International Prevalence of Self-exclusion From Gambling: a Systematic Review and Meta-analysis (original) (raw)
Introduction
For more than 20 years, gambling operators internationally have offered customers the option to exclude or bar themselves from gambling to minimise gambling-related harm [1]. Self-exclusion is a form of stimulus control that employs a formalised process for preventing access to gambling products. More specifically, self-exclusion programmes involve an agreement between a gambling operator and customer that the customer will be unable to access or use gambling products for a specified period that can range from as little as 3 months to a lifetime, depending on the jurisdiction [2]. Promoted as part of a suite of “responsible gambling” tools, provision of self-exclusion is often a mandatory requirement under licencing conditions for both land-based and online gambling operators [3].
Self-exclusion processes vary by gambling operator and multiple barriers exist that may discourage initiation of the process. In particular, the arduous process of signing up to self-exclusion has been described as one of the main barriers to uptake, as well as associated shame and embarrassment [4]. Land-based programmes have historically required in-person registration, with some jurisdictions requiring the person to enter and register at each venue from which they want to exclude [1, 4]. People who elected to exclude often also needed to provide a photograph to enable detection of breaches of the self-exclusion contract [1]. Still, breaches were common due to inadequate monitoring and enforcement of self-exclusion contracts [1]. In contrast, online betting exclusions usually operate through operator websites, making them less onerous as there is no interview or interaction with a person and no requirement of a photograph [5•, 6•]. Self-exclusion processes have gradually changed in some jurisdictions, with the roll-out of online multi-venue exclusion options from land-based gambling operators [7, 8] and exclusions that cover all forms of land-based and online gambling [6•].
Self-exclusion is one of the most researched harm reduction approaches. Systematic review evidence has found that self-exclusion leads to reduced gambling behaviour and gambling-related harm during the period of self-exclusion [9••]. Reduced gambling through self-exclusion has potential flow-on effects, such as improvement to mental health, reduced life stress, and financial problems [10]. Financial problems associated with gambling expenditure are the predominant reason for people to self-exclude, while other important motivators are wanting to regain control, wishing to reduce conflict with significant others, and realising that there is a gambling problem [1, 4, 11••]. Research shows that the majority of self-excluders are on the higher end of the gambling risk continuum [1, 11••]. Furthermore, although self-exclusion is more common among those with current gambling problems, there is evidence that it is also used by those without recent problems [6•].
In line with increasing availability of gambling opportunities worldwide [12,13,14], more attention has been devoted to the reduction of gambling-related harm and promotion of “responsible gambling” tools, including self-exclusion [3]. Research implies that information on “responsible gambling” is largely disregarded by those who gamble [15, 16] and it has been suggested that self-exclusion is underutilised by those at the higher end of the gambling risk continuum [13, 16]. There have been numerous reviews of the self-exclusion literature, all focusing primarily on the presence of gambling problems in samples of people who have self-excluded [1, 4, 11••]. To date, however, there has been no systematic investigation of the uptake and awareness of self-exclusion programmes in the general population. To address this gap, the primary aim of the present systematic review and meta-analysis was to identify the international prevalence of self-exclusion from gambling among the adult general population and among those at varying levels of problem gambling risk (low-risk, moderate-risk, and problem gambling). The secondary aim was to identify the international prevalence of awareness of self-exclusion programmes among the general population and in people at various levels of problem gambling risk.
The current study builds on methodology developed in our recent systematic review and meta-analysis on the prevalence of help-seeking for problem gambling in the general population [17•]. This meta-analysis reported a global prevalence of help seeking based on data extracted from 24 large-scale representative studies. The findings revealed that one in five people with problem gambling had sought help. Based on our previous work, it is expected that prevalence estimates related to self-exclusion vary depending on various factors including the geographic location of the prevalence study and the methodological design used to estimate the prevalence. Such heterogeneity is a common occurrence across literature presenting estimates of gambling and gambling behaviour. For example, the help-seeking review showed that the pooled prevalence of help-seeking for gambling problems was significantly higher when people were asked if they had sought help in their lifetime compared to in the past year [17•]. Furthermore, in line with differences in gambling behaviour observed between those engaging in online and land-based gambling [13, 14], self-exclusion estimates may vary depending on whether the studies focus on self-exclusion from online or land-based gambling operators. As such, the current study also investigated potential variability in international estimates of self-exclusion uptake and awareness by exclusion type (land-based or online self-exclusion), region (Australasian or North American), measurement timeframe (past 12 months or ever self-exclusion), and year of data collection, where possible.
Methods
The methodology in this review is consistent with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) and Meta-analyses of Observational Studies (MOOSE) guidelines [18, 19]. The review was registered a-priori with PROSPERO (CRD42022344338). In the PROSPERO protocol, studies described as using representative panel data (i.e. panels that enable recruitment resulting in a distribution of demographic characteristics of the study sample similar to that of the general population) were deemed eligible for inclusion in the review. However, since registration, a meta-analysis of gambling prevalence studies in the UK was published which showed that estimates from panel studies were almost two to four times higher than estimates reported in their non-panel counterparts [20]. Based on these findings, the inclusion criteria regarding sampling methods were adjusted as it was decided that it was unreasonable to pool data from panel and non-panel studies.
Eligibility Criteria
Studies were included if they (1) were published in English language from 2010 onwards and described data collection that commenced after 1 January 2010 to ensure that current evidence was captured; (2) employed representative sampling methods to determine the prevalence of gambling participation or problem gambling; (3) included over half of study participants aged 18 years or over; (4) provided an estimate of the prevalence of self-exclusion from gambling (defined as an agreement between an individual and a gambling operator to have a period of prohibited access to gambling land-based venues or websites/apps) and/or awareness thereof in the study population; and (5) provided sufficient data to calculate the prevalence of self-exclusion and/or awareness of self-exclusion programmes (e.g. studies needed to include data on the number of participants administered the self-exclusion items). Studies were excluded if the (1) primary aim of data collection was not related to the prevalence of gambling participation or problem gambling; (2) focus was only on other methods to prevent access to gambling opportunities such as website or banking blocks; (3) study population consisted of a help-seeking sample (e.g. in-person treatment seekers) or specific populations (e.g. university students, prisoners, migrants, casino or gaming patrons, specific age groups, or those attending mental health services); (4) publication was a book, conference paper, or presentation; and (5) data were presented in another included source which provided more detailed data. The items measuring self-exclusion did not need to form a validated screen as none currently exists.
Search Strategy
Systematic grey and scientific literature searches were conducted to identify gambling prevalence studies published from January 2010 to August 2022. The main target of the systematic search was grey literature (e.g. reports and government publications) as these records are most likely to contain more elaborate information on topics related to self-exclusion prevalence. The searched sources were gambling research repositories (i.e. the Gambling Research Exchange Ontario Evidence Centre, Gamble Aware, UK Gambling Commission Library) and gambling research institutes in each country or region with regulated gambling (e.g. Victorian Responsible Gambling Foundation, National Council on Problem Gambling, Alberta Gambling Research Institute, Australasian Gaming Council, University of Nevada, Las Vegas Center for Gaming Research). Furthermore, country-specific domains were searched using the search terms gambling and prevalence in combination with the country or state to identify region-specific records that were potentially missed in the other sources. Google searches were limited by screening the first 50 records per search. Scientific electronic databases (ProQuest, Ovid PsycINFO, PubMed, and Scopus) were searched using a combination of key words and wildcards related to gambling (gambl*) and prevalence studies (i.e. prevalence, population, representative, nation*, epidemiolog*, cross-sectional, participation). Where appropriate, additional limits were placed on each database (e.g. year restriction, subject area). Finally, a manual search of the reference lists of previous systematic reviews on problem gambling prevalence [21, 22] was performed to identify further relevant studies. A detailed overview of the search strategy and search dates is provided in Appendix 1.
Study Selection
It was assumed data on self-exclusion may be reported as a secondary result of gambling prevalence studies without mention in abstracts or summaries of reports. As such, screening started with identification of potentially relevant gambling prevalence studies conducted from 1st of January onwards and published in English language. For reports and government publications, full texts were retrieved for all records reflecting gambling prevalence surveys and eligibility was assessed by screening the title, table of contents, and executive summary, and performing a key word search of the full texts using terms related to self-exclusion (e.g. exclu, ban, locked). For peer-reviewed articles, eligibility was assessed based on screening titles and abstracts. Subsequently, all full texts of grey and scientific literature were assessed against the full set of selection criteria. Screening was performed by two reviewers (RB and NB), with half of the identified records being double screened. Concordance was achieved for 95% of records, with discrepancies resolved through group discussion (RB, NB, and SR).
Data Extraction and Risk of Bias Assessment
A structured Microsoft Excel data extraction form was used to extract data from the eligible studies. Extracted data included descriptive characteristics (e.g. location, funding, recruitment methods, year and mode of data collection, problem gambling measure), sample characteristics (e.g. sample size, problem gambling estimates), and data on self-exclusion (e.g. self-exclusion item/s, type of self-exclusion, timeframe of self-exclusion measurement, the subsample to which the self-exclusion item/s was administered, self-exclusion prevalence estimates). Extraction of weighted prevalence estimates was prioritised over unweighted estimates, where available. Quality of the studies was evaluated using a selection of items from the 10-item Risk of Bias tool for prevalence studies [23]. Specifically, five items were selected that were relevant to the component of the studies that covered self-exclusion and evaluated bias related to the sampling frame (i.e. whether it was a true or close presentation of the target population), participant selection within sampling frame (i.e. whether it was random or a census), item-non-response (i.e. whether the likelihood of non-response biases to the self-exclusion item was minimal), definition of self-exclusion (i.e. whether an acceptable definition of self-exclusion was used), and data-collection mode (i.e. whether the same mode of data collection was used for all participants when administering the self-exclusion item) (see Appendix 2 for the interpretations and examples of the Risk of Bias tool items). For each item, risk of bias was scored as low or high risk, or as not reported if there was insufficient information reported to adequately score risk of bias. Data extraction and risk of bias assessment were performed independently by two reviewers (RB and NB) for each of the included studies with a concordance estimate of 96%. Discrepancies in data extraction and bias assessment were resolved through group discussion with the wider research team (RB, NB, ND, and SR).
Data Analysis
All meta-analyses were performed using the metafor package [24] in R software v4.1.1 [25]. The effect size measures in the meta-analytic models reflected the proportions of self-exclusion use (i.e. primary analysis) and self-exclusion awareness (i.e. secondary analysis) in the population-representative sample. All meta-analyses were conducted using a binomial-normal model, with logit links [26]. The resulting estimates of the average log odds were back-transformed to retrieve the median pooled prevalence estimates. Weighting of effect sizes was based on the inverse of their variance. Random effects models were used because of the expected heterogeneity between the studies included in the meta-analysis. Heterogeneity of the meta-analytic estimates was evaluated using the _I_2 statistic, where _I_2 values of 25%, 50%, and 75% may be interpreted as low, moderate, and high levels of heterogeneity, respectively [27]. Potential moderators of the estimated proportion were investigated in a series of subgroup analyses and meta-regressions. In each subgroup analyses, a categorical variable (i.e. self-exclusion type, region, measurement timeframe, and level of problem gambling) was included reflecting a potential moderator, whereas in the meta-regression, a continuous variable (i.e. data collection year) was included reflecting a potential moderator. In line with Cochrane recommendations [28], meta-analyses were performed where at least two prevalence estimates were available per model and study data could be meaningfully pooled. An overview of all decision rules related to data extraction and analysis is shown in Appendix 3.
Sensitivity Analysis and Publication Bias
A series of sensitivity analyses were conducted to examine whether the meta-analytic estimates were robust to methodological quality of the included studies. For each risk of bias item, a sensitivity analysis was conducted in which the included studies were restricted to studies assessed as having low risk of bias on the respective item. Publication bias was evaluated with funnel plots for the prevalence estimates of self-exclusion and awareness thereof with sample sizes plotted on the _y_-axis as a measure of accuracy [29]. Subsequently, the trim-and-fill procedure [30] was used to adjust the estimates for publication bias [31].
Additional Analyses
Subgroup analysis was performed to compare self-exclusion prevalence estimates by gambling risk (low-risk, moderate-risk, or problem gambling) classified as per Problem Gambling Severity Index (PGSI) risk categories [32]. Subgroup analyses were also conducted to explore factors that may explain the variability in the meta-analytic estimates. These analyses included subgroups by (1) type (land-based or online self-exclusion); (2) region (North America versus Australasia); and (3) measurement timeframe (past 12 months or ever self-exclusion), with the last subgroup analysis only being applicable to use of self-exclusion but not awareness. Variability related to year of data collection was explored in meta-regression.
Results
Study Selection
The grey literature search yielded 6637 records which resulted in the review of 45 full-text documents. The scientific database search yielded another 8592 records which, after duplicate removal, resulted in screening 4691 records and reviewing 22 full-text documents. After assessing the full-text documents against the full set of eligibility criteria, 15 studies were included in the meta-analysis [33,34,35,36,37,38,39,40,41,42,43,44,45,46,47], of which 11 reported on the prevalence of self-exclusion [33, 34, 38, 39, 41,42,43,44,45,46,47] and five reported on the prevalence of self-exclusion awareness [35,36,37, 40, 41]. Figure 1 provides an overview of the study selection process. Excluded studies presenting panel data comprised surveys from Sweden, the UK, and Canada. Appendix 4 reports on the reasons for exclusion of the 52 reviewed full-text studies, organised by region.
Fig. 1
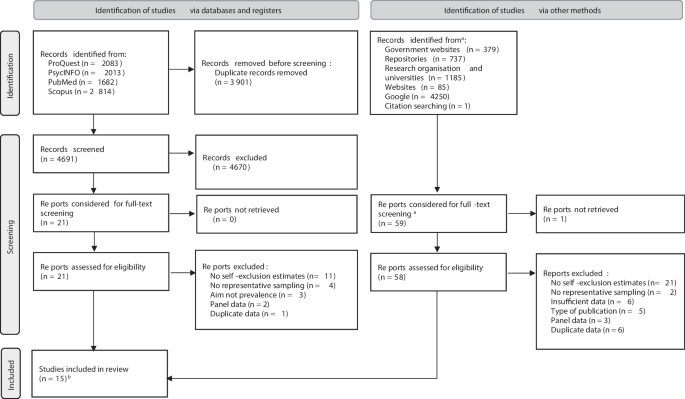
PRISMA flow diagram of study selection. See Appendix 1 for a complete list of identified and searched sources. aFor the first phase of screening, we retrieved full texts of all records from grey literature to enable search of executive summary, table of contents, and key words. bAll from grey literature
Characteristics of Included Studies
Appendix 5 provides an overview of the overall characteristics of included studies. The majority of studies were from the Australasian region (80.0%, k = 12) and the rest was from the North American region (20.0%, k = 3). Data collection was most commonly conducted by telephone (93.3%, k = 14), while the remaining study used a combination of data collection via telephone, mail, and online surveys. Individuals eligible to respond to the surveys were aged 18 years or older in all studies. The response rate for the overall survey ranged from 7.5 to 44.6%. Overall study sample size ranged from 1761 to 20,017 respondents (median = 9578). All studies administered the PGSI to determine problem gambling risk and reported that between 3.9–7.7% of respondents in the overall study population were in the low-risk gambling category, 1.1–3.7% in the moderate-risk gambling category, and 0.4–1.4% in the problem gambling category.
Tables 1 and 2 show self-exclusion-related data among the included studies reporting on use of self-exclusion (73.3%, k = 11) and awareness of self-exclusion (33.3%, k = 5). Over half of the studies reported the prevalence of self-exclusion use or awareness by one or more PGSI categories of problem gambling risk (60.0%, k = 9). Studies reported estimates of self-exclusion from land-based gambling operators (60.0%, k = 9), or from online gambling operators (26.7%, k = 4), or as an overall estimate of self-exclusion from any type of gambling operator (13.3%, k = 2). Most studies reported past 12 months use of self-exclusion (53.3%, k = 8), while some reported ever self-exclusion (26.7%, k = 4), and one reported data for both measurement timeframes. Almost all studies administered survey items related to self-exclusion to a subsample of the overall population (86.7%, k = 13). Samples were commonly limited to respondents who reported gambling in the past year or those who had a PGSI score above a certain risk score.
Table 1 Study data on self-exclusion from gambling operators
Table 2 Study data on awareness of self-exclusion options
Risk of Bias
Risk of bias assessment was performed on the study components that related to the use of self-exclusion or awareness of self-exclusion to examine the degree to which the findings were robust to methodological quality of the included studies (Table 3). Among the 11 studies with a component on use of self-exclusion, bias related to the sampling frame was classified as high risk in all but one of the included studies (90.9%, k = 10). Selection of respondents within the sampling frame, however, was mostly rated as low risk of bias (90.9%, k = 10). Only two studies reported response rates of the self-exclusion item and both were classified as having low risk of bias related to item-non-response (18.2%, k = 2). The majority of studies were classified as having a low risk of bias related to the definition of self-exclusion (81.8%, k = 9) and to the data collection mode (90.9%, k = 10). All five studies with a study component on awareness of self-exclusion were rated as low risk of for bias related to selection of respondents, definition of the self-exclusion awareness item, and data collection mode. Bias related to the sampling frame was classified as high in all but one study (80.0%, k = 4), while bias related to item-response rate was classified as low in one study and not reported in the other studies reporting estimates on self-exclusion awareness (80.0%, k = 4).
Table 3 Risk of bias assessment of included studies
Meta-analysis
Use of Self-exclusion
Of the 15 included studies, 11 provided data to calculate the general population estimate of self-exclusion. The median prevalence of self-exclusion in the primary analysis was 0.26% (95%CI 0.16–0.43) of the general adult population, with high levels of between-study heterogeneity (_I_2 = 94.43). Figure 2 provides an overview of the meta-analytic results from the primary analysis.
Fig. 2
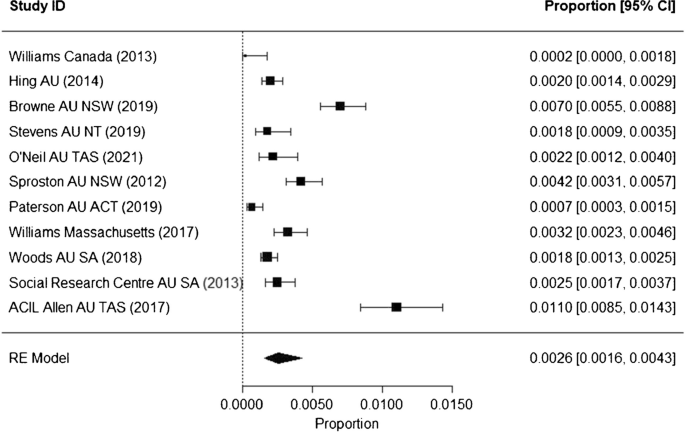
Forest plot showing meta-analytic results of the prevalence of self-exclusion use. Note: Studies presented in order of descending sample size
The sensitivity analyses replicated the primary analysis but restricted the meta-analysis to studies that were scored as having low risk of bias on the items used to assess quality of the included studies. Meta-analytic results of the sensitivity analyses were similar to results of the main analysis (Table 4). Funnel plots were used to examine publication bias (Appendix 6). Visual inspection of the funnel plot for the main model suggested some asymmetry. The trim-and-fill procedure imputed three studies on the right of the plot. After this procedure, a slightly higher adjusted prevalence (0.35%, 95%CI 0.20–0.62) was observed compared to prevalence of the main model (0.26% 95%CI 0.16–0.43).
Table 4 Meta-analytic results estimating the prevalence of self-exclusion
The estimated prevalence of self-exclusion among participants classified in the PGSI problem-gambling category (15.20%, 95%CI 11.00–19.39) was significantly higher than among participants classified in the PGSI moderate-risk gambling category (2.50%, 95%CI 1.32–4.69, p < 0.001) or the PGSI low-risk gambling category (0.53%, 95%CI 0.05–5.48, p < 0.001).
Potentially relevant sources of heterogeneity between the studies included in the main analysis were assessed by conducting subgroup analyses (Table 5). Although the self-exclusion prevalence was considerably higher in Australasia (0.28%, 95%CI 0.17–0.46) compared to North America (0.11%, 95%CI 0.02–0.70), there was no evidence of a significant difference between the regions (p = 0.270). Subgroup analyses also did not reveal any systemic variation in the prevalence estimates by type of gambling self-exclusion (land-based versus online gambling) or timeframe indicated in the self-exclusion item (past 12 months versus ever). Meta-regression results of data collection year did not indicate a significant association (p = 0.658).
Table 5 Meta-analytic results estimating the prevalence of self-exclusion by subgroup
Awareness of Self-exclusion
Five of the included studies reported on awareness of self-exclusion (Table 6 and Fig. 3). The median prevalence of self-exclusion awareness among the general population was 11.09% (95%CI 6.67–17.89), with high levels between-study heterogeneity (_I_2 = 99.70). No sensitivity analyses were conducted as the risk of bias was scored as low in all or in less than two studies for each of the risk of bias items. The funnel plot showed no asymmetry and no procedures were required to adjust for publication bias (Appendix 6).
Table 6 Meta-analytic results estimating the prevalence self-exclusion awareness
Fig. 3
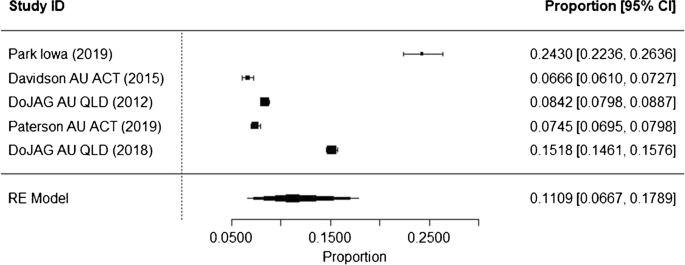
Forest plot showing meta-analytic results of the prevalence of self-exclusion awareness. Notes: Studies presented in order of descending sample size; DoJAG, Department of Justice and Attorney-General
Two studies reported awareness prevalence by subgroup of problem gambling risk. Pooling these data showed that the prevalence of self-exclusion awareness among participants classified in the PGSI problem gambling category (81.37%, 95%CI 58.36–93.16) was significantly higher than participants classified in the PGSI low-risk gambling category (57.79%, 95%CI 42.87–71.41, p = 0.029), but not participants classified in the PGSI moderate-risk gambling category (67.26%, 95%CI 58.57–74.90).
The relatively small number of studies reporting awareness of self-exclusion estimates precluded the option of performing subgroup analyses to explore potential causes of heterogeneity. Only one study from the North American region asked about awareness, no studies referred specifically to awareness of self-exclusion from online gambling operators, and timeframe was not applicable to items on awareness of self-exclusion. Meta-regression by year of data collection did not show a significant association (p = 0.338).
Discussion
This meta-analysis was the first to estimate the international prevalence of gambling self-exclusion and awareness of self-exclusion programmes. Based on pooled data of 11 studies, the current study estimated an international prevalence of self-exclusion from gambling operators of 0.26%. Sensitivity analysis showed that this estimate was relatively robust when assessed against risk of bias in the included studies. Prevalence estimates were significantly increased in people classified at the higher end of the gambling risk spectrum, with about one in seven people classified in the problem gambling category having self-excluded, compared to one in 40 classified in the moderate-risk gambling category and around one in 200 classified in the low-risk gambling category. Based on pooled data of five studies, estimates showed that, internationally, 11% of the adult population was aware of self-exclusion programmes. Awareness of self-exclusion was also higher in people classified in the problem gambling category compared to those classified in the low-risk gambling category.
Interestingly, the prevalence of self-exclusion from gambling estimated in this study is almost identical to the prevalence of help-seeking for gambling (0.26% versus 0.23%) which was reported in our previous global review of gambling prevalence studies [17•]. The relatively low prevalence of self-exclusion may relate to barriers such as potentially complex or embarrassing registration processes [1, 4] or lack of a centralised or online system that would easily allow for multiple and concurrent exclusions [7]. There have been some concerning reports of online gambling operators promoting self-exclusion while the self-exclusion tool was not actually accessible or required self-assessment prior to registration [3], illustrating potential barriers specific to self-exclusion from online services. These findings lend support for a move towards streamlined self-exclusion for all forms of gambling, such as that recently implemented in Sweden [48]. These findings indicate that more needs to be done to increase uptake of harm-minimisation approaches in the gambling field.
In addition to barriers to enrol in self-exclusion programmes, suboptimal utilisation may be attributable to a lack of awareness of self-exclusion. “Responsible gambling” is often promoted in gambling venues and on gambling websites or apps [1, 3]. The findings of the current study suggest a greatly higher prevalence of self-exclusion awareness in people with problem gambling compared to those at lower risk. Although caution is needed when interpreting this finding as it was based on only two studies, awareness of self-exclusion programmes is likely higher among those with more exposure to gambling. This is corroborated by a study among Canadian casino patrons finding that regular patrons were more commonly aware of the casino’s self-exclusion programme than occasional patrons [49].
A global systematic review on gambling prevalence surveys reported that overall, the majority of adults participate in gambling activities [22]. According to the findings of the current review, only slightly more than one in ten adults are aware of self-exclusion programmes, suggesting that promotion of self-exclusion programmes is inadequate, even among those who gamble. “Responsible gambling” information is generally required as part of gambling advertisements but literature indicates that this information is often lacking or presented in an inconspicuous manner [50]. Furthermore, research examining eye-tracking movements revealed that “responsible gambling” messages in gambling advertisements are often ignored [51]. Directing promotion of “responsible gambling” tools to gambling venues, websites, or apps also limits awareness in those who do not gamble frequently. This may hamper uptake as people who develop gambling problems commonly seek advice from friends and family [52] who are unlikely to suggest self-exclusion if they are unaware of self-exclusion programmes. Taken together, these findings further support previous calls for better targeting, more efficient promotion, and broader information dissemination of self-exclusion programmes [1, 7].
There were high levels of heterogeneity in the estimated prevalence of self-exclusion but no consistent patterns were found in factors that may have contributed to variability between studies. Although the findings indicated higher use of self-exclusion in Australasia than in North America, there was no evidence of a significant difference, which may be due to the limited number of studies in the North American region. Prevalence estimates were also largely similar when comparing whether respondents had self-excluded ever in their lifetime or in the past year or whether they had self-excluded from land-based or online gambling operators. The findings of the current review suggest that there are other factors that may be causing this study variability, such as the availability of a centralised self-exclusion system and duration of self-exclusion periods, which greatly differ across jurisdictions [53]. The limited number of gambling prevalence studies reporting sufficient data on use and awareness of self-exclusion programmes to calculate prevalence estimates prevented exploration of study variability in more detail.
Self-exclusion has been promoted as one of the main, albeit most restrictive, industry-led “responsible gambling” tools aimed at reducing gambling harm [54]. Importantly, “responsible gambling” tools are intended to prevent people from progressing to the higher end of the gambling risk spectrum [55]. The current study estimated a self-exclusion prevalence of around 15% in those with problem gambling. However, it also found that self-exclusion was rarely used by those at the lower end of the gambling risk continuum. This is in line with other findings indicating that the majority of people who self-exclude have gambling problems [1, 11••]. Indeed, self-exclusion is primarily used by people who realise they have a problem and are committed to stop gambling [1]. These findings suggest that positioning of self-exclusion as a harm reduction strategy may be inaccurate. Although people may continue to use other forms of gambling [1, 4, 11••], self-exclusion is essentially an abstinence-based approach that is not intended to promote safer or more responsible use of gambling products.
Recognition that people who self-exclude frequently have gambling problems may increase the onus on the industry to improve the effectiveness and accessibility of these programmes. For example, multiple reviews have reported that self-exclusion is generally a useful stimulus control strategy but that, due to inadequate enforcement, about half of excluders breach their self-exclusion orders at least once during the exclusion period [1, 4, 11••]. If self-exclusion is predominantly used by people experiencing gambling problems, then it needs to be clear that the impact of self-exclusion beyond the excluded period is variable, thereby suggesting that ongoing enrolment might be required if gambling is to be avoided over longer periods of time. Furthermore, it appears that short-term exclusions of less than 3 months are not effective in reducing gambling expenditure meaning this too should be communicated to gamblers [5•]. Investigation of breaches, renewal, and duration of self-exclusion contracts were beyond the scope of this study and more research is warranted on these topics.
In partial acknowledgement of the high number of people with gambling problems who exclude, it has been suggested that self-exclusion should be combined with psychological treatment [1]. Estimates indicate that only about one in five people with problem gambling have undertaken action to change their gambling behaviour, including professional services and informal help [17•]. Evidence suggests that people who self-exclude do not want psychological treatment to change gambling behaviour and this is perhaps why they have selected self-exclusion [4]. For instance, a study in which a brief intervention with a counsellor was offered at the start and end of a self-exclusion period showed that only 15% of participants took up the option of professional treatment [56]. Similarly, a study conducted in Canada showed that when self-excluders were offered an intervention programme with motivational and self-management tools, only about one in three participants completed the programme [57]. These findings suggest that it may be beneficial to promote self-exclusion as a self-management tool using a method of stimulus control rather than a psychological treatment.
It should be noted that this study may underestimate the self-exclusion prevalence overall and in those at various levels of gambling risk. In the majority of included studies, the self-exclusion item was only administered to people meeting criteria of past-year gambling participation or scoring above a certain threshold on the PGSI. Self-exclusion is intended to prevent exposure to gambling activities provided by gambling operators specified in the agreement. As such, people who self-exclude might not meet those criteria and would have been excluded from the meta-analysis, potentially leading to lower prevalence estimates. In addition, the estimates in the current study only reflect self-exclusion through a formal agreement. Self-exclusion from internet gambling operators may also be achieved by using blocking software that prevents access to these operators. Including use of blocking tools to self-exclude may increase self-exclusion estimates as illustrated by a survey performed among Canadian panellists who gambled online [58]. In this survey, 5% of respondents had ever asked for their gambling account to be blocked for a few weeks or more, while 8% had ever used a tool to block their access to online gambling. To adequately inform gambling harm reduction policies, there is a need for standardising the instruments and methods used to estimate self-exclusion. Importantly, self-exclusion survey items should be administered to a random selection of the entire study population regardless of current gambling behaviour or problem gambling risk to capture all people who self-exclude. It is recommended that items cover all self-exclusion options offered within a jurisdiction, preferably with sub-items dedicated to self-exclusion from specific gambling operators or types, particularly when there is no centralised system available.
To address concerns about the global expansion of gambling opportunities and with it a rise in gambling harm that will affect most parts of the world [59], the current study aimed to assess the international prevalence of use and awareness of self-exclusion programmes. Our review employed a rigorous systematic search which targeted both scientific and grey literature. Nevertheless, only studies from Australia, Canada, and the USA were represented in the findings, which limits generalisability to other regions in the world. This is in line with two other systematic reviews on gambling behaviour in self-excluders [4, 11, 60, 61], 5–6% in past year gamblers in the UK [62, 63], and 2% overall in Canada [58]). Given the likely rise in population surveys using panels, it is timely to examine the degree to which panels overestimate relevant prevalence rates and traditional approaches like computer-assisted telephone interviews provide an underestimation. In terms of bias towards English language, during our study selection process, a considerable number of studies were reviewed from jurisdictions where English is not the native language, but none was eligible for inclusion in the review, mostly due to insufficient data on self-exclusion. This is further supported by evidence from the African region, where gambling participation is becoming increasingly widespread but [64, 65], to date, limited information is available on gambling harm-reduction and self-exclusion programmes [64].
Apart from the level of global representativeness of the findings, the current review had various other limitations. Importantly, several of the meta-analytic models included a small number of studies, thereby reducing the generalisability of the findings to the wider population. Additionally, survey items in the included studies varied greatly in formulation of the self-exclusion items (e.g. timeframe to which item referred, specification of gambling type, specification of self-exclusion period) and follow-up items (e.g. addressing breaches of agreement, recurrent self-exclusions). As such, the current study was unable to provide more detailed information on systematic differences in self-exclusion uptake related to characteristics of self-exclusion programmes.
Conclusion
Despite self-exclusion being one of the most researched harm-reduction approaches, the current review highlighted the relative limited body of literature reporting representative estimates regarding the uptake and awareness of self-exclusion programmes. Nevertheless, the findings indicate a need to find effective approaches to increase uptake and awareness of self-exclusion. Efforts may in part be dedicated to increasing awareness of self-exclusion in the wider population to facilitate encouragement from peers to register for self-exclusion programmes. Governments should enforce gambling operators to improve clarity and ease of engaging in self-exclusion programmes and thereby remove common barriers to registration. Moreover, future research should employ standardised methods of assessing self-exclusion uptake to enable an accurate comparison of prevalence estimates by population subgroups.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
- Gainsbury SM. Review of self-exclusion from gambling venues as an intervention for problem gambling. J Gambl Stud. 2014;30(2):229–51.
Article PubMed Google Scholar - Ladouceur R, Shaffer P, Blaszczynski A, Shaffer HJ. Responsible gambling: a synthesis of the empirical evidence. Addict Res Theory. 2017;25(3):225–35.
Article Google Scholar - Catania M, Griffiths MD. Analyzing consumer protection for gamblers across different online gambling operators: a replication study. Int J Ment Health Addict, 2021:1–16. https://doi.org/10.1007/s11469-021-00695-9.
- Motka F, et al. Who uses self-exclusion to regulate problem gambling? A systematic literature review. J Behav Addict. 2018;7(4):903–16.
Article PubMed PubMed Central Google Scholar - • Rodda SN. A systematic review of internet delivered interventions for gambling: prevention, harm reduction and early intervention. J Gambl Stud. 2021;38(3):967–91. https://doi.org/10.1007/s10899-021-10070-x. Systematic review of 15 studies reporting on internet-delivered interventions for prevention, harm reduction, and early intervention for gambling. Twenty percent of studies focused on internet-delivered self-exclusion.
Article PubMed Google Scholar - • Håkansson A, Henzel V. Who chooses to enroll in a new national gambling self-exclusion system? A general population survey in Sweden. Harm Reduct J. 2020;17(1):82. https://doi.org/10.1186/s12954-020-00423-x. Panel survey of 1940 people in Sweden sought to determine the characteristics of those who used a national multi-venue online and land-based self-exclusion programme.
Article PubMed PubMed Central Google Scholar - Hing N, Nuske E. The self-exclusion experience for problem gamblers in South Australia. Aust Soc Work. 2012;65(4):457–73.
Article Google Scholar - Pickering D, Blaszczynski A. Should I stay or should I go? A comparative exploratory analysis of individuals electing to continue or discontinue self-exclusion from land-based gambling venues. Int J Ment Heal Addict. 2022;20(2):1182–99.
Article Google Scholar - •• McMahon N, Thomson K, Kaner E, Bambra C. Effects of prevention and harm reduction interventions on gambling behaviours and gambling related harm: an umbrella review. Addict Behav. 2019;90:380–8. https://doi.org/10.1016/j.addbeh.2018.11.048. Umbrella review of harrm reduction interventions and their impact on gambling harm. Discusses two reviews which identified 11 unique studies on the effects of self-exclusion programmes.
Article PubMed Google Scholar - Drawson AS, Tanner J, Mushquash CJ, Mushquash AR, Mazmanian D. The use of protective behavioural strategies in gambling: a systematic review. Int J Ment Heal Addict. 2017;15(6):1302–19.
Article Google Scholar - •• Kotter R, Kräplin A, Pittig A, Bühringer G. A systematic review of land-based self-exclusion programs: demographics, gambling behavior, gambling problems, mental symptoms, and mental health. J Gambl Stud. 2019;35(2):367–94. https://doi.org/10.1007/s10899-018-9777-8. Systematic review of 19 studies reporting on self-exclusion programmes. Provides a summary demographic characteristics of self-excluders and outcomes related to self-exclusion.
Article PubMed Google Scholar - Abbott MW. The changing epidemiology of gambling disorder and gambling-related harm: public health implications. Public Health. 2020;184:41–5. https://doi.org/10.1016/j.puhe.2020.04.003.
Article CAS PubMed Google Scholar - Gainsbury SM. Online gambling addiction: the relationship between internet gambling and disordered gambling. Curr Addict Rep. 2015;2(2):185–93. https://doi.org/10.1007/s40429-015-0057-8.
Article PubMed PubMed Central Google Scholar - Lawn S, Oster C, Riley B, Smith D, Baigent M, Rahamathulla M. A literature review and gap analysis of emerging technologies and new trends in gambling. Int J Environ Res Public Health, 2020;17(3). https://doi.org/10.3390/ijerph17030744.
- Bjorseth B, et al. The effects of responsible gambling pop-up messages on gambling behaviors and cognitions: a systematic review and meta-analysis. Front Psychiatry. 2020;11:601800. https://doi.org/10.3389/fpsyt.2020.601800.
Article PubMed Google Scholar - Gainsbury SM, Abarbanel BLL, Philander KS, Butler JV. Strategies to customize responsible gambling messages: a review and focus group study. BMC Public Health. 2018;18(1):1381. https://doi.org/10.1186/s12889-018-6281-0.
Article PubMed PubMed Central Google Scholar - • Bijker R, Booth N, Merkouris SS, Dowling NA, Rodda SN. Global prevalence of help-seeking for problem gambling: a systematic review and meta-analysis. Addiction. 2022;117(12):2972–85. https://doi.org/10.1111/add.15952. Systematic review and meta-analysis of 24 gambling prevalence studies. Provides global estimates on help-seeking for problem gambling.
Article PubMed PubMed Central Google Scholar - Page MJ, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org/10.1136/bmj.n71.
Article PubMed PubMed Central Google Scholar - Brooke BS, Schwartz TA, Pawlik TM. Moose reporting guidelines for meta-analyses of observational studies. JAMA Surg. 2021;156(8):787–8. https://doi.org/10.1001/jamasurg.2021.0522.
Article PubMed Google Scholar - Sturgis P, Kuha J. How survey mode affects estimates of the prevalence of gambling harm: a multisurvey study. Public Health. 2022;204:63–9. https://doi.org/10.1016/j.puhe.2021.12.014.
Article CAS PubMed Google Scholar - Williams RJ, Volberg RA, Stevens RMG. The population prevalence of problem gambling: methodological influences, standardized rates, jurisdictional differences, and worldwide trends. Guelph, ON: Ontario Problem Gambling Research Centre; 2012.
- Calado F, Griffiths MD. Problem gambling worldwide: an update and systematic review of empirical research (2000–2015). J Behav Addict. 2016;5(4):592–613. https://doi.org/10.1556/2006.5.2016.073.
Article PubMed PubMed Central Google Scholar - Hoy D, et al. Assessing risk of bias in prevalence studies: modification of an existing tool and evidence of interrater agreement. J Clin Epidemiol. 2012;65(9):934–9. https://doi.org/10.1016/j.jclinepi.2011.11.014.
Article PubMed Google Scholar - Viechtbauer W. Conducting meta-analyses in R with the metafor package. J Stat Softw, 2010;36(3):1–48. https://doi.org/10.18637/jss.v036.i03.
- R Core Team. R: a language and environment for statistical computing. Vienna, AT: R Foundation for Statistical Computing. 2021.
- Stijnen T, Hamza TH, Ozdemir P. Random effects meta-analysis of event outcome in the framework of the generalized linear mixed model with applications in sparse data. Stat Med. 2010;29(29):3046–67.
Article PubMed Google Scholar - Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analysis. BMJ. 2003;327(7414):557–60.
Article PubMed PubMed Central Google Scholar - Ryan R, Hill S. Cochrane consumers and communication review group: meta-analysis. Melbourne, AU: La Trobe University. 2016. https://doi.org/10.26181/5b57d2b96b326.
- Hunter J, et al. In meta-analyses of proportion studies, funnel plots were found to be an inaccurate method of assessing publication bias. J Clin Epidemiol. 2014;67:897–903. https://doi.org/10.1016/j.jclinepi.2014.03.003.
Article PubMed Google Scholar - Duval S, Tweedie R. Trim and fill: a simple funnel plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000;56:455–63.
Article CAS PubMed Google Scholar - Mavridis D, Salanti G. How to assess publication bias: funnel plot, trim-and-fill method and selection models. Evid-Based Ment Health. 2014;17(1):30.
Article PubMed Google Scholar - Ferris JA, Wynne HJ. The Canadian problem gambling index. 2001. Ottawa, ON: Canadian Centre on substance abuse.
- ACIL Allen Consulting, Deakin University, Central Queensland University, Social Research Centre. Fourth social and economic impact study of gambling in tasmania: report 2. 2017. Hobart, AU: Tasmanian Department of Treasury and Finance. https://acilallen.com.au/uploads/projects/159/ACILAllen_FourthTasGambling_Vol2_2017-1581307240.pdf. Accessed 30 Jun 2022.
- Browne M, Rockloff M, Hing N, Russell A, Boyle CM, Rawat V. NSW Gambling survey 2019. Bundaberg, AU: Central Queensland University. 2019. https://www.responsiblegambling.nsw.gov.au/__data/assets/pdf_file/0008/881279/NSW-Gambling-Survey-2019-report-FINAL-AMENDED-Mar-2020.pdf. Accessed 5 Aug 2022.
- Davidson T, Rodgers B, Taylor-Rodgers E, Sumoi A, Lucas N. 2014 Survey on gambling, health and wellbeing in the ACT: final report. Canberra, AU: Australian National University. 2015. https://www.gamblingandracing.act.gov.au/__data/assets/pdf_file/0010/846901/2014-Survey-on-Gambling,-Health-and-Wellbeing-in-the-ACT-.pdf. Accessed 30 Jun 2022.
- Department of Justice and Attorney-General, State of Queensland. Queensland household gambling survey 2011-2012. Brisbane, AU: Department of Justice and Attorney-General. 2012. https://www.publications.qld.gov.au/dataset/liquor-and-gambling-research/resource/79c83075-5dd6-48f7-84b1-8bd6b106eaff. Accessed 5 Aug 2022.
- Department of Justice and Attorney-General, State of Queensland. Queensland household gambling survey 2016-17. Brisbane, AU: Department of Justice and Attorney-General. 2018. https://www.publications.qld.gov.au/dataset/liquor-and-gambling-research/resource/4267f3c2-950b-407e-b88f-d31e116cedcb. Accessed 24 Aug 2022.
- Hing N, Gainsbury S, Blaszczynski A, Wood R, Lubman D, Russel A. Interactive gambling. Melbourne, AU: Victoria office of liquor, gaming and racing. commissioned by gambling research Australia. 2014. https://www.gamblingresearch.org.au/sites/default/files/2019-10/Interactive%20Gambling%202014.pdf. Accessed 29 Aug 2023.
- O’Neil M, et al. Fifth social and economic impact study of gambling in Tasmania 2021. Volume 2: 2020 Prevalence survey report. Adelaide, Au: South Australian Centre for Economic Studies, University of Adelaide. 2021. https://www.treasury.tas.gov.au/Documents/Fifth%20SEIS%20Volume%202%20-%20Prevalence%20Survey.PDF. Accessed 3 Aug 2022.
- Park K, Losch M, Muilenburg R, Zubrod A. Gambling attitudes and behaviors: a 2018 survey of adult Iowans. Attitudes and opinions. Cedar Falls, IA: Center for Social Behavioral Research, University of Northern Iowa. 2019. https://idph.iowa.gov/igtp/reports. Accessed 12 Aug 2022.
- Paterson M, Leslie P, Taylor M. 2019 Act gambling survey. Canberra, AU: centre for gambling research, The Australian National University. 2019. https://csrm.cass.anu.edu.au/sites/default/files/docs/2019/10/2019-ACT-Gambling-Survey.pdf. Accessed 5 Aug 2022.
- Social Research Centre. Gambling prevalence in South Australia. Adelaide, AU: South Australian Department for Communities and Social Inclusion, Office for Problem Gambling. 2013. https://problemgambling.sa.gov.au/__data/assets/pdf_file/0007/80368/sa-gambling-prevalence-study-report-2012.pdf. Accessed 3 Aug 2022.
- Sproston K, Hing N, Palankay C. Prevalence of gambling and problem gambling in New South Wales. Bundaberg, AU: Central Queensland University. 2012. https://www.gambleaware.nsw.gov.au/-/media/files/published-research-pdfs/prevalence-of-gambling-and-problem-gambling-in-nsw.ashx?rev=a09cb2e9d3b04b1db45f3de149fc86e8&hash=CE20E2AE8FB5E22DA79CD27D8FAD6D9B. Accessed 3 Aug 2022.
- Stevens M, Gupta M, Flack M. Northern Territory gambling prevalence and wellbeing survey report, 2018. Darwin, AU: NT Government Department of Industry, Tourism and Trade. 2019. https://industry.nt.gov.au/__data/assets/pdf_file/0010/959176/2018-nt-gambling-prevalence-wellbeing-survey.pdf. Accessed 5 Aug 2022
- Williams RJ, Volberg RA. Gambling and problem gambling in Ontario. Ontario, CA: Ontario Problem Gambling Research Centre and the Ontario Ministry of Health and Long Term Care. 2013. https://www.researchgate.net/publication/328107604_Gambling_and_problem_gambling_in_Ontario. Accesed 30 Jun 2022.
- Williams R, Pekrow P, Volberg R, Stanek E, Zorn M, Houpt A. Impacts of gambling in Massachusetts: results of a baseline online panel survey (BOPS). Amherst, MA: School of Public Health and Health Sciences, University of Massachusetts Amherst. 2017. https://massgaming.com/wp-content/uploads/Impacts-of-Gambling-in-Massachusetts-Results-of-a-Baseline-Online-Panel-Survey-BOPS_1.10.2017_Report.pdf. Accessed 5 Aug 2022.
- Woods A, Sproston K, Brook K, Delfabbro P, O’Neil M. Gambling prevalence in South Australi (2018): final report. Adelaide, AU: Department of Human Services, South Australia. 2018. https://problemgambling.sa.gov.au/__data/assets/pdf_file/0017/80126/2018-SA-Gambling-Prevalence-Survey-Final-Report-Updated-07.02.19.pdf. Accessed 3 Aug 2022
- Hakansson A, Widinghoff C. Gambling despite nationwide self-exclusion-a survey in online gamblers in Sweden. Front Psychiatry. 2020;11:599967. https://doi.org/10.3389/fpsyt.2020.599967.
Article PubMed PubMed Central Google Scholar - Christensen DR, et al. Responsible gambling in Canada: an analysis of the RG Check patron surveys. J Gambl Stud. 2022;38(3):905–15. https://doi.org/10.1007/s10899-021-10052-z.
Article PubMed Google Scholar - Torrance J, et al. Emergent gambling advertising; a rapid review of marketing content, delivery and structural features. BMC Public Health. 2021;21(1):718. https://doi.org/10.1186/s12889-021-10805-w.
Article PubMed PubMed Central Google Scholar - Lole L, et al. Are sports bettors looking at responsible gambling messages? An eye-tracking study on wagering advertisements. J Behav Addict. 2019;8(3):499–507. https://doi.org/10.1556/2006.8.2019.37.
Article PubMed PubMed Central Google Scholar - Rodda SN, Dowling NA, Lubman DI. Gamblers seeking online help are active help-seekers: time to support autonomy and competence. Addict Behav. 2018;87:272–5. https://doi.org/10.1016/j.addbeh.2018.06.001.
Article CAS PubMed Google Scholar - Kraus L, et al. Self-exclusion from gambling: a toothless tiger? Front Psychiatry. 2022;13:992309. https://doi.org/10.3389/fpsyt.2022.992309.
Article PubMed PubMed Central Google Scholar - Livingstone C, Rintoul A, Francis L. What is the evidence for harm minimisation measures in gambling venues. Evid Base. 2014;2:1–24.
Google Scholar - Blaszczynski A, Ladouceur R, Shaffer HJ. A science-based framework for responsible gambling: the Reno model. J Gambl Stud. 2004;20(3):301–17.
Article PubMed Google Scholar - Tremblay N, Boutin C, Ladouceur R. Improved self-exclusion program: preliminary results. J Gambl Stud. 2008;24(4):505–18. https://doi.org/10.1007/s10899-008-9110-z.
Article PubMed Google Scholar - Yakovenko I, Hodgins DC. Effectiveness of a voluntary casino self-exclusion online self-management program. Internet Interv. 2021;23:100354. https://doi.org/10.1016/j.invent.2020.100354.
Article PubMed Google Scholar - Ipsos. British Columbia online problem gambling prevalence study 2020. https://www2.gov.bc.ca/assets/gov/sports-recreation-arts-and-culture/gambling/gambling-in-bc/reports/bc_online_problem_gambling_prevalence_report_2020.pdf.
- Wardle H, Degenhardt L, Ceschia A, Saxena S. The Lancet public health commission on gambling. Lancet Public Health. 2021;6(1):e2–3. https://doi.org/10.1016/S2468-2667(20)30289-9.
Article PubMed Google Scholar - Hakansson A. Changes in gambling behavior during the COVID-19 pandemic-a web survey study in Sweden. Int J Environ Res Public Health, 2020;17(11):4013. https://doi.org/10.3390/ijerph17114013.
- Hakansson A, Widinghoff C. Changes of gambling patterns during COVID-19 in Sweden, and potential for preventive policy changes. A second look nine months into the pandemic. Int J Environ Res Public Health, 2021;18(5):2342. https://doi.org/10.3390/ijerph18052342.
- Gambling Commission. Gambling participation in 2018: behaviour, awareness and attitudes. 2019. https://cliftondavies.com/wp-content/uploads/2019/02/GC-Gambling-participation-in-2018-behaviour-awareness-attitudes-Annual-Report-.pdf.
- Gambling Commission. Gambling participation in 2019: behaviour, awareness and attitudes: annual report. 2020. https://assets.ctfassets.net/j16ev64qyf6l/7uIxjm1SNQMygdOFV2bzxN/ea74db1104925f015edb11db0596f98b/Gambling-participation-in-2019-behaviour-awareness-and-attitudes.pdf.
- Sichali JM, et al. Regulation of gambling in sub-saharan africa: findings from a comparative policy analysis. Public Health. 2023;214:140–5. https://doi.org/10.1016/j.puhe.2022.07.018.
Article CAS PubMed Google Scholar - Bitanihirwe BKY, et al. Gambling in sub-Saharan Africa: traditional forms and emerging technologies. Curr Addict Rep. 2022;9(4):373–84. https://doi.org/10.1007/s40429-022-00449-0.
Article PubMed PubMed Central Google Scholar