo surveillance testing. [159]
In 2016, the US Multi-Society Task Force on Colorectal Cancer issued guidelines on colonoscopy after colorectal cancer resection, which included the following recommendations [161] :
- Patients with colorectal cancer (CRC) should undergo high-quality perioperative clearing with colonoscopy. The procedure should be performed preoperatively, or within a 3- to 6-mo interval after surgery in the case of obstructive CRC. The goals of perioperative clearing colonoscopy are detection of synchronous cancer and detection and complete resection of precancerous polyps.
- Patients who have undergone curative resection of either colon or rectal cancer should receive their first surveillance colonoscopy 1 yr after surgery (or 1 yr after the clearing perioperative colonoscopy).
- Patients with localized rectal cancer who have undergone surgery without total mesorectal excision, those who have undergone transanal local excision (ie, transanal excision or transanal endoscopic microsurgery) or endoscopic submucosal dissection, and those with locally advanced rectal cancer who did not receive neoadjuvant chemoradiation and then surgery using total mesorectal excision techniques, are at increased risk for local recurrence. In these situations, it is suggested that patients undergo local surveillance with flexible sigmoidoscopy or endoscopic ultrasound (EUS) every 3−6 mo for the first 2−3 yr after surgery. These surveillance measures are in addition to recommended colonoscopic surveillance for metachronous neoplasia.
- In patients with obstructive CRC precluding complete colonoscopy, CT colonography (CTC) is recommended as the best alternative to exclude synchronous neoplasms. Double-contrast barium enema is an acceptable alternative if CTC is not available.
Cancer Care Ontario published guidelines for the follow-up care of survivors of stages II and III colorectal cancer, and these were endorsed by the American Society of Clinical Oncology. The recommendations include the following [159] :
- Surveillance is especially important in the initial 2-4 years following treatment, when most recurrences occur
- Patients should be followed for 5 years, and regular reviews of medical history, physical examination, and carcinoembryonic antigen testing should be performed every 3-6 months
- Annual computed tomography (CT) scanning of the abdomen and chest should be performed for 3 years
- Pelvic CT scanning should be performed in patients with rectal cancer annually for 3-5 years
- In patients who have not received pelvic radiation, a rectosigmoidoscopy should be performed every 6 months for 2-5 years
- A surveillance colonoscopy should be performed approximately 1 year after initial surgery
- Patients should be counseled to maintain a healthy body weight, be physically active, and follow a healthy diet
![]()
Prevention
Colorectal cancer prevention strategies fall into three categories:
- Lifestyle measures
- Pharmacologic prevention
Lifestyle measures
Abundant epidemiologic literature suggests an association of risk for developing colorectal cancer with dietary habits, environmental exposures, and level of physical activity. For example, a prospective cohort study in the general population of two Danish cities concluded that 23% of colorectal cancer cases might have been prevented if all participants had followed recommendations for the following five lifestyle factors [162] :
- Physical activity
- Waist circumference
- Smoking
- Alcohol intake
- Diet
A study of 79,952 men and 93,475 women who participated in the Multiethnic Cohort Study found that greater adherence to plant-based diets rich in healthy plant foods and low in less-healthy plant foods is associated with a reduced risk of colorectal cancer in men, but not in women. Plant foods designated as healthy were whole grains, fruits, vegetables, vegetable oils, nuts, legumes, and tea and coffee; those designated as less healthy were refined grains, fruit juices, potatoes, and added sugars. Benefits of a plant-based diet were greater in Japanese American, Native Hawaiian, and White groups than in African-American or Latino groups and for left colon and rectal tumors than right tumors. [163]
There is also evidence that diet and physical activity affect the risk for recurrence of colon cancer. A prospective observational study involving patients with stage III colon cancer from the CALGB 89803 adjuvant chemotherapy trial demonstrated adverse effect with regards to risk for recurrence and increased mortality for patients following a "Western" diet (high intake of red meat, refined grains, fat, and sweets) versus a "prudent" diet (high intake of fruits and vegetables, poultry, and fish). [15]
In another observational study from the same cohort of patients, patients were prospectively monitored and physical activity was recorded. The study concluded that physical activity reduces the risk of recurrence and mortality in patients with resected stage III colon cancer. [164]
Calcium and vitamin D supplementation
Although earlier data had strongly indicated that calcium supplementation can help prevent colorectal cancer, and had suggested a preventive effect of vitamin D supplementation, a randomized trial by Baron et al found that daily supplementation with vitamin D3 (1000 IU), calcium (1200 mg), or both after removal of colorectal adenomas did not significantly reduce the risk of recurrent colorectal adenomas over a period of 3 to 5 years. [165]
However, a randomized trial by Barry et al suggested that vitamin D receptor genotype may affect the benefits of vitamin D3 supplementation. In their analysis of 41 single-nucleotide polymorphisms (SNPs) in vitamin D and calcium pathway genes in 1702 patients with colorectal adenomas, vitamin D3 supplementation decreased risk for advanced adenomas (but not adenomas overall) by 64% in study subjects with the AA genotype at the rs7968585 SNP, but increased risk by 41% in those with one or two G alleles. The benefits of calcium supplementation were not significantly linked to genotype. [166]
Circulating levels of 25 hydroxyvitamin D (25[OH]D) that are optimal for preventing colorectal cancer may be significantly higher than levels necessary for bone health, according to an international collaborative meta-analysis that pooled 17 cohorts. Although levels of 50 to < 62.5 nmol/L are considered adequate for bone health by the Institute of Medicine, the study found that levels of 75–< 87.5 were associated with 19% lower risk and levels of 87.5–< 100 nmol/L were associated with 27% lower risk. [167]
For each 25 nmol/L increment in circulating 25(OH)D, colorectal cancer risk was 19% lower in women and 7% lower in men. In addition, the study confirmed that vitamin D deficiency increases colorectal cancer risk: 25(OH)D levels of less than 30 nmol/L were associated with a 31% greater risk compared with adequate levels. [167]
Pharmacologic prevention
Pharmacologic prevention is based on the understanding of colorectal carcinogenesis and the availability of pharmacologic agents that are effective yet minimally toxic. The efficacy of these agents is usually first tested in high-risk populations.
Celecoxib (Celebrex), a selective cyclooxygenase-2 inhibitor, was first tested in patients with familial adenomatous polyposis (FAP). Celecoxib was effective in decreasing the number and size of polyps on serial colonoscopies, which was the primary surrogate endpoint for this trial. [168] The drug was approved for FAP patients, although it remains to be seen whether this intervention translates to reduced cancer incidence and prolonged survival.
Enthusiasm for cyclooxygenase-2 inhibitors as chemopreventive agents has dampened because of a high incidence of cardiovascular toxicity in trial patients, which led to the removal of rofecoxib from the market. Other nonsteroidal anti-inflammatory drugs (NSAIDs), such as sulindac and nonselective cyclooxygenase inhibitors, have been tested in lower-risk populations.
Aspirin use has been shown to be effective in both primary prevention of colorectal cancer (at doses of 300 mg or more daily for about 5 years [169] ) and secondary prevention (at doses ranging from 81 to 325 mg daily [170] ) of colorectal adenomas. The decrease in colon cancer risk with aspirin use may vary among population subgroups. However, body mass index, physical activity, and plasma C-peptide levels were shown to not have a significant impact on aspirin’s effect on colon cancer risk. [171]
Examination of questionnaire data collected from the Nurses’ Health Study and the Health Professionals Follow-up Study showed regular aspirin use was associated with lower risk of BRAF –wild-type colorectal cancer (multivariable hazard ratio [HR], 0.73) but not with BRAF -mutated cancer risk (multivariable HR, 1.03). Status of tumor PTGS2 expression or PIK3CA or KRAS mutation had no effect on this association. [172]
A 2013 study showed that low-dose aspirin taken every other day lowers the risk for colorectal cancer in middle-aged women. Nearly 40,000 women aged 45 and older were randomized to low-dose aspirin (100 mg) or placebo every other day for roughly 10 years; 84% were followed for an additional 7 years after treatment ended. At followup, colorectal cancer risk was lower in the aspirin group, mostly owing to a reduction in proximal colon cancer; this reduction in risk emerged after 10 years. [173]
American College of Gastroenterology (ACG) guidelines suggest the use of low-dose aspirin to reduce risk of colorectal cancer in individuals aged 50–69 years with a cardiovascular disease risk of 10% or higher over the next 10 years, who are not an increased risk for bleeding and are willing to take aspirin for at least 10 years. The ACG recommends against the use of aspirin as a substitute for colorectal cancer screening. [54]
Some trials focused on combined inhibition of polyamine production and cyclooxygenase inhibition. A report from a large randomized trial of a combination of sulindac and dimethylformamine (DMFO), an inhibitor of ornithine decarboxylase (ODC), described a dramatic effect of this combination in reducing polyp recurrence in patients with prior history of colon polyps. Confirmatory trials are ongoing. [174]
![]()
- PDQ Adult Treatment Editorial Board. Colon Cancer Treatment–Health Professional Version. National Cancer Institute. Available at https://www.cancer.gov/types/colorectal/hp/colon-treatment-pdq. September 26, 2024; Accessed: January 16, 2025.
- Goldberg RM, Sargent DJ, Morton RF, et al. A randomized controlled trial of fluorouracil plus leucovorin, irinotecan, and oxaliplatin combinations in patients with previously untreated metastatic colorectal cancer. J Clin Oncol. 2004 Jan 1. 22(1):23-30. [QxMD MEDLINE Link].
- Haller DG, Catalano PJ, Macdonald JS, O'Rourke MA, Frontiera MS, Jackson DV. Phase III study of fluorouracil, leucovorin, and levamisole in high-risk stage II and III colon cancer: final report of Intergroup 0089. J Clin Oncol. 2005 Dec 1. 23(34):8671-8. [QxMD MEDLINE Link].
- Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med. 2004 Jun 3. 350(23):2335-42. [QxMD MEDLINE Link].
- Sanoff HK, Sargent DJ, Campbell ME, et al. Five-year data and prognostic factor analysis of oxaliplatin and irinotecan combinations for advanced colorectal cancer: N9741. J Clin Oncol. 2008 Dec 10. 26(35):5721-7. [QxMD MEDLINE Link].
- Nguyen LH, Goel A, Chung DC. Pathways of Colorectal Carcinogenesis. Gastroenterology. 2020 Jan. 158 (2):291-302. [QxMD MEDLINE Link]. [Full Text].
- Järvinen HJ, Aarnio M, Mustonen H, Aktan-Collan K, Aaltonen LA, Peltomäki P, et al. Controlled 15-year trial on screening for colorectal cancer in families with hereditary nonpolyposis colorectal cancer. Gastroenterology. 2000 May. 118 (5):829-34. [QxMD MEDLINE Link].
- Rex DK, Ahnen DJ, Baron JA, Batts KP, Burke CA, Burt RW, et al. Serrated lesions of the colorectum: review and recommendations from an expert panel. Am J Gastroenterol. 2012 Sep. 107 (9):1315-29; quiz 1314, 1330. [QxMD MEDLINE Link].
- Chang WH, Cerione RA, Antonyak MA. Extracellular Vesicles and Their Roles in Cancer Progression. Methods Mol Biol. 2021. 2174:143-170. [QxMD MEDLINE Link]. [Full Text].
- Zhao X, Yuan C, Wangmo D, Subramanian S. Tumor secreted extracellular vesicles regulate T-cell costimulation and can be manipulated to induce tumor specific T-cell responses. Gastroenterology. 2021 Apr 22. [QxMD MEDLINE Link].
- Burn J, Bishop DT, Mecklin JP, Macrae F, et al. Effect of aspirin or resistant starch on colorectal neoplasia in the Lynch syndrome. N Engl J Med. 2008 Dec 11. 359(24):2567-78. [QxMD MEDLINE Link].
- Yan HHN, Lai JCW, Ho SL, Leung WK, Law WL, Lee JFY, et al. RNF43 germline and somatic mutation in serrated neoplasia pathway and its association with BRAF mutation. Gut. 2017 Sep. 66 (9):1645-1656. [QxMD MEDLINE Link].
- Carballal S, Balaguer F, IJspeert JEG. Serrated polyposis syndrome; epidemiology and management. Best Pract Res Clin Gastroenterol. 2022 Jun-Aug. 58-59:101791. [QxMD MEDLINE Link].
- Dekker E, Bleijenberg A, Balaguer F, Dutch-Spanish-British Serrated Polyposis Syndrome collaboration. Update on the World Health Organization Criteria for Diagnosis of Serrated Polyposis Syndrome. Gastroenterology. 2020 May. 158 (6):1520-1523. [QxMD MEDLINE Link]. [Full Text].
- Meyerhardt JA, Niedzwiecki D, Hollis D, et al. Association of dietary patterns with cancer recurrence and survival in patients with stage III colon cancer. JAMA. 2007 Aug 15. 298(7):754-64. [QxMD MEDLINE Link].
- Aune D, Chan DS, Lau R, et al. Dietary fibre, whole grains, and risk of colorectal cancer: systematic review and dose-response meta-analysis of prospective studies. BMJ. 2011 Nov 10. 343:d6617. [QxMD MEDLINE Link]. [Full Text].
- Pala V, Sieri S, Berrino F, et al. Yogurt consumption and risk of colorectal cancer in the Italian European prospective investigation into cancer and nutrition cohort. Int J Cancer. 2011 Dec 1. 129(11):2712-9. [QxMD MEDLINE Link].
- Tabung FK, Liu L, Wang W, Fung TT, Wu K, Smith-Warner SA, et al. Association of Dietary Inflammatory Potential With Colorectal Cancer Risk in Men and Women. JAMA Oncol. 2018 Jan 18. [QxMD MEDLINE Link].
- Monteiro CA, Cannon G, Levy RB, Moubarac JC, Louzada ML, Rauber F, et al. Ultra-processed foods: what they are and how to identify them. Public Health Nutr. 2019 Apr. 22 (5):936-941. [QxMD MEDLINE Link]. [Full Text].
- Meine GC, Picon RV, Espírito Santo PA, Sander GB. Ultra-Processed Food Consumption and Gastrointestinal Cancer Risk: A Systematic Review and Meta-Analysis. Am J Gastroenterol. 2024 Jun 1. 119 (6):1056-1065. [QxMD MEDLINE Link].
- Goncalves MD, Lu C, Tutnauer J, Hartman TE, Hwang SK, Murphy CJ, et al. High-fructose corn syrup enhances intestinal tumor growth in mice. Science. 2019 Mar 22. 363 (6433):1345-1349. [QxMD MEDLINE Link].
- Tsoi KK, Pau CY, Wu WK, Chan FK, Griffiths S, Sung JJ. Cigarette smoking and the risk of colorectal cancer: a meta-analysis of prospective cohort studies. Clin Gastroenterol Hepatol. 2009 Jun. 7(6):682-688.e1-5. [QxMD MEDLINE Link].
- Cho E, Lee JE, Rimm EB, Fuchs CS, Giovannucci EL. Alcohol consumption and the risk of colon cancer by family history of colorectal cancer. Am J Clin Nutr. 2012 Feb. 95(2):413-9. [QxMD MEDLINE Link]. [Full Text].
- Yuhara H, Steinmaus C, Cohen SE, Corley DA, Tei Y, Buffler PA. Is diabetes mellitus an independent risk factor for colon cancer and rectal cancer?. Am J Gastroenterol. 2011 Nov. 106(11):1911-21; quiz 1922. [QxMD MEDLINE Link].
- Jacobs ET, Ahnen DJ, Ashbeck EL, Baron JA, Greenberg ER, Lance P, et al. Association between body mass index and colorectal neoplasia at follow-up colonoscopy: a pooling study. Am J Epidemiol. 2009 Mar 15. 169(6):657-66. [QxMD MEDLINE Link].
- Bailly L, Fabre R, Pradier C, Iannelli A. Colorectal Cancer Risk Following Bariatric Surgery in a Nationwide Study of French Individuals With Obesity. JAMA Surg. 2020 Mar 11. [QxMD MEDLINE Link].
- Morikawa T, Kuchiba A, Lochhead P, et al. Prospective Analysis of Body Mass Index, Physical Activity, and Colorectal Cancer Risk Associated with ß-Catenin (CTNNB1) Status. Cancer Res. 2013 Mar 1. 73(5):1600-10. [QxMD MEDLINE Link]. [Full Text].
- Zhou E, Wang L, Santiago CN, Nanavati J, Rifkin S, Spence E, et al. Adult-Attained Height and Colorectal Cancer Risk: A Cohort Study, Systematic Review and Meta-Analysis. Cancer Epidemiol Biomarkers Prev. 2022 Mar 1. [QxMD MEDLINE Link]. [Full Text].
- Zhang J, Haines C, Watson AJM, Hart AR, Platt MJ, Pardoll DM, et al. Oral antibiotic use and risk of colorectal cancer in the United Kingdom, 1989-2012: a matched case-control study. Gut. 2019 Aug 19. [QxMD MEDLINE Link].
- Surveillance, Epidemiology, and End Results Program. Cancer Stat Facts: Colorectal Cancer. National Cancer Institute. Available at https://seer.cancer.gov/statfacts/html/colorect.html. Accessed: January 16, 2025.
- Cancer Facts & Figures 2025. American Cancer Society. Available at https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2025/2025-cancer-facts-and-figures-acs.pdf. Accessed: January 16, 2025.
- Siegel RL, Fedewa SA, Anderson WF, Miller KD, Ma J, Rosenberg PS, et al. Colorectal Cancer Incidence Patterns in the United States, 1974-2013. J Natl Cancer Inst. 2017 Aug 1. 109 (8):[QxMD MEDLINE Link]. [Full Text].
- Ferlay J, Ervik M, Lam F, Laversanne M, Colombet M, Mery L, et al. Colon. Global Cancer Observatory. Available at https://gco.iarc.who.int/media/globocan/factsheets/cancers/8-colon-fact-sheet.pdf. Accessed: January 17, 2025.
- Malvezzi M, Carioli G, Bertuccio P, Boffetta P, Levi F, La Vecchia C, et al. European cancer mortality predictions for the year 2018 with focus on colorectal cancer. Ann Oncol. 2018 Mar 19. [QxMD MEDLINE Link]. [Full Text].
- Sung H, Siegel RL, Laversanne M, Jiang C, Morgan E, Zahwe M, et al. Colorectal cancer incidence trends in younger versus older adults: an analysis of population-based cancer registry data. Lancet Oncol. 2025 Jan. 26 (1):51-63. [QxMD MEDLINE Link]. [Full Text].
- Giaquinto AN, Miller KD, Tossas KY, Winn RA, Jemal A, Siegel RL. Cancer statistics for African American/Black People 2022. CA Cancer J Clin. 2022 May. 72 (3):202-229. [QxMD MEDLINE Link]. [Full Text].
- Siegel RL, Miller KD, Goding Sauer A, Fedewa SA, Butterly LF, Anderson JC, et al. Colorectal cancer statistics, 2020. CA Cancer J Clin. 2020 Mar 5. [QxMD MEDLINE Link]. [Full Text].
- Meester RGS, Mannalithara A, Lansdorp-Vogelaar I, Ladabaum U. Trends in Incidence and Stage at Diagnosis of Colorectal Cancer in Adults Aged 40 Through 49 Years, 1975-2015. JAMA. 2019 May 21. 321 (19):1933-1934. [QxMD MEDLINE Link].
- Chua TC, Saxena A, Chu F, Zhao J, Morris DL. Predictors of cure after hepatic resection of colorectal liver metastases: an analysis of actual 5- and 10-year survivors. J Surg Oncol. 2011 Jun. 103(8):796-800. [QxMD MEDLINE Link].
- Fong Y, Fortner J, Sun RL, Brennan MF, Blumgart LH. Clinical score for predicting recurrence after hepatic resection for metastatic colorectal cancer: analysis of 1001 consecutive cases. Ann Surg. 1999 Sep. 230(3):309-18; discussion 318-21. [QxMD MEDLINE Link].
- Aggarwal C, Meropol NJ, Punt CJ, Iannotti N, Saidman BH, Sabbath KD, et al. Relationship among circulating tumor cells, CEA and overall survival in patients with metastatic colorectal cancer. Ann Oncol. 2012 Oct 1. [QxMD MEDLINE Link].
- Katz SC, Bamboat ZM, Maker AV, Shia J, Pillarisetty VG, Yopp AC, et al. Regulatory T Cell Infiltration Predicts Outcome Following Resection of Colorectal Cancer Liver Metastases. Ann Surg Oncol. 2012 Sep 26. [QxMD MEDLINE Link].
- Yothers G, Sargent DJ, Wolmark N, et al. Outcomes Among Black Patients With Stage II and III Colon Cancer Receiving Chemotherapy: An Analysis of ACCENT Adjuvant Trials. J Natl Cancer Inst. 2011 Oct 19. 103(20):1498-1506. [QxMD MEDLINE Link]. [Full Text].
- Campbell PT, Newton CC, Dehal AN, et al. Impact of body mass index on survival after colorectal cancer diagnosis: the Cancer Prevention Study-II Nutrition Cohort. J Clin Oncol. 2012 Jan 1. 30(1):42-52. [QxMD MEDLINE Link].
- Campbell PT, Patel AV, Newton CC, Jacobs EJ, Gapstur SM. Associations of recreational physical activity and leisure time spent sitting with colorectal cancer survival. J Clin Oncol. 2013 Mar 1. 31(7):876-85. [QxMD MEDLINE Link].
- Morikawa T, Kuchiba A, Yamauchi M, et al. Association of CTNNB1 (beta-catenin) alterations, body mass index, and physical activity with survival in patients with colorectal cancer. JAMA. 2011 Apr 27. 305(16):1685-94. [QxMD MEDLINE Link]. [Full Text].
- Rothwell PM, Fowkes GR, Belch JF, Ogawa H, Warlow CP, Meade TW. Effect of daily aspirin on long-term risk of death due to cancer: analysis of individual patient data from randomized trials. Lancet. Dec 7/2010; Early online publication. [Full Text].
- Burn J, Gerdes AM, Macrae F, et al. Long-term effect of aspirin on cancer risk in carriers of hereditary colorectal cancer: an analysis from the CAPP2 randomised controlled trial. Lancet. 2011 Dec 17. 378(9809):2081-7. [QxMD MEDLINE Link]. [Full Text].
- Baillargeon J, Kuo YF, Lin YL, et al. Effect of mental disorders on diagnosis, treatment, and survival of older adults with colon cancer. J Am Geriatr Soc. 2011 Jul. 59(7):1268-73. [QxMD MEDLINE Link].
- Phipps AI, Baron J, Newcomb PA. Prediagnostic smoking history, alcohol consumption, and colorectal cancer survival: The Seattle Colon Cancer Family Registry. Cancer. 2011 Nov 1. 117(21):4948-57. [QxMD MEDLINE Link]. [Full Text].
- Dehal AN, Newton CC, Jacobs EJ, et al. Impact of diabetes mellitus and insulin use on survival after colorectal cancer diagnosis: the Cancer Prevention Study-II Nutrition Cohort. J Clin Oncol. 2012 Jan 1. 30(1):53-9. [QxMD MEDLINE Link].
- Arhi CS, Ziprin P, Bottle A, Burns EM, Aylin P, Darzi A. Colorectal cancer patients under the age of 50 experience delays in primary care leading to emergency diagnoses: a population-based study. Colorectal Dis. 2019 Aug 6. [QxMD MEDLINE Link]. [Full Text].
- Fritz CDL, Otegbeye EE, Zong X, Demb J, Nickel KB, Olsen MA, et al. Red-flag Signs and Symptoms for Earlier Diagnosis of Early-Onset Colorectal Cancer. J Natl Cancer Inst. 2023 May 4. [QxMD MEDLINE Link].
- [Guideline] Shaukat A, Kahi CJ, Burke CA, Rabeneck L, Sauer BG, Rex DK. ACG Clinical Guidelines: Colorectal Cancer Screening 2021. Am J Gastroenterol. 2021 Mar 1. 116 (3):458-479. [QxMD MEDLINE Link]. [Full Text].
- Umar A, Boland CR, Terdiman JP, Syngal S, de la Chapelle A, Rüschoff J, et al. Revised Bethesda Guidelines for hereditary nonpolyposis colorectal cancer (Lynch syndrome) and microsatellite instability. J Natl Cancer Inst. 2004 Feb 18. 96(4):261-8. [QxMD MEDLINE Link]. [Full Text].
- Thirunavukarasu P, Sukumar S, Sathaiah M, Mahan M, Pragatheeshwar KD, Pingpank JF, et al. C-stage in Colon Cancer: Implications of Carcinoembryonic Antigen Biomarker in Staging, Prognosis, and Management. J Natl Cancer Inst. 2011 Apr 20. 103(8):689-97. [QxMD MEDLINE Link].
- Littlejohn C, Hilton S, Macfarlane GJ, Phull P. Systematic review and meta-analysis of the evidence for flexible sigmoidoscopy as a screening method for the prevention of colorectal cancer. Br J Surg. 2012 Sep 21. [QxMD MEDLINE Link].
- Holme O, et al for the NORCCAP Study Group. Long-Term Effectiveness of Sigmoidoscopy Screening on Colorectal Cancer Incidence and Mortality in Women and Men: A Randomized Trial. Ann Intern Med. 24 April 2018. [Full Text].
- Kahi CJ, Pohl H, Myers LJ, Mobarek D, Robertson DJ, Imperiale TF. Colonoscopy and Colorectal Cancer Mortality in the Veterans Affairs Health Care System: A Case-Control Study. Ann Intern Med. 2018 Mar 13. [QxMD MEDLINE Link].
- Wilschut JA, Habbema JD, van Leerdam ME, et al. Fecal occult blood testing when colonoscopy capacity is limited. J Natl Cancer Inst. 2011 Dec 7. 103(23):1741-51. [QxMD MEDLINE Link].
- Jensen CD, Corley DA, Quinn VP, Doubeni CA, Zauber AG, Lee JK, et al. Fecal Immunochemical Test Program Performance Over 4 Rounds of Annual Screening: A Retrospective Cohort Study. Ann Intern Med. 2016 Jan 26. [QxMD MEDLINE Link]. [Full Text].
- Corley DA, Jensen CD, Quinn VP, Doubeni CA, Zauber AG, Lee JK, et al. Association Between Time to Colonoscopy After a Positive Fecal Test Result and Risk of Colorectal Cancer and Cancer Stage at Diagnosis. JAMA. 2017 Apr 25. 317 (16):1631-1641. [QxMD MEDLINE Link].
- Gandhi S, Narula N, Mosleh W, Marshall JK, Farkouh M. Meta-analysis: colonoscopic post-polypectomy bleeding in patients on continued clopidogrel therapy. Aliment Pharmacol Ther. 2013 May. 37(10):947-52. [QxMD MEDLINE Link].
- Nelson R. FDA Approves Cologuard for Colorectal Cancer Screening. Medscape Medical News. Available at https://www.medscape.com/viewarticle/829757. August 11, 2014; Accessed: January 17, 2025.
- Brooks M. FDA Clears First Blood-Based Colorectal Cancer Screening Test. Medscape Medical News. Available at https://www.medscape.com/viewarticle/861942. April 14, 2016; Accessed: January 17, 2025.
- Given Imaging Receives FDA Clearance for PillCam® COLON in Patients Following Incomplete Colonoscopy. Med Device Online. Available at https://www.meddeviceonline.com/doc/given-imaging-fda-pillcam-colon-incomplete-colonoscopy-0001. February 3, 2014; Accessed: January 17, 2025.
- Spada C, De Vincentis F, Cesaro P, Hassan C, Riccioni ME, Minelli Grazioli L, et al. Accuracy and safety of second-generation PillCam COLON capsule for colorectal polyp detection. Therap Adv Gastroenterol. 2012 May. 5(3):173-8. [QxMD MEDLINE Link]. [Full Text].
- American Cancer Society Guideline for Colorectal Cancer Screening. American Cancer Society. Available at https://www.cancer.org/cancer/types/colon-rectal-cancer/detection-diagnosis-staging/acs-recommendations.html. January 29, 2024; Accessed: January 17, 2025.
- [Guideline] US Preventive Services Task Force., Davidson KW, Barry MJ, Mangione CM, Cabana M, Caughey AB, et al. Screening for Colorectal Cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2021 May 18. 325 (19):1965-1977. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High Risk Assessment: Colorectal, Endometrial, and Gastric. NCCN. Available at https://www.nccn.org/professionals/physician_gls/pdf/genetics_colon.pdf. Version 3.2024 — October 31, 2024; Accessed: December 31, 2024.
- [Guideline] Levin B, Lieberman DA, McFarland B, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. CA Cancer J Clin. 2008 May-Jun. 58(3):130-60. [QxMD MEDLINE Link].
- [Guideline] Johnson DA, Barkun AN, Cohen LB, Dominitz JA, Kaltenbach T, Martel M, et al. Optimizing adequacy of bowel cleansing for colonoscopy: recommendations from the US Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol. 2014 Oct. 109 (10):1528-45. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] Gupta S, Lieberman D, Anderson JC, Burke CA, Dominitz JA, Kaltenbach T, et al. Recommendations for Follow-Up After Colonoscopy and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2020 Feb 5. 143(3):844-57. [QxMD MEDLINE Link].
- [Guideline] Rutter MD, East J, Rees CJ, Cripps N, Docherty J, Dolwani S, et al. British Society of Gastroenterology/Association of Coloproctology of Great Britain and Ireland/Public Health England post-polypectomy and post-colorectal cancer resection surveillance guidelines. Gut. 2020 Feb. 69 (2):201-223. [QxMD MEDLINE Link]. [Full Text].
- Knudsen MD, Wang K, Wang L, Polychronidis G, Berstad P, Hjartåker A, et al. Colorectal Cancer Incidence and Mortality After Negative Colonoscopy Screening Results. JAMA Oncol. 2025 Jan 1. 11 (1):46-54. [QxMD MEDLINE Link].
- [Guideline] Sepulveda AR, Hamilton SR, Allegra CJ, Grody W, Cushman-Vokoun AM, Funkhouser WK, et al. Molecular Biomarkers for the Evaluation of Colorectal Cancer: Guideline From the American Society for Clinical Pathology, College of American Pathologists, Association for Molecular Pathology, and the American Society of Clinical Oncology. J Clin Oncol. 2017 May 1. 35 (13):1453-1486. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] Van Cutsem E, Cervantes A, Adam R, et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann Oncol. 2016 Aug. 27 (8):1386-422. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Colon Cancer. Available at https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf. Version 5.2024 — August 22, 2024; Accessed: January 17, 2025.
- American Joint Committee on Cancer. Colon and Rectum. Amin MB, Edge S, Greene F, Byrd DR, Brookland RK, et al, eds. AJCC Cancer staging manual. 8th ed. New York: Springer; 2017.
- Ogino S, Kawasaki T, Kirkner GJ, Ohnishi M, Fuchs CS. 18q loss of heterozygosity in microsatellite stable colorectal cancer is correlated with CpG island methylator phenotype-negative (CIMP-0) and inversely with CIMP-low and CIMP-high. BMC Cancer. 2007 May 2. 7:72. [QxMD MEDLINE Link].
- Jimeno A, Messersmith WA, Hirsch FR, Franklin WA, Eckhardt SG. KRAS Mutations and Sensitivity to Epidermal Growth Factor Receptor Inhibitors in Colorectal Cancer: Practical Application of Patient Selection. J Clin Oncol. 2009 Jan 5. [QxMD MEDLINE Link].
- Sargent DJ, Marsoni S, Monges G, Thibodeau SN, Labianca R, Hamilton SR, et al. Defective mismatch repair as a predictive marker for lack of efficacy of fluorouracil-based adjuvant therapy in colon cancer. J Clin Oncol. 2010 Jul 10. 28 (20):3219-26. [QxMD MEDLINE Link]. [Full Text].
- Ribic CM, Sargent DJ, Moore MJ, et al. Tumor microsatellite-instability status as a predictor of benefit from fluorouracil-based adjuvant chemotherapy for colon cancer. N Engl J Med. 2003 Jul 17. 349(3):247-57. [QxMD MEDLINE Link].
- Mlecnik B, Tosolini M, Kirilovsky A, Berger A, Bindea G, Meatchi T, et al. Histopathologic-based prognostic factors of colorectal cancers are associated with the state of the local immune reaction. J Clin Oncol. 2011 Feb 20. 29(6):610-8. [QxMD MEDLINE Link].
- Le Voyer TE, Sigurdson ER, Hanlon AL, et al. Colon cancer survival is associated with increasing number of lymph nodes analyzed: a secondary survey of intergroup trial INT-0089. J Clin Oncol. 2003 Aug 1. 21(15):2912-9. [QxMD MEDLINE Link].
- Gunderson LL, Jessup JM, Sargent DJ, Greene FL, Stewart AK. Revised TN categorization for colon cancer based on national survival outcomes data. J Clin Oncol. 2010 Jan 10. 28(2):264-71. [QxMD MEDLINE Link]. [Full Text].
- Hugen N, van de Velde CJ, de Wilt JH, Nagtegaal ID. Metastatic pattern in colorectal cancer is strongly influenced by histological subtype. Ann Oncol. 2014 Mar. 25(3):651-7. [QxMD MEDLINE Link].
- Boggs W. Histology influences colorectal cancer metastatic pattern. Reuters Health Information. March 11, 2014. [Full Text].
- [Guideline] Baxter NN, Kennedy EB, Bergsland E, Berlin J, George TJ, Gill S, et al. Adjuvant Therapy for Stage II Colon Cancer: ASCO Guideline Update. J Clin Oncol. 2021 Dec 22. 22(16):JCO2102538. [QxMD MEDLINE Link]. [Full Text].
- Boller AM, Nelson H. Colon and rectal cancer: laparoscopic or open?. Clin Cancer Res. 2007 Nov 15. 13(22 Pt 2):6894s-6s. [QxMD MEDLINE Link].
- Fleshman J, Sargent DJ, Green E, Anvari M, Stryker SJ, Beart RW Jr. Laparoscopic colectomy for cancer is not inferior to open surgery based on 5-year data from the COST Study Group trial. Ann Surg. 2007 Oct. 246(4):655-62; discussion 662-4. [QxMD MEDLINE Link].
- Jayne DG, Guillou PJ, Thorpe H, et al. Randomized trial of laparoscopic-assisted resection of colorectal carcinoma: 3-year results of the UK MRC CLASICC Trial Group. J Clin Oncol. 2007 Jul 20. 25(21):3061-8. [QxMD MEDLINE Link].
- Kuhry E, Schwenk WF, Gaupset R, Romild U, Bonjer HJ. Long-term results of laparoscopic colorectal cancer resection. Cochrane Database Syst Rev. 2008 Apr 16. CD003432. [QxMD MEDLINE Link].
- Lacy AM, Delgado S, Castells A, et al. The long-term results of a randomized clinical trial of laparoscopy-assisted versus open surgery for colon cancer. Ann Surg. 2008 Jul. 248(1):1-7. [QxMD MEDLINE Link].
- Veldkamp R, Kuhry E, Hop WC, et al. Laparoscopic surgery versus open surgery for colon cancer: short-term outcomes of a randomised trial. Lancet Oncol. 2005 Jul. 6(7):477-84. [QxMD MEDLINE Link].
- Vogel JD, Felder SI, Bhama AR, Hawkins AT, Langenfeld SJ, Shaffer VO, et al. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Colon Cancer. Dis Colon Rectum. 2022 Feb 1. 65 (2):148-177. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] Argilés G, Tabernero J, Labianca R, Hochhauser D, Salazar R, Iveson T, et al. Localised colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2020 Oct. 31 (10):1291-1305. [QxMD MEDLINE Link]. [Full Text].
- Poultsides GA, Servais EL, Saltz LB, Patil S, Kemeny NE, Guillem JG. Outcome of Primary Tumor in Patients With Synchronous Stage IV Colorectal Cancer Receiving Combination Chemotherapy Without Surgery As Initial Treatment. J Clin Oncol. 2009 Jun 1. [QxMD MEDLINE Link].
- Nitzkorski JR, Farma JM, Watson JC, Siripurapu V, Zhu F, Matteotti RS, et al. Outcome and natural history of patients with stage IV colorectal cancer receiving chemotherapy without primary tumor resection. Ann Surg Oncol. 2012 Feb. 19(2):379-83. [QxMD MEDLINE Link].
- Venderbosch S, de Wilt JH, Teerenstra S, et al. Prognostic value of resection of primary tumor in patients with stage IV colorectal cancer: retrospective analysis of two randomized studies and a review of the literature. Ann Surg Oncol. 2011 Nov. 18(12):3252-60. [QxMD MEDLINE Link]. [Full Text].
- Di Benedetto F, Berretta M, D'Amico G, et al. Liver resection for colorectal metastases in older adults: a paired matched analysis. J Am Geriatr Soc. 2011 Dec. 59(12):2282-90. [QxMD MEDLINE Link].
- Brouquet A, Overman MJ, Kopetz S, et al. Is resection of colorectal liver metastases after a second-line chemotherapy regimen justified?. Cancer. 2011 Oct 1. 117(19):4484-92. [QxMD MEDLINE Link]. [Full Text].
- House MG, Kemeny NE, Gonen M, et al. Comparison of adjuvant systemic chemotherapy with or without hepatic arterial infusional chemotherapy after hepatic resection for metastatic colorectal cancer. Ann Surg. 2011 Dec. 254(6):851-6. [QxMD MEDLINE Link].
- van Hooft JE, Bemelman WA, Oldenburg B, et al. Colonic stenting versus emergency surgery for acute left-sided malignant colonic obstruction: a multicentre randomised trial. Lancet Oncol. 2011 Apr. 12(4):344-52. [QxMD MEDLINE Link].
- Sargent D, Sobrero A, Grothey A, O'Connell MJ, Buyse M, Andre T, et al. Evidence for cure by adjuvant therapy in colon cancer: observations based on individual patient data from 20,898 patients on 18 randomized trials. J Clin Oncol. 2009 Feb 20. 27(6):872-7. [QxMD MEDLINE Link].
- Twelves C, Scheithauer W, McKendrick J, Seitz JF, Van Hazel G, Wong A, et al. Capecitabine versus 5-fluorouracil/folinic acid as adjuvant therapy for stage III colon cancer: final results from the X-ACT trial with analysis by age and preliminary evidence of a pharmacodynamic marker of efficacy. Ann Oncol. 2012 May. 23 (5):1190-1197. [QxMD MEDLINE Link]. [Full Text].
- Schmoll HJ, Tabernero J, Maroun J, de Braud F, Price T, Van Cutsem E, et al. Capecitabine Plus Oxaliplatin Compared With Fluorouracil/Folinic Acid As Adjuvant Therapy for Stage III Colon Cancer: Final Results of the NO16968 Randomized Controlled Phase III Trial. J Clin Oncol. 2015 Nov 10. 33 (32):3733-40. [QxMD MEDLINE Link]. [Full Text].
- André T, Boni C, Navarro M, Tabernero J, Hickish T, Topham C, et al. Improved overall survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage II or III colon cancer in the MOSAIC trial. J Clin Oncol. 2009 Jul 1. 27 (19):3109-16. [QxMD MEDLINE Link].
- van Erning FN, Creemers GJ, De Hingh IH, Loosveld OJ, Goey SH, Lemmens VE. Reduced risk of distant recurrence after adjuvant chemotherapy in patients with stage III colon cancer aged 75 years or older. Ann Oncol. 2013 Aug 8. [QxMD MEDLINE Link].
- André T, Iveson T, Labianca R, Meyerhardt JA, Souglakos I, Yoshino T, et al. The IDEA (International Duration Evaluation of Adjuvant Chemotherapy) Collaboration: Prospective Combined Analysis of Phase III Trials Investigating Duration of Adjuvant Therapy with the FOLFOX (FOLFOX4 or Modified FOLFOX6) or XELOX (3 versus 6 months) Regimen for Patients with Stage III Colon Cancer: Trial Design and Current Status. Curr Colorectal Cancer Rep. 2013. 9:261-269. [QxMD MEDLINE Link]. [Full Text].
- Lieu C, Kennedy EB, Bergsland E, Berlin J, George TJ, Gill S, et al. Duration of Oxaliplatin-Containing Adjuvant Therapy for Stage III Colon Cancer: ASCO Clinical Practice Guideline. J Clin Oncol. 2019 Jun 1. 37 (16):1436-1447. [QxMD MEDLINE Link]. [Full Text].
- Quasar Collaborative Group, Gray R, Barnwell J, et al. Adjuvant chemotherapy versus observation in patients with colorectal cancer: a randomised study. Lancet. 2007 Dec 15. 370(9604):2020-9. [QxMD MEDLINE Link].
- O'Connor ES, Greenblatt DY, LoConte NK, et al. Adjuvant chemotherapy for stage II colon cancer with poor prognostic features. J Clin Oncol. 2011 Sep 1. 29(25):3381-8. [QxMD MEDLINE Link]. [Full Text].
- Petrelli F, Labianca R, Zaniboni A, et al. Assessment of Duration and Effects of 3 vs 6 Months of Adjuvant Chemotherapy in High-Risk Stage II Colorectal Cancer: A Subgroup Analysis of the TOSCA Randomized Clinical Trial. JAMA Oncol. 2020 Feb 13. [QxMD MEDLINE Link].
- Kim GP, Sargent DJ, Mahoney MR, Rowland KM Jr, Philip PA, Mitchell E, et al. Phase III noninferiority trial comparing irinotecan with oxaliplatin, fluorouracil, and leucovorin in patients with advanced colorectal carcinoma previously treated with fluorouracil: N9841. J Clin Oncol. 2009 Jun 10. 27(17):2848-54. [QxMD MEDLINE Link]. [Full Text].
- Seymour MT, Thompson LC, Wasan HS, et al. Chemotherapy options in elderly and frail patients with metastatic colorectal cancer (MRC FOCUS2): an open-label, randomised factorial trial. Lancet. 2011 May 21. 377(9779):1749-59. [QxMD MEDLINE Link].
- Mayer RJ, Van Cutsem E, Falcone A, Yoshino T, Garcia-Carbonero R, Mizunuma N, et al. Randomized trial of TAS-102 for refractory metastatic colorectal cancer. N Engl J Med. 2015 May 14. 372 (20):1909-19. [QxMD MEDLINE Link].
- Prager GW, Taieb J, Fakih M, Ciardiello F, et al. Trifluridine-Tipiracil and Bevacizumab in Refractory Metastatic Colorectal Cancer. N Engl J Med. 2023 May 4. 388 (18):1657-1667. [QxMD MEDLINE Link]. [Full Text].
- Pawlik TM, Raut CP, Rodriguez-Bigas MA. Colorectal carcinogenesis: MSI-H versus MSI-L. Dis Markers. 2004. 20 (4-5):199-206. [QxMD MEDLINE Link]. [Full Text].
- Bennouna J, Sastre J, Arnold D, Osterlund P, Greil R, Van Cutsem E, et al. Continuation of bevacizumab after first progression in metastatic colorectal cancer (ML18147): a randomised phase 3 trial. Lancet Oncol. 2013 Jan. 14(1):29-37. [QxMD MEDLINE Link].
- Kabbinavar FF, Hurwitz HI, Yi J, Sarkar S, Rosen O. Addition of bevacizumab to fluorouracil-based first-line treatment of metastatic colorectal cancer: pooled analysis of cohorts of older patients from two randomized clinical trials. J Clin Oncol. 2009 Jan 10. 27(2):199-205. [QxMD MEDLINE Link].
- Goey KKH, Elias SG, van Tinteren H, Laclé MM, Willems SM, Offerhaus GJA, et al. Maintenance treatment with capecitabine and bevacizumab versus observation in metastatic colorectal cancer: updated results and molecular subgroup analyses of the phase 3 CAIRO3 study. Ann Oncol. 2017 Sep 1. 28 (9):2128-2134. [QxMD MEDLINE Link]. [Full Text].
- Tebbutt NC, Murphy F, Zannino D, et al. Risk of arterial thromboembolic events in patients with advanced colorectal cancer receiving bevacizumab. Ann Oncol. 2011 Aug. 22(8):1834-8. [QxMD MEDLINE Link].
- Allegra CJ, Yothers G, O'Connell MJ, Sharif S, Petrelli NJ, Colangelo LH, et al. Phase III trial assessing bevacizumab in stages II and III carcinoma of the colon: results of NSABP protocol C-08. J Clin Oncol. 2011 Jan 1. 29(1):11-6. [QxMD MEDLINE Link].
- Stark, Angela. FDA approves first biosimilar for the treatment of cancer. FDA News Release. 09/14/2017. Available at https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm576112.htm.
- Van Cutsem E, Köhne CH, Láng I, Folprecht G, Nowacki MP, Cascinu S, et al. Cetuximab plus irinotecan, fluorouracil, and leucovorin as first-line treatment for metastatic colorectal cancer: updated analysis of overall survival according to tumor KRAS and BRAF mutation status. J Clin Oncol. 2011 May 20. 29(15):2011-9. [QxMD MEDLINE Link].
- Van Cutsem E, Köhne CH, Hitre E, Zaluski J, Chang Chien CR, Makhson A, et al. Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N Engl J Med. 2009 Apr 2. 360(14):1408-17. [QxMD MEDLINE Link]. [Full Text].
- Cunningham D, Humblet Y, Siena S, et al. Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N Engl J Med. 2004 Jul 22. 351(4):337-45. [QxMD MEDLINE Link].
- Lin AY, Buckley NS, Lu AT, et al. Effect of KRAS mutational status in advanced colorectal cancer on the outcomes of anti-epidermal growth factor receptor monoclonal antibody therapy: a systematic review and meta-analysis. Clin Colorectal Cancer. 2011 Mar 1. 10(1):63-9. [QxMD MEDLINE Link].
- Chustecka Z. FDA Approves Panitumumab for Use With FOLFOX in mCRC. Medscape Medical News. Available at https://www.medscape.com/viewarticle/825699. Accessed: June 2, 2014.
- Douillard JY, Siena S, Cassidy J, Tabernero J, Burkes R, Barugel M, et al. Randomized, phase III trial of panitumumab with infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX4) versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastatic colorectal cancer: the PRIME study. J Clin Oncol. 2010 Nov 1. 28(31):4697-705. [QxMD MEDLINE Link].
- Peeters M, Price TJ, Cervantes A, Sobrero AF, Ducreux M, Hotko Y, et al. Randomized phase III study of panitumumab with fluorouracil, leucovorin, and irinotecan (FOLFIRI) compared with FOLFIRI alone as second-line treatment in patients with metastatic colorectal cancer. J Clin Oncol. 2010 Nov 1. 28(31):4706-13. [QxMD MEDLINE Link].
- Price TJ, Peeters M, Kim TW, Li J, Cascinu S, Ruff P, et al. Panitumumab versus cetuximab in patients with chemotherapy-refractory wild-type KRAS exon 2 metastatic colorectal cancer (ASPECCT): a randomised, multicentre, open-label, non-inferiority phase 3 study. Lancet Oncol. 2014 May. 15(6):569-79. [QxMD MEDLINE Link].
- Hecht JR, Mitchell E, Chidiac T, Scroggin C, Hagenstad C, Spigel D, et al. A randomized phase IIIB trial of chemotherapy, bevacizumab, and panitumumab compared with chemotherapy and bevacizumab alone for metastatic colorectal cancer. J Clin Oncol. 2009 Feb 10. 27(5):672-80. [QxMD MEDLINE Link].
- Douillard JY, Oliner KS, Siena S, Tabernero J, Burkes R, Barugel M, et al. Panitumumab-FOLFOX4 treatment and RAS mutations in colorectal cancer. N Engl J Med. 2013 Sep 12. 369(11):1023-34. [QxMD MEDLINE Link].
- Kim TW, Elme A, Kusic Z, Park JO, Udrea AA, Kim SY, et al. A phase 3 trial evaluating panitumumab plus best supportive care vs best supportive care in chemorefractory wild-type KRAS or RAS metastatic colorectal cancer. Br J Cancer. 2016 Nov 8. 115 (10):1206-1214. [QxMD MEDLINE Link]. [Full Text].
- VECTIBIX® (panitumumab) [package insert]. Thousand Oaks, CA: Amgen Inc. January 2025. Available at [Full Text].
- Tabernero J, Yoshino T, Cohn AL, Obermannova R, Bodoky G, Garcia-Carbonero R, et al. Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab, oxaliplatin, and a fluoropyrimidine (RAISE): a randomised, double-blind, multicentre, phase 3 study. Lancet Oncol. 2015 Apr 10. [QxMD MEDLINE Link].
- Overman MJ, McDermott R, Leach JL, Lonardi S, Lenz HJ, Morse MA, et al. Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (CheckMate 142): an open-label, multicentre, phase 2 study. Lancet Oncol. 2017 Jul 19. [QxMD MEDLINE Link]. [Full Text].
- Overman MJ, Lonardi S, Wong KYM, Lenz HJ, Gelsomino F, Aglietta M, et al. Durable Clinical Benefit With Nivolumab Plus Ipilimumab in DNA Mismatch Repair-Deficient/Microsatellite Instability-High Metastatic Colorectal Cancer. J Clin Oncol. 2018 Mar 10. 36 (8):773-779. [QxMD MEDLINE Link].
- Opdivo (nivolumab) [package insert]. Bristol-Myers Squibb Company: Princeton, NJ 08543 USA. 7/2017. Available at [Full Text].
- Le DT, Uram JN, Wang H, Bartlett BR, Kemberling H, Eyring AD, et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N Engl J Med. 2015 Jun 25. 372 (26):2509-20. [QxMD MEDLINE Link]. [Full Text].
- Stivarga (regorafenib) [package insert]. Wayne, NJ: Bayer HealthCare Pharmaceuticals Inc. September 2012. Available at [Full Text].
- Grothey A, Van Cutsem E, Sobrero A, Siena S, Falcone A, Ychou M, et al. Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): an international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet. 2013 Jan 26. 381 (9863):303-12. [QxMD MEDLINE Link].
- Li J, Qin S, Xu RH, et al. Effect of Fruquintinib vs Placebo on Overall Survival in Patients With Previously Treated Metastatic Colorectal Cancer: The FRESCO Randomized Clinical Trial. JAMA. 2018 Jun 26. 319 (24):2486-2496. [QxMD MEDLINE Link]. [Full Text].
- Dasari A, Lonardi S, Garcia-Carbonero R, et al. Fruquintinib versus placebo in patients with refractory metastatic colorectal cancer (FRESCO-2): an international, multicentre, randomised, double-blind, phase 3 study. Lancet. 2023 Jul 1. 402 (10395):41-53. [QxMD MEDLINE Link]. [Full Text].
- Patel A, Sun W. Ziv-aflibercept in metastatic colorectal cancer. Biologics. 2014. 8:13-25. [QxMD MEDLINE Link]. [Full Text].
- Van Cutsem E, et al. Aflibercept Plus FOLFIRI vs. Placebo Plus FOLFIRI in Second-Line Metastatic Colorectal Cancer: a Post Hoc Analysis of Survival from the Phase III VELOUR Study Subsequent to Exclusion of Patients who had Recurrence During or Within 6 Months of Completing Adjuvant Oxaliplatin-Based Therapy. Target Oncol. 2016 Jun. 11 (3):383-400. [QxMD MEDLINE Link]. [Full Text].
- Van Cutsem E, Tabernero J, Lakomy R, Prenen H, Prausová J, Macarulla T, et al. Addition of aflibercept to fluorouracil, leucovorin, and irinotecan improves survival in a phase III randomized trial in patients with metastatic colorectal cancer previously treated with an oxaliplatin-based regimen. J Clin Oncol. 2012 Oct 1. 30(28):3499-506. [QxMD MEDLINE Link].
- FDA approves an oncology drug that targets a key genetic driver of cancer, rather than a specific type of tumor. U.S. Food & Drug Administration. Available at https://www.fda.gov/news-events/press-announcements/fda-approves-oncology-drug-targets-key-genetic-driver-cancer-rather-specific-type-tumor. November 26, 2018; Accessed: June 5, 2019.
- FDA grants accelerated approval to encorafenib with cetuximab and mFOLFOX6 for metastatic colorectal cancer with a BRAF V600E mutation. U.S. Food & Drug Administration. Available at https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-encorafenib-cetuximab-and-mfolfox6-metastatic-colorectal-cancer-braf. December 20, 2024; Accessed: December 31, 2024.
- Kopetz S, Grothey A, Yaeger R, et al. Encorafenib, Binimetinib, and Cetuximab in BRAF V600E-Mutated Colorectal Cancer. N Engl J Med. 2019 Oct 24. 381 (17):1632-1643. [QxMD MEDLINE Link].
- Davenport L. Updated BEACON: Doublet as Good as Triplet in Metastatic CRC. Medscape Medical News. Available at https://www.medscape.com/viewarticle/931555. June 2, 2020; Accessed: February 11, 2021.
- Sartore-Bianchi A, Trusolino L, Martino C, Bencardino K, Lonardi S, et al. Dual-targeted therapy with trastuzumab and lapatinib in treatment-refractory, KRAS codon 12/13 wild-type, HER2-positive metastatic colorectal cancer (HERACLES): a proof-of-concept, multicentre, open-label, phase 2 trial. Lancet Oncol. 2016 Apr 20. [QxMD MEDLINE Link]. [Full Text].
- Otto MA. Tucatinib Plus Trastuzumab Approved for HER2+ Colorectal Cancer. Medscape Medical News. Available at https://www.medscape.com/viewarticle/987242. January 20, 2023; Accessed: December 31 2024.
- Hendlisz A, Van den Eynde M, Peeters M, Maleux G, Lambert B, Vannoote J, et al. Phase III trial comparing protracted intravenous fluorouracil infusion alone or with yttrium-90 resin microspheres radioembolization for liver-limited metastatic colorectal cancer refractory to standard chemotherapy. J Clin Oncol. 2010 Aug 10. 28(23):3687-94. [QxMD MEDLINE Link].
- Song M, Wu K, Meyerhardt JA, Ogino S, Wang M, Fuchs CS, et al. Fiber Intake and Survival After Colorectal Cancer Diagnosis. JAMA Oncol. 2017 Nov 2. [QxMD MEDLINE Link]. [Full Text].
- Van Blarigan EL, Ou FS, Bainter TM, Fuchs CS, Niedzwiecki D, Zhang S, et al. Associations Between Unprocessed Red Meat and Processed Meat With Risk of Recurrence and Mortality in Patients With Stage III Colon Cancer. JAMA Netw Open. 2022 Feb 1. 5 (2):e220145. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] Meyerhardt JA, Mangu PB, Flynn PJ, Korde L, Loprinzi CL, Minsky BD, et al. Follow-Up Care, Surveillance Protocol, and Secondary Prevention Measures for Survivors of Colorectal Cancer: American Society of Clinical Oncology Clinical Practice Guideline Endorsement. J Clin Oncol. 2013 Nov 12. [QxMD MEDLINE Link].
- [Guideline] Labianca R, Nordlinger B, Beretta GD, Mosconi S, Mandalà M, Cervantes A, et al. Early colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013 Oct. 24 Suppl 6:vi64-72. [QxMD MEDLINE Link].
- [Guideline] Kahi CJ, Boland CR, Dominitz JA, Giardiello FM, Johnson DA, Kaltenbach T, et al. Colonoscopy Surveillance After Colorectal Cancer Resection: Recommendations of the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2016 Mar. 150 (3):758-768.e11. [QxMD MEDLINE Link]. [Full Text].
- Kirkegaard H, Johnsen NF, Christensen J, Frederiksen K, Overvad K, Tjonneland A. Association of adherence to lifestyle recommendations and risk of colorectal cancer: a prospective Danish cohort study. BMJ. 2010 Oct 26. 341:c5504. [QxMD MEDLINE Link]. [Full Text].
- Kim J, Boushey CJ, Wilkens LR, Haiman CA, Le Marchand L, Park SY. Plant-based dietary patterns defined by a priori indices and colorectal cancer risk by sex and race/ethnicity: the Multiethnic Cohort Study. BMC Med. 2022 Nov 29. 20 (1):430. [QxMD MEDLINE Link]. [Full Text].
- Meyerhardt JA, Heseltine D, Niedzwiecki D, Hollis D, Saltz LB, Mayer RJ, et al. Impact of physical activity on cancer recurrence and survival in patients with stage III colon cancer: findings from CALGB 89803. J Clin Oncol. 2006 Aug 1. 24(22):3535-41. [QxMD MEDLINE Link].
- Baron JA, Barry EL, Mott LA, Rees JR, Sandler RS, et al. A Trial of Calcium and Vitamin D for the Prevention of Colorectal Adenomas. N Engl J Med. 2015 Oct 15. 373 (16):1519-30. [QxMD MEDLINE Link]. [Full Text].
- Barry EL, Peacock JL, Rees JR, Bostick RM, Robertson DJ, Bresalier RS, et al. Vitamin D Receptor Genotype, Vitamin D3 Supplementation, and Risk of Colorectal Adenomas: A Randomized Clinical Trial. JAMA Oncol. 2016 Dec 15. [QxMD MEDLINE Link].
- McCullough ML, Zoltick ES, Weinstein SJ, Fedirko V, Wang M, et al. Circulating Vitamin D and Colorectal Cancer Risk: An International Pooling Project of 17 Cohorts. J Natl Cancer Inst. 2018 Jun 14. [QxMD MEDLINE Link].
- Arber N, Spicak J, Rácz I, Zavoral M, Breazna A, Gerletti P, et al. Five-year analysis of the prevention of colorectal sporadic adenomatous polyps trial. Am J Gastroenterol. 2011 Jun. 106(6):1135-46. [QxMD MEDLINE Link].
- Flossmann E, Rothwell PM. Effect of aspirin on long-term risk of colorectal cancer: consistent evidence from randomised and observational studies. Lancet. 2007 May 12. 369(9573):1603-13. [QxMD MEDLINE Link].
- Cole BF, Logan RF, Halabi S, Benamouzig R, Sandler RS, Grainge MJ, et al. Aspirin for the chemoprevention of colorectal adenomas: meta-analysis of the randomized trials. J Natl Cancer Inst. 2009 Feb 18. 101(4):256-66. [QxMD MEDLINE Link].
- Zhang X, Smith-Warner SA, Chan AT, et al. Aspirin Use, Body Mass Index, Physical Activity, Plasma C-Peptide, and Colon Cancer Risk in US Health Professionals. Am J Epidemiol. 2011 Aug 15. 174(4):459-67. [QxMD MEDLINE Link].
- Nishihara R, Lochhead P, Kuchiba A, Jung S, Yamauchi M, Liao X, et al. Aspirin use and risk of colorectal cancer according to BRAF mutation status. JAMA. 2013 Jun 26. 309(24):2563-71. [QxMD MEDLINE Link].
- Cook NR, Lee IM, Zhang SM, Moorthy MV, Buring JE. Alternate-Day, Low-Dose Aspirin and Cancer Risk: Long-Term Observational Follow-up of a Randomized Trial. Ann Intern Med. 2013 Jul 16. 159(2):77-85. [QxMD MEDLINE Link].
- Meyskens FL Jr, McLaren CE, Pelot D, Fujikawa-Brooks S, Carpenter PM, Hawk E, et al. Difluoromethylornithine plus sulindac for the prevention of sporadic colorectal adenomas: a randomized placebo-controlled, double-blind trial. Cancer Prev Res (Phila Pa). 2008 Jun. 1(1):32-8. [QxMD MEDLINE Link].
- [Guideline] National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Colorectal Cancer Screening. NCCN. Available at https://www.nccn.org/professionals/physician_gls/pdf/colorectal_screening.pdf. Version 1.2024 — February 27, 2024; Accessed: January 17, 2025.
- [Guideline] Stjepanovic N, Moreira L, Carneiro F, Balaguer F, Cervantes A, Balmaña J, et al. Hereditary gastrointestinal cancers: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann Oncol. 2019 Oct 1. 30 (10):1558-1571. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] Qaseem A, Crandall CJ, Mustafa RA, Hicks LA, Wilt TJ, Clinical Guidelines Committee of the American College of Physicians., et al. Screening for Colorectal Cancer in Asymptomatic Average-Risk Adults: A Guidance Statement From the American College of Physicians. Ann Intern Med. 2019 Nov 5. 171 (9):643-654. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] American Cancer Society Guideline for Colorectal Cancer Screening. American Cancer Society. Available at https://www.cancer.org/cancer/colon-rectal-cancer/detection-diagnosis-staging/acs-recommendations.html. May 30, 2018; Accessed: May 25, 2019.
- [Guideline] Rubenstein JH, Enns R, Heidelbaugh J, Barkun A, Clinical Guidelines Committee. American Gastroenterological Association Institute Guideline on the Diagnosis and Management of Lynch Syndrome. Gastroenterology. 2015 Sep. 149 (3):777-82; quiz e16-7. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] Stoffel EM, Mangu PB, Gruber SB, Hamilton SR, Kalady MF, Lau MW, et al. Hereditary colorectal cancer syndromes: American Society of Clinical Oncology Clinical Practice Guideline endorsement of the familial risk-colorectal cancer: European Society for Medical Oncology Clinical Practice Guidelines. J Clin Oncol. 2015 Jan 10. 33 (2):209-17. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] Steele SR, Chang GJ, Hendren S, Weiser M, Irani J, Buie WD, et al. Practice Guideline for the Surveillance of Patients After Curative Treatment of Colon and Rectal Cancer. Dis Colon Rectum. 2015 Aug. 58 (8):713-25. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] Cervantes A, Adam R, Roselló S, Arnold D, Normanno N, Taïeb J, et al. Metastatic colorectal cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2023 Jan. 34 (1):10-32. [QxMD MEDLINE Link]. [Full Text].
- [Guideline] Allegra CJ, Rumble RB, Hamilton SR, Mangu PB, Roach N, Hantel A, et al. Extended RAS Gene Mutation Testing in Metastatic Colorectal Carcinoma to Predict Response to Anti-Epidermal Growth Factor Receptor Monoclonal Antibody Therapy: American Society of Clinical Oncology Provisional Clinical Opinion Update 2015. J Clin Oncol. 2016 Jan 10. 34 (2):179-85. [QxMD MEDLINE Link]. [Full Text].
- Tournigand C, Andre T, Achille E, et al. FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer: a randomized GERCOR study. J Clin Oncol. 2004 Jan 15. 22(2):229-37. [QxMD MEDLINE Link].
- Arkenau HT, Arnold D, Cassidy J, Diaz-Rubio E, Douillard JY, Hochster H, et al. Efficacy of oxaliplatin plus capecitabine or infusional fluorouracil/leucovorin in patients with metastatic colorectal cancer: a pooled analysis of randomized trials. J Clin Oncol. 2008 Dec 20. 26(36):5910-7. [QxMD MEDLINE Link].
- Sehgal R, Lembersky BC, Rajasenan KK, et al. A Phase I/II Study of Capecitabine Given on a Week on/Week off Schedule Combined With Bevacizumab and Oxaliplatin for Patients With Untreated Advanced Colorectal Cancer. Clin Colorectal Cancer. 2011 Jun. 10(2):117-20. [QxMD MEDLINE Link].
Author
Coauthor(s)
Vassiliki Liana Tsikitis, MD, MBA, MCR, FACS, FASCRS Professor of Surgery, Head, Division of Gastrointestinal and General Surgery, Vice Chair, Diversity Equity and Inclusion, Department of Surgery, Oregon Health and Science University School of Medicine
Vassiliki Liana Tsikitis, MD, MBA, MCR, FACS, FASCRS is a member of the following medical societies: Alpha Omega Alpha, American College of Surgeons, American Society of Colon and Rectal Surgeons, Association of Women Surgeons, European Society of Coloproctology, International Society of Surgery, Mayo Clinic Alumni Association, Pacific Coast Surgical Association, Society for Surgery of the Alimentary Tract, Society of University Surgeons, The Priestley Society, Western Surgical Association
Disclosure: Nothing to disclose.
Specialty Editor Board
Francisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical Center College of Pharmacy; Editor-in-Chief, Medscape Drug Reference
Disclosure: Received salary from Medscape for employment. for: Medscape.
Chief Editor
N Joseph Espat, MD, MS, FACS Harold J Wanebo Professor of Surgery, Assistant Dean of Clinical Affairs, Boston University School of Medicine; Chairman, Department of Surgery, Director, Adele R Decof Cancer Center, Roger Williams Medical Center
N Joseph Espat, MD, MS, FACS is a member of the following medical societies: Alpha Omega Alpha, American Association for Cancer Research, American College of Surgeons, American Medical Association, American Society for Parenteral and Enteral Nutrition, American Society of Clinical Oncology, Americas Hepato-Pancreato-Biliary Association, Association for Academic Surgery, Central Surgical Association, Chicago Medical Society, International Hepato-Pancreato-Biliary Association, Pancreas Club, Sigma Xi, The Scientific Research Honor Society, Society for Leukocyte Biology, Society for Surgery of the Alimentary Tract, Society of American Gastrointestinal and Endoscopic Surgeons, Society of Surgical Oncology, Society of University Surgeons, Southeastern Surgical Congress, Southern Medical Association, Surgical Infection Society
Disclosure: Nothing to disclose.
Additional Contributors
Elwyn C Cabebe, MD Associate Medical Director, Stanford Cancer Networks; Medical Director, Stanford Cancer Center South Bay (CCSB); Medical Director of Oncology Quality, Stanford Medical Partners
Elwyn C Cabebe, MD is a member of the following medical societies: American Association for Cancer Research, American Society of Clinical Oncology, Association of Northern California Oncologists, Philippine Medical Society of Northern California, Santa Clara County Medical Association, Monterey County Medical Society
Disclosure: Nothing to disclose.