Is HIV-1 evolving to a less virulent form in humans? (original) (raw)
Abstract
During the rapid spread of HIV-1 in humans, the main (M) group of HIV-1 has evolved into ten distinct subtypes, undergone countless recombination events and diversified extensively. The impact of this extreme genetic diversity on the phenotype of HIV-1 has only recently become a research focus, but early findings indicate that the dominance of HIV-1 subtype C in the current epidemic might be related to the lower virulence of this subtype compared with other subtypes. Here, we explore whether HIV-1 has reached peak virulence or has already started the slow path to attenuation.
Similar content being viewed by others
Main
There are four classified retroviruses that infect humans and cause symptomatic disease. Human T-cell lymphotropic virus (HTLV) types 1 and 2 are members of the Deltaretrovirus genus in the subfamily Orthoretrovirinae, show a low rate of evolution in the human population, and probably originated from a non-human primate millions of years ago1,2,3,4. The high frequency of HTLV-1 infections was localized in specific endemic areas (for example, southern Japan) until recent times, indicating a relatively slow spread in the human population compared with another human retrovirus, HIV-1.
HIV-1 was introduced into the human population just 60–80 years ago5 but an estimated 40 million individuals are currently infected with the virus[6](/articles/nrmicro1594#ref-CR6 "UNAIDS/WHO. AIDS Epidemic Update 2006. [online]
, (UNAIDS/WHO, Geneva, 2006)."). The spread and expansion of HIV-1 across Africa and throughout the world has been accompanied by one of the most rapid evolutionary rates described for a human pathogen[6](/articles/nrmicro1594#ref-CR6 "UNAIDS/WHO. AIDS Epidemic Update 2006.
[online]
, (UNAIDS/WHO, Geneva, 2006)."), aside from hepatitis C virus. HIV-1 remains one of the most lethal pathogens (100% mortality) that currently infects humans, whereas infection by other human viruses that are often more feared, such as Ebola, severe acute respiratory syndrome (SARS), influenza H5NI and Lassa Fever, can have a mortality rate of <50% (Refs [7–9](/articles/nrmicro1594#ref-CR7 "Geisbert, T. W. & Jahrling, P. B. Exotic emerging viral diseases: progress and challenges. Nature Med. 10, S110–S121 (2004).")).Whether or not a lethal pathogen evolves to become a relatively benign parasite or even a commensal organism has been a subject of great debate. The survival of Euroasian populations during the European bubonic plague (1347–1352) and the 1918 influenza epidemic is often perceived as evidence for pathogen attenuation. However, neither Yersinia pestis nor the H1N1 influenza virus seem to have attenuated during these relatively short human epidemics. Surviving the Y. pestis epidemic is thought to be more related to fractionation of the human population, the resistance of rodent ectoparasites and, possibly, the selection of resistant human hosts10,11.
Nonetheless, there are many examples of microparasite evolution and host selection leading to attenuation or resistance to disease. The best documented and controlled example is the rapid outgrowth of an attenuated myxoma virus following its introduction into Australia in 1950 to control the expanding rabbit population12,13,14. This virus might have attenuated as a result of altered immunomodulatory properties in addition to a reduction in the replication rate13,14. More recent analyses of archived reports from the fifteenth century suggest that the dramatic decrease in the severity of syphilis symptoms that took place over a period of less than 10 years was related to a reduction in virulence rather than the selection of resistant hosts15. Rapid (decades to centuries) versus slow (thousand to millions of years) attenuation might be related to the severity of disease, the rate of lethality and the transmission efficiency or transmission routes. The suggestion that the simian lentiviruses have attenuated in their non-human primate hosts during millions of years of co-evolution16 has been challenged by recent phylogenetic analyses that indicate the introduction of simian immunodeficiency virus (SIV) into African primates might be a relatively recent event that unfolded in the past hundreds or thousands of years, therefore indicating that primate lentiviruses might frequently jump between primate species and then rapidly adapt to the new host17,18.
Studies that have modelled the expansion and contraction of various epidemics have indicated that the inter-relationships between lethal pathogens and their hosts are complex and frequently not comparable19,20,21,22. These questions can only be answered by understanding pathogen evolution, dynamics and spread within the population at large and within infected hosts. The propensity for HIV-1 to evolve rapidly in response to various immune and other host pressures indicates that this virus is more likely to become attenuated through a reduction of virulence rather than selection of resistant hosts.
Defining pathogen fitness and virulence
The phylogenetic approaches that are commonly used to describe the evolution of pathogens do not examine how these genetic differences actually impact on the physical attributes, often termed the fitness, of the pathogen. This is understandable, given the complexities of measuring fitness, which can be defined as the adaptability or reproductive success of an organism in a specific environment. In the case of HIV-1 research, fitness is frequently misrepresented or over-interpreted23,[24](/articles/nrmicro1594#ref-CR24 "Quinones-Mateu, M. E. & Arts, E. J. HIV-1 Fitness: Implications for Drug Resistance, Disease Progression, and Global Epidemic Evolution. [online]
, (HIV Sequence Compendium, Theoretical Biology and Biophysics Group, Los Alamos National Laboratory, Los Alamos, 2001)."). For example, HIV-1 virions in which the reverse transcriptase (RT) harbours mutations that confer resistance to antiretroviral drugs (ARVs) such as 3TC (Lamivudine or Epivir) seem less fit than virions carrying the wild-type RT[25](/articles/nrmicro1594#ref-CR25 "Feng, J. Y. & Anderson, K. S. Mechanistic studies examining the efficiency and fidelity of DNA synthesis by the 3TC-resistant mutant (184V) of HIV-1 reverse transcriptase. Biochemistry 38, 9440–9448 (1999)."),[26](/articles/nrmicro1594#ref-CR26 "Deval, J. et al. Mechanistic basis for reduced viral and enzymatic fitness of HIV-1 reverse transcriptase containing both K65R and M184V mutations. J. Biol. Chem. 279, 509–516 (2004)."). However, this reduced fitness in a reconstituted _in vitro_ assay does not necessarily imply that the drug-resistant virus will be less fit in a human host receiving ARVs. Fitness in each environment can be inter-related but is not necessarily consequential. For the purposes of this Opinion article, HIV-1 fitness will be defined in a specific environment and only significant correlations between environments will be highlighted as being potentially consequential.Fitness is not always synonymous with virulence, which is typically defined as the rate of host mortality as a consequence of infection27 but which can be further refined to include the reproduction rate and pathogenic potential of the pathogen28. These parameters also define the fitness of a pathogen within a host. Typically, virulence is difficult to measure for viruses such as HIV-1, given the long asymptomatic period after infection. Therefore, intermittent measures of HIV-1 replicative fitness during disease can often provide insights into the rates of disease progression29,30,31,32. Confusion between these principles of virulence and fitness is introduced when examining fitness within the host compared with examining fitness within a population[24](/articles/nrmicro1594#ref-CR24 "Quinones-Mateu, M. E. & Arts, E. J. HIV-1 Fitness: Implications for Drug Resistance, Disease Progression, and Global Epidemic Evolution. [online]
, (HIV Sequence Compendium, Theoretical Biology and Biophysics Group, Los Alamos National Laboratory, Los Alamos, 2001)."),[33](/articles/nrmicro1594#ref-CR33 "Ewald, P. W. Evolution of Infectious Disease (Oxford University Press, Oxford, 1994)."). Maynard, Ewald, Anderson, May, Novak and others[22](/articles/nrmicro1594#ref-CR22 "Anderson, R. M. & May, R. M. Infectious Diseases of Humans: Dynamics and Control (Oxford University Press, Oxford, 1991)."),[33](/articles/nrmicro1594#ref-CR33 "Ewald, P. W. Evolution of Infectious Disease (Oxford University Press, Oxford, 1994)."),[34](/articles/nrmicro1594#ref-CR34 "Nowak, M. A. & May, R. M. Virus Dynamics: Mathematical Principles of Immunology and Virology (Oxford University Press, Oxford, 2000)."),[35](/articles/nrmicro1594#ref-CR35 "Maynard, S. J. Group selection and kin selection. Nature 201, 1145–1147 (1964)."),[36](/articles/nrmicro1594#ref-CR36 "Szathmary, E. & Maynard, S. J. From replicators to reproducers: the first major transitions leading to life. J. Theor. Biol. 187, 555–571 (1997).") suggest that pathogen strain 'A', with slow replicative fitness but high transmission efficiency, will be favoured in a host population over strain 'B', with increased replicative fitness. However, when the strains compete together in a single host, it is clear that strain 'B' is more virulent and would out-compete and, consequently, be fitter than, strain 'A'. In terms of a pathogen spreading through a host population, high pathogen fitness is then defined by a reduction in reproduction rate and virulence without a loss in transmission. This article will address the possible direct relationship between HIV-1 virulence and replicative fitness but it is important to note that attenuation of virulence is not always synonymous with lower replicative capacity. For example, the attenuation of myxoma virulence in the Australian rabbit population might be more related to changes in virus-mediated immunomodulation than to lower replicative fitness in rabbits[13](/articles/nrmicro1594#ref-CR13 "Zuniga, M. C. A pox on thee! Manipulation of the host immune system by myxoma virus and implications for viral–host co-adaptation. Virus Res. 88, 17–33 (2002)."),[14](/articles/nrmicro1594#ref-CR14 "Best, S. M. & Kerr, P. J. Coevolution of host and virus: the pathogenesis of virulent and attenuated strains of myxoma virus in resistant and susceptible European rabbits. Virology 267, 36–48 (2000).").Expansion of HIV-1 in humans
HIV-1 was first introduced into the human population from the chimpanzee subspecies Pan troglodytes troglodytes37,38,39. Most recently, Keele et al. have discovered a region in southern Cameroon where chimpanzees carry SIV strains (SIVcpzptt) that are closely related to two distinct lineages of HIV-1, the main (M) and new (N) groups37 (Fig. 1). The origin of the outlier (O) group might be related to a jump from Gorilla gorilla40. SIVcpzptt was introduced into the human population multiple times, over decades to possibly centuries, but these transfer events probably started to increase in the 1920s to the 1950s as a result of human migration into this dense tropical region5,37,38,39. Similar to the pending introduction of influenza H5N1 from the avian to the human host41, a distinct but possibly rare SIVcpzptt strain might have had the capacity for efficient replication and sexual transmission in humans17,37. Following this founder event, human population density and contact had to be sufficiently high for subsequent transmission and spread. It is possible that a single transmission of HIV-1 group M spawned the >60–80 million infections that have taken place since the beginning of the epidemic37. By contrast, HIV-2 originated in humans from a cross-species transmission from sooty mangabeys in west Africa (near or in Guinea-Bissau) around 1930–1955 (Refs 42, 43). In the 1980s, the incidence of HIV-1 group M in central Africa and HIV-2 in west Africa expanded exponentially but clearly at different rates, as the prevalence of HIV-1 M infections (28 million) far exceeds that of HIV-2 infections (<1 million)[6](/articles/nrmicro1594#ref-CR6 "UNAIDS/WHO. AIDS Epidemic Update 2006. [online]
, (UNAIDS/WHO, Geneva, 2006)."),[44](/articles/nrmicro1594#ref-CR44 "Schim van der Loeff, M. F. & Aaby, P. Towards a better understanding of the epidemiology of HIV-2. AIDS 13, S69–S84 (1999)."),[45](/articles/nrmicro1594#ref-CR45 "Schim van der Loeff, M. F. et al. Sixteen years of HIV surveillance in a West African research clinic reveals divergent epidemic trends of HIV-1 and HIV-2. Int. J. Epidemiol. 35, 1322–1328 (2006)."). In stark contrast, HIV-1 groups O and N are responsible for <25,000 infections, most of which are in Cameroon and Gabon[6](/articles/nrmicro1594#ref-CR6 "UNAIDS/WHO. AIDS Epidemic Update 2006.
[online]
, (UNAIDS/WHO, Geneva, 2006)."),[46](/articles/nrmicro1594#ref-CR46 "Ayouba, A. et al. HIV-1 group O infection in Cameroon, 1986 to 1998. Emerg. Infect. Dis. 7, 466–467 (2001)."),[47](/articles/nrmicro1594#ref-CR47 "Yamaguchi, J. et al. HIV infections in northwestern Cameroon: identification of HIV type 1 group O and dual HIV type 1 group M and group O infections. AIDS Res. Hum. Retroviruses 20, 944–957 (2004)."),[48](/articles/nrmicro1594#ref-CR48 "Yamaguchi, J. et al. HIV-1 Group N: evidence of ongoing transmission in Cameroon. AIDS Res. Hum. Retroviruses 22, 453–457 (2006)."),[49](/articles/nrmicro1594#ref-CR49 "Yamaguchi, J. et al. Identification of HIV type 1 group N infections in a husband and wife in Cameroon: viral genome sequences provide evidence for horizontal transmission. AIDS Res. Hum. Retroviruses 22, 83–92 (2006)."). The expansion and divergent evolution of HIV-1 group M into diverse subtypes ([Fig. 1](/articles/nrmicro1594#Fig1)) has been dated to 1956–1976 and might have coincided with human emigration and the seeding of new regional epidemics in central Africa[5](/articles/nrmicro1594#ref-CR5 "Korber, B. et al. Timing the ancestor of the HIV-1 pandemic strains. Science 288, 1789–1796 (2000)."),[50](/articles/nrmicro1594#ref-CR50 "Salemi, M. et al. Dating the common ancestor of SIVcpz and HIV-1 group M and the origin of HIV-1 subtypes using a new method to uncover clock-like molecular evolution. FASEB J. 15, 276–278 (2001)."),[51](/articles/nrmicro1594#ref-CR51 "Travers, S. A. et al. Timing and reconstruction of the most recent common ancestor of the subtype C clade of human immunodeficiency virus type 1. J. Virol. 78, 10501–10506 (2004).").Figure 1: Phylogenetic tree of human and simian lentiviruses.
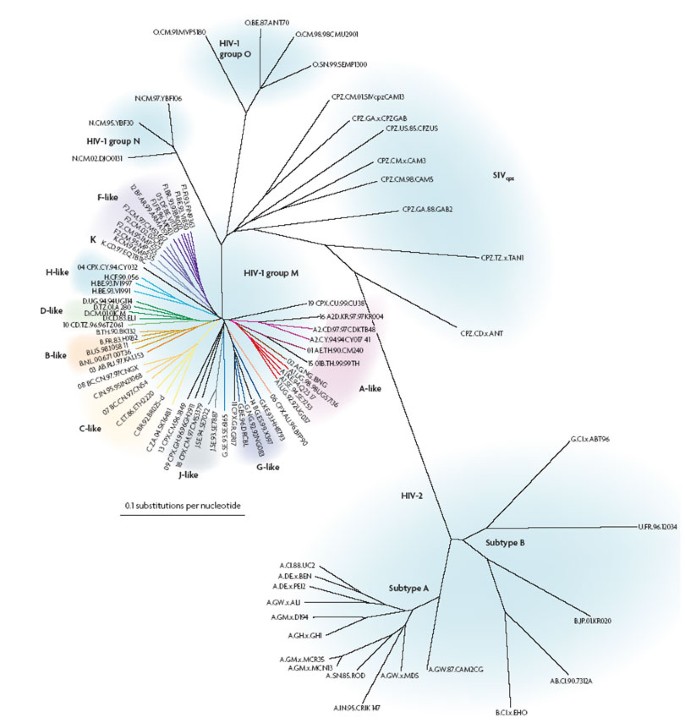
The genetic similarity between different HIV and simian immunodeficiency virus (SIV) strains was compared by aligning the full genome sequences of 87 human and simian lentiviruses using ClustalX v.1.83 (the accession numbers are available on request). Phylogenetic trees based on nucleotide distance were constructed by neighbour-joining methods as implemented in ClustalX with 1,000 bootstrap resamplings (not presented) and schematically represented with the TreeView program. HIV-2 and HIV-1 share only 50–60% sequence identity and cluster at distinct locations on the phylogenetic tree whereas SIVcpz branches out from the root of the HIV-1 groups. The origins of these HIV-1 groups in southern Cameroon have recently been described and indicate two probable jumps from chimpanzee (groups M and N) and gorilla (group O) species. HIV-1 M subtypes probably evolved from a discrete introduction into the human population and then diverged into different subtypes. The subtypes defined as 'A-like' describe HIV-1 isolates with sequences that map phylogenetically more to subtype A than to any other subtype. For example, the recombinant form CRF02_AG (such as 02 AG.NG.IBNG in the HIV-1 group M A-like cluster) has longer genomic segments that are more related to subtype A than to subtype G. M, main; N, new.
HIV-1 subtypes share 70–90% sequence identity, groups share <70%, and HIV-1 and HIV-2 can differ as much as 50% at the nucleotide level (Fig. 1). Given this extreme genetic diversity, is it reasonable to assume that not all HIV types, groups, subtypes and even isolates have evolved to maintain similar virulence? Although many research articles have described genotypic differences between subtypes, there are only a handful of studies that have examined potential phenotypic differences among the human lentiviruses52,53,54,55,56. No studies have modelled how phenotypic or 'fitness' differences among these viruses might affect disease progression in infected individuals or the general spread of the virus in the human population. This article can only provide predictions of temporal HIV-1 attenuation based on published studies and significant trends during the human epidemic. To understand how attenuation of virulence can occur, it is important to understand the population dynamics and fitness of HIV-1 in each infected host and during host-to-host transmission.
How HIV-1 infects, and evolves in, a host
In relation to other sexually transmitted pathogens, HIV-1 is transmitted with moderate efficiency by sexual contact and apparently greater efficiency by direct blood-to-blood contact (for example, needle sharing by intravenous drug users)57,58 or vertical mother-to-child perinatal transmission59. There are many cases of discordant couples in which the HIV-positive individual fails to transmit the virus to the uninfected partner despite frequent opportunity60. A schematic of transmission events and disease progression is provided in Fig. 2 and Box 1. An increased viral load in the donor and consequently in the inoculating dose increases the transmission efficiency61,62. An increased viral load in the donor also corresponds to greater genetic diversity of the inoculating HIV-1 population (termed the virus isolate)63 (Fig. 2), and yet few HIV-1 clones will establish an infection in the recipient64. This dramatic bottleneck might be related to accessing the initial target cells (cells of the dendritic lineage)65,66 and establishing a productive, systemic infection. Based on extensive studies on RNA viruses, it is clear that restrictive genetic bottlenecks invoked by various selection pressures will reduce replicative fitness67,68,69. Unfortunately, nearly all of these viral fitness studies have been done in tissue-culture infections and not in animal models or in defined donor–recipient transmission pairs. Greater HIV-1 genetic diversity during acute or early infection has been associated with more rapid disease progression70. In addition, the genetic diversity of HIV-1 seems to correlate directly with replicative fitness29.
Figure 2: A hypothetical example of changes in replicative fitness and viral load during HIV-1 disease progression.
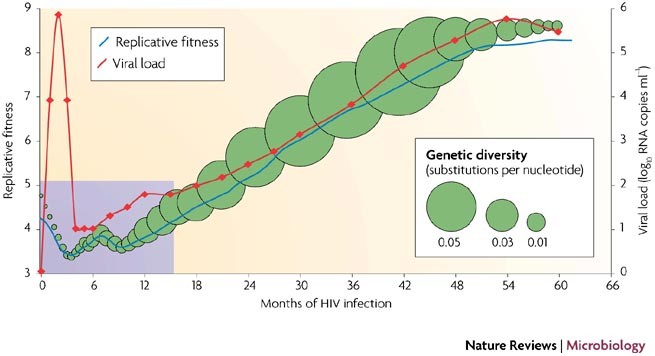
An individual is typically infected by a few HIV-1 clones (depicted by a small green circle), which dramatically increase in copy number but not in genetic diversity during the first 1–2 months of infection. Following this acute infection period, viral load is reduced partly as a result of strong HIV-specific cell-mediated immunity. The virus population is thought to oscillate between expansion of HIV-1 populations owing to immune escape from existing HIV-specific cytotoxic T-lymphocyte (CTL) clones and contraction caused by new genetic bottlenecks that are induced by newly emerging CTL clones. The replicative fitness and genetic diversity of the HIV-1 population seem to track closely together and, following early disease (purple box), both increase at a relatively linear rate with the length of infection. This increase in replicative fitness correlates with increases in viral loads (right axis) and decreases in CD4+ T-cell counts (not shown). The scale for replicative fitness is arbitrary but is derived from the relative HIV-1 fitness values, that is, the ability of one HIV-1 isolate to out-compete another in ex vivo dual-virus competition experiments.
HIV is the obvious aetiological agent of AIDS, yet it is commonly assumed that the phenotypic characteristics and replication efficiency (the ex vivo fitness) of the infecting, wild-type HIV isolates have little impact on the rate of disease progression. Much attention has been focused on host correlates of disease progression, such as the strength of HIV-specific immune responses71,72,73,74,75,76,77 and host genetic polymorphisms that might affect HIV-1 replication78,79,80,81,82. RNA load remains the best predictor of HIV disease progression83 and the dramatic reductions in this load achieved by ARV treatment can delay disease progression84. It is important to note that a high viral load is not an absolute in relation to the severity of the disease. In non-human hosts such as sooty mangabeys, a high SIV load is not associated with clinical symptoms85. Recent studies indicate that the decline in CD4+ T-cell counts, and not the increase in viral load, is a better predictor of disease progression86.
The first evidence that specific viral genetic traits might affect virulence was the identification of long-term non-progressing individuals harbouring a defective HIV-1 isolate lacking a nef open reading frame87,88. Mutations or deletions in this accessory-protein-coding gene can significantly impair fitness in tissue-culture infections89. Even with this discovery 10 years ago, the effect of relative HIV-1 replicative fitness on disease progression has not been the subject of intense study owing to difficulties in accurately measuring HIV-1 fitness.
There have been only limited studies examining how virus fitness changes during natural infections31,32,90,91. The replication capacities of different HIV-1 isolates are commonly compared by measuring ex vivo growth kinetics in single virus infections31,32. The viruses used in many studies are not isolated from infected patients but rather are chimeric recombinant viruses containing gene(s) from the patient's virus within the genome of a laboratory HIV-1 strain32,92. Small environmental differences in separate single virus infections and the inherent variability of detection assays can prevent accurate estimates of viral fitness by these methods. By contrast, dual virus infections or competition assays involve multiple rounds of virus replication, are less affected by environmental changes and, as a result, can quantify small but significant differences in fitness29,93,94. In HIV research, multiple and single-cycle single virus infections, and competition experiments, have been used in studies that described impaired HIV-1 replicative fitness conferred by drug-resistance mutations95,96. Nevertheless, the impact of these drug resistance mutations in primary HIV-1 isolates (as opposed to chimeric viruses) has not been fully assessed.
Initial reports using HIV-1 competition assays in peripheral blood mononuclear cell (PBMC) cultures to measure fitness indicated that many long-term survivors harbour HIV-1 with an impaired replication capacity, whereas rapid progressors can be infected with more aggressive HIV-1 isolates30. Subsequent studies indicated that the genetic diversity and fitness of the intra-patient HIV-1 population continues to increase during disease and to diverge from the founder HIV-1 clones29,63,70 (Fig. 2). This diversity reaches an inflection point just before the inception of AIDS symptoms. During the asymptomatic period, the steady increase in HIV-1 diversity occurs concomitantly with increasing viral load and, more significantly, with increasing ex vivo replicative fitness of the infecting HIV-1 isolate29 (Fig. 2). Red Queen dynamics (in which the interaction between a parasite and its host leads to a constant evolutionary process of adaptation and counter-adaptation) predict that increasing replicative fitness must be associated with a continual expansion of the genetic breadth and size of a population97,98. Any strong selective pressure can result in the contraction of population size, the appearance of deleterious mutations and decreasing fitness99,100,101. Interestingly, the introduction of ARVs as a strong selective pressure during asymptomatic disease resulted in a dramatic decrease in HIV-1 load, genetic diversity and replicative fitness, even in the absence of drug resistance mutations29.
Following transmission, it is possible that the replicative fitness and genetic diversity of newly infecting HIV-1 isolates is lower than that of the inoculating virus from the donor (Box 1). Such a continual increase in HIV-1 diversity and fitness is in direct conflict with the idea that the HIV-specific acquired immune response can counter this viral expansion102. Discrepancies in these data might simply be due to the time period of sampling and analyses. HIV-1 genetic diversity and fitness only increases after the first one to two years of infection29 (Fig. 2). Immediately following acute infection, both host genetics and the HIV-specific immune response might have crucial roles in establishing a genetic diversity and fitness set point, which might also correspond with the well-documented viral-load set point83,103 (Fig. 2). Cell-mediated immunity could be the most dominant factor in specifically reducing viral load and, as a consequence, fitness and diversity104,105,106,107.
How can HIV-1 virulence be attenuated?
The genes at the human leukocyte antigen (HLA) loci are extremely variable. In humans in most geographical regions, it is typically rare to find a perfect match in the HLA A–G alleles that encode major histocompatibility complex (MHC) class I and in the six HLA D genes that encode MHC class II. Even in regions of specific ethnicities, there is considerable population diversity in HLA alleles, which encompass at least 21 major A, 35 B and 15 C alleles (see the dbMHC web site). Compared with Eurasian populations, HLA diversity is much greater in the main ethnic groups of sub-Saharan Africa; a study of >4,000 individuals characterized at the A, B and C loci found no preference for a single allele108. The least HLA diversity is often observed in more homogeneous Caucasian populations, most notably, the Caucasian Australian population (see the dbMHC web site)109.
How might a human population that is diverse in terms of HLA type or other host polymorphisms influence HIV-1 evolution? Quantitative aspects of the HIV-specific immune response (for example, high levels of HIV-specific cytotoxic T lymphocytes (CTLs) versus low levels) are self-limiting because this immunity is not transferred between individuals. However, a qualitative difference in terms of what the immune system 'sees' in the infecting HIV-1 strain could have a significant impact on virulence. A mismatch of HLA genes between the donor and recipient of a transmission pair would result in the presentation of a different set of HIV-1 peptide epitopes to CD8+ T cells in the recipient that were not recognized in the donor110,111. With each new transmission, the infecting virus must then evolve to escape this pressure, which in turn seems to reduce replicative fitness112,[113](/articles/nrmicro1594#ref-CR113 "Troyer, R. M. et al. The fitness cost of CTL escape: not a terrible hardship on HIV-1? [online]
, (XVI International AIDS Conference, Toronto, Canada 13–18 August, 2006)"). In human populations with a low HLA diversity (for example, in Australia), CTL escape mutations might become fixed along with compensatory mutations that restore or maintain HIV-1 virulence[109](/articles/nrmicro1594#ref-CR109 "Moore, C. B. et al. Evidence of HIV-1 adaptation to HLA-restricted immune responses at a population level. Science 296, 1439–1443 (2002).") ([Box 1](/articles/nrmicro1594#Sec2)). By contrast, the constant passage of HIV-1 through humans of different HLA types (for example, in Africa) might prevent the accumulation of compensatory mutations, which could stabilize CTL escape mutations ([Box 1](/articles/nrmicro1594#Sec2)). However, a model involving only HLA types is obviously too simplistic, considering the effects of other host factors. For example, polymorphisms in other host restriction factors, such as ABOBEC3G/3F and TRIM5α, could also alter disease progression[114](/articles/nrmicro1594#ref-CR114 "Sheehy, A. M., Gaddis, N. C., Choi, J. D. & Malim, M. H. Isolation of a human gene that inhibits HIV-1 infection and is suppressed by the viral Vif protein. Nature 418, 646–650 (2002)."),[115](/articles/nrmicro1594#ref-CR115 "Stremlau, M. et al. The cytoplasmic body component TRIM5α restricts HIV-1 infection in Old World monkeys. Nature 427, 848–853 (2004)."). Furthermore, host polymorphisms in the HIV-1 co-receptor CCR5 and its ligands (for example, CCL3L1) alter co-receptor or ligand expression levels and, as such, affect the ability of HIV-1 to use the co-receptor[78](/articles/nrmicro1594#ref-CR78 "Dean, M. et al. Genetic restriction of HIV-1 infection and progression to AIDS by a deletion allele of the CKR5 structural gene. Science 273, 1856–1862 (1996)."),[79](/articles/nrmicro1594#ref-CR79 "Berger, E. A., Murphy, P. M. & Farber, J. M. Chemokine receptors as HIV-1 coreceptors: roles in viral entry, tropism, and disease. Annu. Rev. Immunol. 17, 657–700 (1999)."),[80](/articles/nrmicro1594#ref-CR80 "Gonzalez, E. et al. Global survey of genetic variation in CCR5, RANTES, and MIP-1α: impact on the epidemiology of the HIV-1 pandemic. Proc. Natl Acad. Sci. USA 98, 5199–5204 (2001)."),[81](/articles/nrmicro1594#ref-CR81 "Gonzalez, E. et al. The influence of CCL3L1 gene-containing segmental duplications on HIV-1/AIDS susceptibility. Science 307, 1434–1440 (2005)."),[82](/articles/nrmicro1594#ref-CR82 "McDermott, D. H. et al. CCR5 promoter polymorphism and HIV-1 disease progression. Multicenter AIDS Cohort Study (MACS). Lancet 352, 866–870 (1998)."). If these polymorphisms exist at high frequencies in the human population, they too could result in an oscillation between HIV-1 sequences that, in this example, reduce or increase co-receptor avidity, a correlate of replicative fitness.In general, HIV-1 virulence might attenuate if, on average, the loss in fitness that occurs following transmission is greater than the gain in replicative fitness that occurs during asymptomatic disease progression (Box 1). Loss of fitness is probably due to the genetic bottleneck during transmission and/or escape from host restrictions or the host immune response during early disease. The continual introduction of new selective pressures and genetic bottlenecks would lead to the accumulation of deleterious mutations, which in turn would reduce replicative fitness or virulence. However, these hypotheses have not been empirically tested using HIV-1 transmission pairs.
Is there evidence for attenuation of HIV-1?
With the exceptions of anecdotes, a few case reports and one published study on a large cohort, there is no evidence that HIV-1 virulence has either increased or decreased during the past 20–30 years of the pandemic116,117,118,119,120,121. One of the main obstacles in comparing disease progression in the mid-1980s with the current day epidemic in the developed world is the significant medical advancements that have been made. In the developing world, until recently, few if any cohorts have been analysed for disease progression. Finally, owing to increased awareness and education about AIDS, patients are now diagnosed earlier, sometimes during acute infection, whereas in the 1980s many patients did not present to a clinic until the onset of AIDS. As a result, there is often the impression that HIV-1 infections are less aggressive now than they were at the beginning of the pandemic.
In a study published last year, >100 primary HIV-1 isolates were obtained from patient samples in Antwerp, Belgium, but only twelve could be matched from the periods 1985–1987 and 2002–2003 (Ref. 121). All 24 viruses from both time periods were competed against each other in PBMC from HIV-negative donors. Based on >500 head-to-head virus competition experiments, the recent HIV-1 isolates were significantly less fit than the historical isolates121. These findings indicate that HIV-1 might have attenuated in replicative fitness over the past 15–18 years. If the fitness of the infecting HIV-1 strain is a predictor of disease progression29,30,31,32, reduced ex vivo fitness in PBMC might be a strong correlate of decreased virulence. However, these results should be interpreted with caution owing to the limited sample size involved. Furthermore, the cross-sectional design of this study results in sampling of HIV-1 isolates at a single time point during disease progression, which was controlled for disease stage based on CD4+ T-cell count and viral load. Nonetheless, the increased fitness of the 1980 viruses versus the 2000 viruses was significant and greater than any increase in HIV-1 fitness observed during disease progression29,121. Future studies on large cohorts that span the epidemic temporally in various geographical regions are warranted but, as described below, these studies will again be limited to analyses of HIV-1 virulence (that is, replicative fitness) as rates of disease progression will not be available (see below).
Rates of disease progression have now been examined in a European HIV-infected cohort spanning the years 1986–2002 (Ref. 119). The slopes of CD4+ T-cell decline were calculated in antiretroviral-treatment-naive patients with confirmed dates of infection, at no fewer than nine time points over periods >1 year. Following this early period of the AIDS epidemic, there seems to be some evidence for slowing rates of disease progression from 1992–1998. Interestingly, the period following 1992 also corresponds to increasing use of combination ARV treatment, which could only be indirectly related to this attenuation as none of the patients received ARVs during the study period. It is possible that drug resistance mutations might have appeared at a higher frequency during sub-optimal treatment from 1992–1998, that is, before the widespread use of highly active antiretroviral therapy (HAART). These mutations have been associated with reduced fitness95,96 but their presence following a new transmission and in the absence of ARV treatment is low (<5–20%)122,123 and would not fully explain why the rates of disease progression might have decreased between 1992–1998.
The detection of fluctuations in the rate of CD4+ T-cell decline at the start of the HIV-1 epidemic in Europe is surprising given the preliminary data suggesting that replicative fitness might have been higher in the 1980s compared with the 2000s (Ref. 121). Slopes of CD4+ T-cell decline can be heavily influenced by the length of longitudinal follow-up, the follow-up period post-infection, and the number of data points124. For example, most patients in the 1980s presented to a clinic with advanced disease when the slopes of CD4+ T-cell decline are commonly lower than in early disease (especially once the level falls below 200 CD4+ T cells per μl)124,125. Therefore, 'slow' disease progression during 1986–1988 might be associated with the accrual of patients with more advanced disease. In general, natural history cohorts starting at early or acute infection and ending with AIDS-defining illnesses or morbidity (typically 3–10 years without ARV treatment) provide the best estimates of CD4+ T-cell decline and disease progression rates125. In the developed world, cohorts from the 1980s are not readily available owing to late diagnosis, whereas the current cohorts are difficult to assess for the natural history of disease due to ARV intervention. Finally, given the reduced HLA diversity and greater ethnic homogeneity in the Caucasian population, the attenuation rate of subtype B HIV-1 virulence might be less dramatic than the attenuation possible with non-B subtypes in sub-Saharan Africa.
In vivo and ex vivo fitness differences
Early observations on the rates of disease progression in west Africa showed that HIV-2 infections were less aggressive than HIV-1 infections126,127. HIV-2 is also transmitted less frequently than HIV-1 in human populations of similar demographics and similar opportunities for sexual contacts128,129. Whereas HIV-1 has spread across the globe, founder events of HIV-2 in areas other than west Africa did not result in regional epidemics (Fig. 3). Even HIV-1 infections are not evenly distributed among the different groups and subtypes: group N infections have only been characterized in five Cameroonians, whereas ∼30,000 group O infections are estimated in Cameroon and Gabon[6](/articles/nrmicro1594#ref-CR6 "UNAIDS/WHO. AIDS Epidemic Update 2006. [online]
, (UNAIDS/WHO, Geneva, 2006)."),[46](/articles/nrmicro1594#ref-CR46 "Ayouba, A. et al. HIV-1 group O infection in Cameroon, 1986 to 1998. Emerg. Infect. Dis. 7, 466–467 (2001).").Figure 3: HIV-1 diversity in the worldwide epidemic.
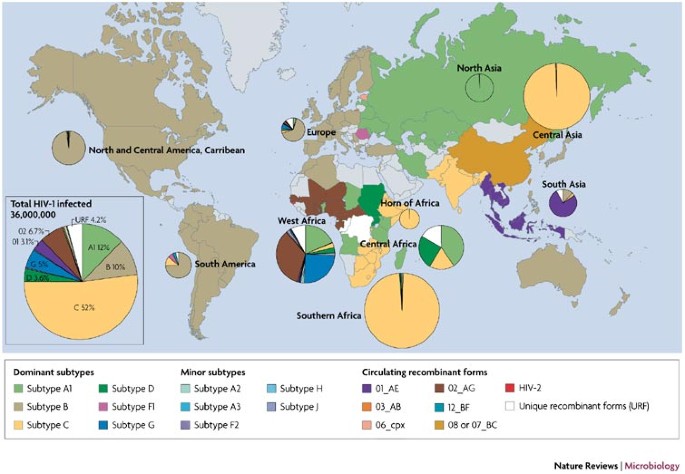
The frequency of each HIV-1 subtype and recombinant form was estimated in each country based on published findings. A complete breakdown of subtype prevalence per country and the countries present in each region are listed in the Supplementary information S1 (table). The countries are colour-coded based on the dominant HIV-1 group main (M) subtype. The countries coloured grey have a low level of HIV-1 prevalence or were not represented in the scientific literature related to HIV-1 subtype prevalence. The pie charts depict the proportion of each subtype or recombinant form in each geographical region. The size of the pies is proportional to the number of HIV-1 infected individuals in that particular region.
HIV-1 group M subtype C has spread more rapidly than any other M subtype, partly as a result of recent subtype C pandemics in southern Africa, south America and Asia130,131,132,133 (Figs 3,4a; and Supplementary information S1 (table)). 'Pure' HIV-1 subtype C or HIV-1 recombinant forms containing at least the envelope gene of subtype C are now responsible for >50% of the HIV-1 infections worldwide130. A founder event of subtype C or a C-containing recombinant form in many regions has also resulted in an apparent displacement of existing HIV-1 subtypes (such as subtypes B and CRF01_AE in south China131,132, many subtypes in Kinshasa, Democratic Republic of Congo134 and subtype B in southern Brazil133) (Figs 3,4A). This displacement could be due to the introduction of subtype C into a population by different transmission routes (heterosexual transmission versus intravenous drug use) or increased sexual activity (for example, commercial sex workers)135. A subtype might initially predominate in a specific transmission group but there is little supporting evidence to suggest that subtypes A, B, C, D and CRF01_AE (also referred to as E) are any more or less transmissible by a specific route, in a specific ethnic group or in specific cell types53,136,137,138,139,140,141. In addition, such initial predominance is generally lost during an epidemic. For example, in Thailand HIV-1 subtypes B and CRF01_AE were segregated to intravenous drug users and heterosexuals, respectively, in the late 1980s but are now more uniformly mixed in the Thai population142.
Figure 4: Relationship between the increasing prevalence of HIV-1 subtype C and its low pathogenic fitness.
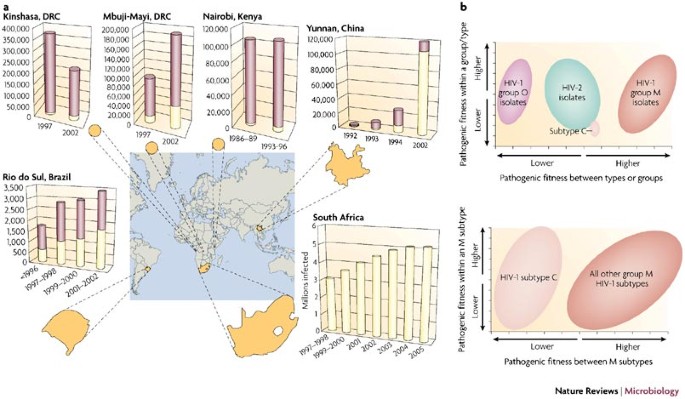
The prevalence of HIV-1 subtype C or subtype C-containing recombinant forms has increased in proportion to other HIV-1 subtypes in Rio do Sul, Brazil (from 35% in 1996 to 52% 2002)133, in Kinshasa and Mbuji-Mayi, Democratic Republic of Congo (DRC) (from 2.1% and 16.3% in 1997 to 9.7% and 25% in 2002, respectively)134 and in Yunnan, China (from 5.1% in 1992 to 90% in 2002)162,163. By contrast, subtype C is dominant in South Africa164 and did not increase in proportion to subtypes A and D or recombinant forms in Kenya165. The number of HIV-1 cases increased in all of these regional epidemics (except in Kinshasa)[6](/articles/nrmicro1594#ref-CR6 "UNAIDS/WHO. AIDS Epidemic Update 2006. [online]
, (UNAIDS/WHO, Geneva, 2006)."). **a** | The number of HIV-1 infections in specific years is subdivided into subtype C (yellow) and non-subtype-C (maroon) HIV-1 infections. **b** | A schematic representation of the pathogenic fitness of human lentiviruses, derived from >3,000 pair-wise dual HIV-1 competition experiments[26](/articles/nrmicro1594#ref-CR26 "Deval, J. et al. Mechanistic basis for reduced viral and enzymatic fitness of HIV-1 reverse transcriptase containing both K65R and M184V mutations. J. Biol. Chem. 279, 509–516 (2004)."),[27](/articles/nrmicro1594#ref-CR27 "Bull, J. J. Virulence. Evolution 48, 1423–1437 (1994)."),[49](/articles/nrmicro1594#ref-CR49 "Yamaguchi, J. et al. Identification of HIV type 1 group N infections in a husband and wife in Cameroon: viral genome sequences provide evidence for horizontal transmission. AIDS Res. Hum. Retroviruses 22, 83–92 (2006)."),[50](/articles/nrmicro1594#ref-CR50 "Salemi, M. et al. Dating the common ancestor of SIVcpz and HIV-1 group M and the origin of HIV-1 subtypes using a new method to uncover clock-like molecular evolution. FASEB J. 15, 276–278 (2001)."),[108](/articles/nrmicro1594#ref-CR108 "Cao, K. et al. Differentiation between African populations is evidenced by the diversity of alleles and haplotypes of HLA class I loci. Tissue Antigens 63, 293–325 (2004)."),[120](/articles/nrmicro1594#ref-CR120 "Kannangara, S., DeSimone, J. A. & Pomerantz, R. J. Attenuation of HIV-1 infection by other microbial agents. J. Infect. Dis. 192, 1003–1009 (2005)."),[123](/articles/nrmicro1594#ref-CR123 "Turner, D. & Wainberg, M. A. HIV transmission and primary drug resistance. AIDS Rev. 8, 17–23 (2006)."),[125](/articles/nrmicro1594#ref-CR125 "McCune, J. M. The dynamics of CD4+ T-cell depletion in HIV disease. Nature 410, 974–979 (2001)."),[165](/articles/nrmicro1594#ref-CR165 "Rainwater, S. et al. No evidence for rapid subtype c spread within an epidemic in which multiple subtypes and intersubtype recombinants circulate. AIDS Res. Hum. Retroviruses 21, 1060–1065 (2005)."). The coloured ovals plot the fitness of primary HIV-1 isolates competed against isolates of the same type, group or subtype (y axis; mean fitness of 1 or equal fitness) compared with the fitness of primary HIV-1 isolates competed against isolates of different types, groups or subtypes. Each oval encompasses the fitness (x and y fitness values) of at least 10 to 20 primary HIV-1 isolates. M, main; O, other.Recent studies have attempted to establish the ex vivo 'pathogenic' and 'transmission' fitness of different HIV types, groups and subtypes52. Ex vivo 'pathogenic fitness' has been previously described as the relative replication capacity of HIV-1 in primary blood cells (CD4+ T cells and PBMCs), which in turn, might be related to HIV-1 virulence30,53. By contrast, ex vivo 'transmission fitness' is measured by competing primary HIV-1 isolates in cells of the dendritic lineage, which are derived from blood monocytes or human skin53,143. Future dual HIV-1 competition experiments using vaginal or cervical biopsy explants might be the best model for transmission fitness65,66. To first establish the 'pathogenic fitness' (or virulence) of HIV, pair-wise competitions were done with eight HIV-2, six HIV-1 group O and 15 HIV-1 group M isolates (2 subtype A, 5 subtype B, 4 subtype C, 2 subtype D and 2 subtype CRF01_AE) in PBMCs144 (Fig. 4b). These viruses were classified as using either the CCR5 (R5) or the CXCR4 (X4) co-receptor for entry. When HIV isolates of the same phenotype (X4 or R5) were competed against each other, the following fitness order (based on >2,000 competitions) was observed (Fig. 4b): HIV-1 group M (subtype A, B, D and CRF01_AE) had a greater fitness than subtype C, which in turn was greater than HIV-2, and HIV-1 group O showed the lowest fitness.
With the exception of subtype C, this order reflects the prevalence of these human lentiviruses in the human population and the proposed rates of transmission efficiency128,129. The R5 HIV-1 subtype C isolates were at least 100-fold less fit than HIV-1 isolates of any other group M subtype53. Aside from subtype C, no other HIV-1 subtype has shown a significant fitness difference in group M53,144. Subtype C HIV-1 isolates are preferentially CCR5-tropic and non-syncytium-inducing (NSI) throughout disease, whereas infections with HIV-1 isolates of other subtypes result in a switch from CCR5 to CXCR4-tropic virus in approximately 50% of late disease cases. A few rare X4 subtype C isolates have been obtained from infected Zimbabweans late in disease145 but even the switch from R5 to X4 did not restore fitness, compared with other group M isolates (Nankya, I. et al, unpublished data).
What causes differential spread?
Differential spread of human lentiviruses in the host population is controlled by both transmission efficiency and opportunity, which is collectively referred to as R0 (Ref. 22). Several models of microparasite expansion in humans have been proposed20,22,33,146,147but most assume that during the early stages of the epidemic, the rate of infection (dY/dt) simply increases as a function of the number of infected individuals (Y) during an infectious period (v = rate of moving into a non-infectious state), the probability of infecting a new host (β) and the frequency of sexual contact (c) (Ref. 22).

The opportunities for HIV-1 transmission relate to the number of sexual contacts, which are more frequent during acute infection and in the asymptomatic period of disease than during AIDS. An infected individual (without general knowledge of the transmission routes or infection status) could engage in several sexual encounters during the acute or early phase (approximately 3 months)148, the period of highest HIV-1 load61,62. Therefore, the exponential growth of HIV-1 infections in the early 1980s could have been primarily the result of transmission from acutely infected men having sex with men or from intravenous drug users148,149,150 (Box 1). However, in heterosexual populations with a reduced frequency of sexual contacts, a donor might transmit HIV-1 to more recipients during a long asymptomatic period (2–5 years) of infection, with moderate viral load, than during the acute or early infection stage (1–3 months), with high viral load. Low HIV-1 virulence, which could lead to longer asymptomatic periods, could also increase the opportunity for transmission (Box 1).
Similarly, poor fitness of HIV-1 group O and HIV-2 compared with HIV-1 group M isolates was found when competitions were carried out in both PBMCs (ex vivo pathogenic fitness) and in dendritic–T-cell cultures (ex vivo transmission fitness)144. In relation to this ex vivo model, poor transmission efficiency has been well documented for HIV-2 compared with HIV-1 in the human populations in which both circulate128,129. By contrast, subtype C HIV-1 isolates had similar ex vivo transmission fitness53 compared with group M subtype B isolates in Langerhans cells even though subtype C isolates are at least 100-fold less fit in PBMC cultures53. In vivo observations indicate that subtype C HIV-1 is transmitted as efficiently as other HIV-1 group M isolates in human cohorts135,137 and in rhesus macaques, through the use of SIV–HIV env chimeric virus (SHIV-MJ4)151. These ex vivo and in vivo observations imply that HIV-1 subtype C is efficiently transmitted but is less virulent than other HIV-1 group M isolates.
HIV-2 and HIV-1 groups O and N might have had limited expansion in the human population due to poor host adaptation and transmission efficiencies. By contrast, HIV-1 group M seems to be more virulent as well as more transmissible. Therefore, the progenitor of the HIV-1 group M lineage might have been more 'fit' for human infection, promoting further adaptation through rapid evolution and passage through the human population. New founder events in segregated human populations in central Africa might have led to subsequent divergence into subtypes. HIV-1 subtypes probably evolved and diverged under similar selection pressures, unless infecting a human population with distinct genetic polymorphisms that had an effect on virulence. Adaptation to the human population followed by attenuation of lethal virulence might, however, be occurring at different rates for divergent HIV-1 clades. If diversity in HLA types has a significant role in HIV-1 evolution, subtypes predominating in Africa, such as subtype C, might attenuate virulence at a faster rate than HIV-1 subtype B, which infects the Caucasian population of lower HLA diversity in the developed world.
Prevalence and reduced virulence
HIV-1 subtype C might be in a more advanced stage of attenuation than other HIV-1 subtypes53,96,144. If it is less virulent than other subtypes, subtype C infections might result in slower disease progression, longer periods of asymptomatic infection and more opportunities for transmission; that is, it would be associated with an increase in R0 (see equation [1]; Box 1). To support a model of disproportionate expansion of HIV-1 subtype C in the human population (Figs 3,4a), the transmission efficiency of subtype C must be greater than, or comparable to, other HIV-1 group M strains. Preliminary data suggest that subtype C is transmitted as efficiently as other HIV-1 group M subtypes53,135,137,151. Therefore, decreased virulence could have a key role in the spread of subtype C by increasing the opportunity for transmission33. So far, comparisons of cohorts infected with subtype C and other subtypes show similar or higher viral loads in the subtype C-infected individuals152,153. These initial observations would argue against the possible subtype C attenuation and would support the more popular assumption, that subtype C is more virulent.
However, there are few studies on the natural history and progression of patients infected by any HIV-1 subtype other than subtype B154,155,156,157. Two studies have described faster disease progression in individuals infected with subtype D compared with subtype A- or subtype C-infected individuals in Uganda and Tanzania154,155,156. The possibility of greater subtype D virulence has been attributed to a higher propensity to switch from the NSI/R5 phenotype to the more aggressive syncytium-inducing (SI)/X4 phenotype158. By contrast, subtype C rarely switches from the NSI/R5 to the SI/X4 phenotype. At a recent presentation at the sixteenth International AIDS Conference in Toronto, Canada[159](/articles/nrmicro1594#ref-CR159 "Arts, E. J. et al. Infection with subtype C HIV-1 of lower replicative fitness as compared to subtypes A and D leads to slower disease progression in Zimbabwean and Ugandan women. [online]
, (XVI International AIDS Conference, Toronto, Canada 13–18 August, 2006)."), interim analyses of disease progression were described in a cohort of 256 subtype A-, C- and D-infected women, recruited at acute or early infection and followed for a mean of 36 months. The mean slope of CD4+ T-cell decline in the subtype C-infected women from Zimbabwe was 2.3-fold slower than in subtype A- and D-infected women from Uganda (_p_<0.008). However, there were no differences in the mean viral loads at 3 and 12 months between the countries or between different subtypes. Slower disease progression, as described by slower declines in CD4+ T-cell counts, was not attributable to any other factors (such as opportunistic infections, sexual activity, diet, age and weight) apart from being infected with subtype C versus subtype A or D. In the Bantu corridor extending from Zimbabwe to Uganda, the frequency of HLA-A, -B and -C alleles and other host polymorphisms (for example, CCR5 deletions or promoter polymorphisms) are similar and could rule out obvious human genetic differences skewing HIV-1 evolution[108](/articles/nrmicro1594#ref-CR108 "Cao, K. et al. Differentiation between African populations is evidenced by the diversity of alleles and haplotypes of HLA class I loci. Tissue Antigens 63, 293–325 (2004).").Summary
The attenuation of infectious pathogens remains contentious and many doubt that the spread of HIV-1 through the human population will lead to decreased virulence as HIV-1 isolates actually gain replicative (or pathogenic) fitness during infection of human hosts. However, this gain might not be sufficient to reverse the loss in pathogenic fitness that occurs during transmission and early disease. The extreme genetic bottleneck following transmission reduces the HIV-1 population size and diversity by at least 10,000-fold. In vitro studies indicate that this genetic reduction correlates with a significant fitness loss. The few HIV-1 clones establishing infection must evade the immune system, resulting in yet another series of genetic bottlenecks reducing fitness. Therefore, attenuation of virulence might occur if the net fitness loss during transmission or early disease is greater than the increase in pathogenic fitness during disease progression and between transmission events. Greater diversity in HLA alleles in African populations compared with Caucasian populations might result in stronger immune pressure in the human population and possibly faster rates of HIV-1 attenuation. Is the global dominance of HIV-1 subtype C related to an attenuation of virulence? Does subtype C infection lead to slower disease progression and more opportunities for new transmission events? These questions might hold the key to the future of the HIV-1 epidemic and could provide a new focus for ARV treatment and vaccine design.
References
- Lemey, P., Pybus, O. G., Van, D. S. & Vandamme, A. M. A Bayesian statistical analysis of human T-cell lymphotropic virus evolutionary rates. Infect. Genet. Evol. 5, 291–298 (2005).
Article CAS PubMed Google Scholar - Van, D. S., Salemi, M. & Vandamme, A. M. Dating the origin of the African human T-cell lymphotropic virus type-i (HTLV-I) subtypes. Mol. Biol. Evol. 18, 661–671 (2001).
Article Google Scholar - Yoshida, M. Discovery of HTLV-1, the first human retrovirus, its unique regulatory mechanisms, and insights into pathogenesis. Oncogene 24, 5931–5937 (2005).
Article CAS PubMed Google Scholar - Coulthart, M. B., Posada, D., Crandall, K. A. & Dekaban, G. A. On the phylogenetic placement of human T cell leukemia virus type 1 sequences associated with an Andean mummy. Infect. Genet. Evol. 6, 91–96 (2006).
Article CAS PubMed Google Scholar - Korber, B. et al. Timing the ancestor of the HIV-1 pandemic strains. Science 288, 1789–1796 (2000).
Article CAS PubMed Google Scholar - UNAIDS/WHO. AIDS Epidemic Update 2006. [online], (UNAIDS/WHO, Geneva, 2006).
- Geisbert, T. W. & Jahrling, P. B. Exotic emerging viral diseases: progress and challenges. Nature Med. 10, S110–S121 (2004).
Article CAS PubMed Google Scholar - Doherty, P. C., Turner, S. J., Webby, R. G. & Thomas, P. G. Influenza and the challenge for immunology. Nature Immunol. 7, 449–455 (2006).
Article CAS Google Scholar - Perlman, S. & Dandekar, A. A. Immunopathogenesis of coronavirus infections: implications for SARS. Nature Rev. Immunol. 5, 917–927 (2005).
Article CAS Google Scholar - Gage, K. L. & Kosoy, M. Y. Natural history of plague: perspectives from more than a century of research. Annu. Rev. Entomol. 50, 505–528 (2005).
Article CAS PubMed Google Scholar - Drancourt, M., Houhamdi, L. & Raoult, D. Yersinia pestis as a telluric, human ectoparasite-borne organism. Lancet Infect. Dis. 6, 234–241 (2006).
Article PubMed Google Scholar - Fenner, F. & Radcliffe, F. N. Myxomatosis (Cambridge University Press, Cambridge, 1965).
Google Scholar - Zuniga, M. C. A pox on thee! Manipulation of the host immune system by myxoma virus and implications for viral–host co-adaptation. Virus Res. 88, 17–33 (2002).
Article CAS PubMed Google Scholar - Best, S. M. & Kerr, P. J. Coevolution of host and virus: the pathogenesis of virulent and attenuated strains of myxoma virus in resistant and susceptible European rabbits. Virology 267, 36–48 (2000).
Article CAS PubMed Google Scholar - Knell, R. J. Syphilis in renaissance Europe: rapid evolution of an introduced sexually transmitted disease? Proc. Biol. Sci. 271, S174–S176 (2004).
PubMed PubMed Central Google Scholar - Jin, M. J. et al. Mosaic genome structure of simian immunodeficiency virus from west African green monkeys. EMBO J. 13, 2935–2947 (1994).
Article CAS PubMed PubMed Central Google Scholar - Apetrei, C., Robertson, D. L. & Marx, P. A. The history of SIVS and AIDS: epidemiology, phylogeny and biology of isolates from naturally SIV infected non-human primates (NHP) in Africa. Front. Biosci. 9, 225–254 (2004).
Article CAS PubMed Google Scholar - Courgnaud, V. et al. Identification of a new simian immunodeficiency virus lineage with a vpu gene present among different cercopithecus monkeys (C. mona, C. cephus, and C. nictitans) from Cameroon. J. Virol. 77, 12523–12534 (2003).
Article CAS PubMed PubMed Central Google Scholar - Hassel, M. P. The Spatial and Temporal Dynamics of Host-Parasitoid Interactions (Oxford University Press, Oxford, 2000).
Google Scholar - Diekmann, O. & Hessterbeek, O. Mathematical Epidemiology of Infectious Diseases: Model Building, Analysis, and Interpretation (Wiley, Chichester, 2006).
Google Scholar - Dronamraju, K. R. Infectious Diseases and Host-Pathogen Evolution (Cambridge University Press, Cambridge, 2004).
Book Google Scholar - Anderson, R. M. & May, R. M. Infectious Diseases of Humans: Dynamics and Control (Oxford University Press, Oxford, 1991).
Google Scholar - Arts, E. J. & Quinones-Mateu, M. E. Sorting out the complexities of HIV-1 fitness. AIDS 17, 780–781 (2003).
Article PubMed Google Scholar - Quinones-Mateu, M. E. & Arts, E. J. HIV-1 Fitness: Implications for Drug Resistance, Disease Progression, and Global Epidemic Evolution. [online], (HIV Sequence Compendium, Theoretical Biology and Biophysics Group, Los Alamos National Laboratory, Los Alamos, 2001).
Google Scholar - Feng, J. Y. & Anderson, K. S. Mechanistic studies examining the efficiency and fidelity of DNA synthesis by the 3TC-resistant mutant (184V) of HIV-1 reverse transcriptase. Biochemistry 38, 9440–9448 (1999).
Article CAS PubMed Google Scholar - Deval, J. et al. Mechanistic basis for reduced viral and enzymatic fitness of HIV-1 reverse transcriptase containing both K65R and M184V mutations. J. Biol. Chem. 279, 509–516 (2004).
Article CAS PubMed Google Scholar - Bull, J. J. Virulence. Evolution 48, 1423–1437 (1994).
CAS PubMed Google Scholar - Bremermann, H. J. & Pickering, J. A game-theoretical model of parasite virulence. J. Theor. Biol. 100, 411–426 (1983).
Article CAS PubMed Google Scholar - Troyer, R. M. et al. Changes in human immunodeficiency virus type 1 fitness and genetic diversity during disease progression. J. Virol. 79, 9006–9018 (2005).
Article CAS PubMed PubMed Central Google Scholar - Quinones-Mateu, M. E. et al. A dual infection/competition assay shows a correlation between ex vivo human immunodeficiency virus type 1 fitness and disease progression. J. Virol. 74, 9222–9233 (2000).
Article CAS PubMed PubMed Central Google Scholar - Blaak, H., Brouwer, M., Ran, L. J., de Wolf, F. & Schuitemaker, H. In vitro replication kinetics of human immunodeficiency virus type 1 (HIV-1) variants in relation to virus load in long-term survivors of HIV-1 infection. J. Infect. Dis. 177, 600–610 (1998).
Article CAS PubMed Google Scholar - Barbour, J. D. et al. Higher CD4+ T cell counts associated with low viral pol replication capacity among treatment-naive adults in early HIV-1 infection. J. Infect. Dis. 190, 251–256 (2004).
Article CAS PubMed Google Scholar - Ewald, P. W. Evolution of Infectious Disease (Oxford University Press, Oxford, 1994).
Google Scholar - Nowak, M. A. & May, R. M. Virus Dynamics: Mathematical Principles of Immunology and Virology (Oxford University Press, Oxford, 2000).
Google Scholar - Maynard, S. J. Group selection and kin selection. Nature 201, 1145–1147 (1964).
Article Google Scholar - Szathmary, E. & Maynard, S. J. From replicators to reproducers: the first major transitions leading to life. J. Theor. Biol. 187, 555–571 (1997).
Article CAS PubMed Google Scholar - Keele, B. F. et al. Chimpanzee reservoirs of pandemic and nonpandemic HIV-1. Science 313, 523–526 (2006).
Article CAS PubMed PubMed Central Google Scholar - Gao, F. et al. Origin of HIV-1 in the chimpanzee Pan troglodytes troglodytes. Nature 397, 436–441 (1999).
Article CAS PubMed Google Scholar - Santiago, M. L. et al. SIVcpz in wild chimpanzees. Science 295, 465 (2002).
Article CAS PubMed Google Scholar - Van Heuverswyn, F. et al. Human immunodeficiency viruses: SIV infection in wild gorillas. Nature 444, 164 (2006).
Article CAS PubMed Google Scholar - Horimoto, T. & Kawaoka, Y. Influenza: lessons from past pandemics, warnings from current incidents. Nature Rev. Microbiol. 3, 591–600 (2005).
Article CAS Google Scholar - Hirsch, V. M., Olmsted, R. A., Murphey-Corb, M., Purcell, R. H. & Johnson, P. R. An African primate lentivirus (SIVsm) closely related to HIV-2. Nature 339, 389–392 (1989).
Article CAS PubMed Google Scholar - Lemey, P. et al. Tracing the origin and history of the HIV-2 epidemic. Proc. Natl Acad. Sci. USA 100, 6588–6592 (2003).
Article CAS PubMed PubMed Central Google Scholar - Schim van der Loeff, M. F. & Aaby, P. Towards a better understanding of the epidemiology of HIV-2. AIDS 13, S69–S84 (1999).
Google Scholar - Schim van der Loeff, M. F. et al. Sixteen years of HIV surveillance in a West African research clinic reveals divergent epidemic trends of HIV-1 and HIV-2. Int. J. Epidemiol. 35, 1322–1328 (2006).
Article PubMed Google Scholar - Ayouba, A. et al. HIV-1 group O infection in Cameroon, 1986 to 1998. Emerg. Infect. Dis. 7, 466–467 (2001).
Article CAS PubMed PubMed Central Google Scholar - Yamaguchi, J. et al. HIV infections in northwestern Cameroon: identification of HIV type 1 group O and dual HIV type 1 group M and group O infections. AIDS Res. Hum. Retroviruses 20, 944–957 (2004).
Article CAS PubMed Google Scholar - Yamaguchi, J. et al. HIV-1 Group N: evidence of ongoing transmission in Cameroon. AIDS Res. Hum. Retroviruses 22, 453–457 (2006).
Article CAS PubMed Google Scholar - Yamaguchi, J. et al. Identification of HIV type 1 group N infections in a husband and wife in Cameroon: viral genome sequences provide evidence for horizontal transmission. AIDS Res. Hum. Retroviruses 22, 83–92 (2006).
Article CAS PubMed Google Scholar - Salemi, M. et al. Dating the common ancestor of SIVcpz and HIV-1 group M and the origin of HIV-1 subtypes using a new method to uncover clock-like molecular evolution. FASEB J. 15, 276–278 (2001).
Article CAS PubMed Google Scholar - Travers, S. A. et al. Timing and reconstruction of the most recent common ancestor of the subtype C clade of human immunodeficiency virus type 1. J. Virol. 78, 10501–10506 (2004).
Article CAS PubMed PubMed Central Google Scholar - Arien, K. K. et al. The replicative fitness of primary human immunodeficiency virus type 1 (HIV-1) group M, HIV-1 group O, and HIV-2 isolates. J. Virol. 79, 8979–8990 (2005).
Article CAS PubMed PubMed Central Google Scholar - Ball, S. C. et al. Comparing the ex vivo fitness of CCR5-tropic human immunodeficiency virus type 1 isolates of subtypes B and C. J. Virol. 77, 1021–1038 (2003).
Article CAS PubMed PubMed Central Google Scholar - Barnett, S. W., Quiroga, M., Werner, A., Dina, D. & Levy, J. A. Distinguishing features of an infectious molecular clone of the highly divergent and noncytopathic human immunodeficiency virus type 2 UC1 strain. J. Virol. 67, 1006–1014 (1993).
Article CAS PubMed PubMed Central Google Scholar - Talbott, R., Kraus, G., Looney, D. & Wong-Staal, F. Mapping the determinants of human immunodeficiency virus 2 for infectivity, replication efficiency, and cytopathicity. Proc. Natl Acad. Sci. USA 90, 4226–4230 (1993).
Article CAS PubMed PubMed Central Google Scholar - Pollakis, G. et al. Phenotypic and genotypic comparisons of CCR5- and CXCR4-tropic human immunodeficiency virus type 1 biological clones isolated from subtype C-infected individuals. J. Virol. 78, 2841–2852 (2004).
Article CAS PubMed PubMed Central Google Scholar - Curran, J. W. et al. Epidemiology of HIV infection and AIDS in the United States. Science 239, 610–616 (1988).
Article CAS PubMed Google Scholar - Parazzini, F. et al. Number of sexual partners, condom use and risk of human immunodeficiency virus infection. Int. J. Epidemiol. 24, 1197–1203 (1995).
Article CAS PubMed Google Scholar - Ryder, R. W. & Behets, F. Reasons for the wide variation in reported rates of mother-to-child transmission of HIV-1. AIDS 8, 1495–1497 (1994).
Article CAS PubMed Google Scholar - Gray, R. H. et al. Probability of HIV-1 transmission per coital act in monogamous, heterosexual, HIV-1-discordant couples in Rakai, Uganda. Lancet 357, 1149–1153 (2001).
Article CAS PubMed Google Scholar - Quinn, T. C. et al. Viral load and heterosexual transmission of human immunodeficiency virus type 1. Rakai Project Study Group. N. Engl. J Med. 342, 921–929 (2000).
Article CAS PubMed Google Scholar - Garcia, P. M. et al. Maternal levels of plasma human immunodeficiency virus type 1 RNA and the risk of perinatal transmission. Women and Infants Transmission Study Group. N. Engl. J Med. 341, 394–402 (1999).
Article CAS PubMed Google Scholar - Shankarappa, R. et al. Consistent viral evolutionary changes associated with the progression of human immunodeficiency virus type 1 infection. J. Virol. 73, 10489–10502 (1999).
Article CAS PubMed PubMed Central Google Scholar - Zhu, T. et al. Genotypic and phenotypic characterization of HIV-1 patients with primary infection. Science 261, 1179–1181 (1993).
Article CAS PubMed Google Scholar - Shattock, R. J. & Moore, J. P. Inhibiting sexual transmission of HIV-1 infection. Nature Rev. Microbiol. 1, 25–34 (2003).
Article CAS Google Scholar - Shattock, R. J., Griffin, G. E. & Gorodeski, G. I. In vitro models of mucosal HIV transmission. Nature Med. 6, 607–608 (2000).
Article CAS PubMed Google Scholar - Bergstrom, C. T., McElhany, P. & Real, L. A. Transmission bottlenecks as determinants of virulence in rapidly evolving pathogens. Proc. Natl Acad. Sci. USA 96, 5095–5100 (1999).
Article CAS PubMed PubMed Central Google Scholar - Lazaro, E., Escarmis, C., Perez-Mercader, J., Manrubia, S. C. & Domingo, E. Resistance of virus to extinction on bottleneck passages: study of a decaying and fluctuating pattern of fitness loss. Proc. Natl Acad. Sci. USA 100, 10830–10835 (2003).
Article CAS PubMed PubMed Central Google Scholar - Elena, S. F. et al. Evolution of fitness in experimental populations of vesicular stomatitis virus. Genetics 142, 673–679 (1996).
Article CAS PubMed PubMed Central Google Scholar - Sagar, M. et al. Infection with multiple human immunodeficiency virus type 1 variants is associated with faster disease progression. J. Virol. 77, 12921–12926 (2003).
Article CAS PubMed PubMed Central Google Scholar - Pontesilli, O. et al. Longitudinal analysis of human immunodeficiency virus type 1-specific cytotoxic T lymphocyte responses: a predominant gag-specific response is associated with nonprogressive infection. J. Infect. Dis. 178, 1008–1018 (1998).
Article CAS PubMed Google Scholar - Dyer, W. B. et al. Strong human immunodeficiency virus (HIV)-specific cytotoxic T- lymphocyte activity in Sydney blood bank cohort patients infected with _nef_-defective HIV type 1. J. Virol. 73, 436–443 (1999).
Article CAS PubMed PubMed Central Google Scholar - Cao, Y., Qin, L., Zhang, L., Safrit, J. & Ho, D. D. Virologic and immunologic characterization of long-term survivors of human immunodeficiency virus type 1 infection. N. Eng. J. Med. 332, 201–208 (1995).
Article CAS Google Scholar - Pantaleo, G. et al. Studies in subjects with long-term nonprogressive human immunodeficiency virus infection. N. Eng. J. Med. 332, 209–216 (1995).
Article CAS Google Scholar - Montefiori, D. C. et al. Neutralizing and infection-enhancing antibody responses to human immunodeficiency virus type 1 in long-term nonprogressors. J. Infect. Dis. 173, 60–67 (1996).
Article CAS PubMed Google Scholar - Carotenuto, P., Looij, D., Keldermans, L., de Wolf, F. & Goudsmit, J. Neutralizing antibodies are positively associated with CD4+ T-cell counts and T-cell function in long-term AIDS-free infection. AIDS 12, 1591–1600 (1998).
Article CAS PubMed Google Scholar - Rosenberg, E. S. et al. Vigorous HIV-1-specific CD4+ T cell responses associated with control of viremia. Science 278, 1447–1450 (1997).
Article CAS PubMed Google Scholar - Dean, M. et al. Genetic restriction of HIV-1 infection and progression to AIDS by a deletion allele of the CKR5 structural gene. Science 273, 1856–1862 (1996).
Article CAS PubMed Google Scholar - Berger, E. A., Murphy, P. M. & Farber, J. M. Chemokine receptors as HIV-1 coreceptors: roles in viral entry, tropism, and disease. Annu. Rev. Immunol. 17, 657–700 (1999).
Article CAS PubMed Google Scholar - Gonzalez, E. et al. Global survey of genetic variation in CCR5, RANTES, and MIP-1α: impact on the epidemiology of the HIV-1 pandemic. Proc. Natl Acad. Sci. USA 98, 5199–5204 (2001).
Article CAS PubMed PubMed Central Google Scholar - Gonzalez, E. et al. The influence of CCL3L1 gene-containing segmental duplications on HIV-1/AIDS susceptibility. Science 307, 1434–1440 (2005).
Article CAS PubMed Google Scholar - McDermott, D. H. et al. CCR5 promoter polymorphism and HIV-1 disease progression. Multicenter AIDS Cohort Study (MACS). Lancet 352, 866–870 (1998).
Article CAS PubMed Google Scholar - Mellors, J. W. et al. Prognosis in HIV-1 infection predicted by the quantity of virus in plasma. Science 272, 1167–1170 (1996).
Article CAS PubMed Google Scholar - Collier, A. C. et al. Treatment of human immunodeficiency virus infection with saquinavir, zidovudine, and zalcitabine. AIDS Clinical Trials Group. N. Engl. J. Med. 334, 1011–1017 (1996).
Article CAS PubMed Google Scholar - Silvestri, G. et al. Nonpathogenic SIV infection of sooty mangabeys is characterized by limited bystander immunopathology despite chronic high-level viremia. Immunity. 18, 441–452 (2003).
Article CAS PubMed Google Scholar - Rodriguez, B. et al. Predictive value of plasma HIV RNA level on rate of CD4 T-cell decline in untreated HIV infection. JAMA 296, 1498–1506 (2006).
Article CAS PubMed Google Scholar - Deacon, N. J. et al. Genomic structure of an attenuated quasispecies of HIV-1 from a blood transfusion donor and recipients. Science 270, 988–991 (1995).
Article CAS PubMed Google Scholar - Kirchhoff, F., Greenough, T. C., Brettler, D. B., Sullivan, J. L. & Desrosiers, R. C. Brief report: absence of intact nef sequences in a long-term survivor with nonprogressive HIV-1 infection. N. Eng. J. Med. 332, 228–232 (1995).
Article CAS Google Scholar - Huang, Y., Zhang, l. & Ho, D. D. Biological characterization of nef in long-term survivors of human immunodeficiency virus type 1 infection. J. Virol. 69, 8142–8146 (1995).
Article CAS PubMed PubMed Central Google Scholar - Leroux, C., Issel, C. J. & Montelaro, R. C. Novel and dynamic evolution of equine infectious anemia virus genomic quasispecies associated with sequential disease cycles in an experimentally infected pony. J. Virol. 71, 9627–9639 (1997).
Article CAS PubMed PubMed Central Google Scholar - Plagemann, P. G., Chen, Z. & Li, K. Replication competition between lactate dehydrogenase-elevating virus quasispecies in mice. Implications for quasispecies selection and evolution. Arch. Virol. 146, 1283–1296 (2001).
Article CAS PubMed Google Scholar - Lu, J. & Kuritzkes, D. R. A novel recombinant marker virus assay for comparing the relative fitness of hiv-1 reverse transcriptase variants. J. Acquir. Immune. Defic. Syndr. 27, 7–13 (2001).
Article CAS PubMed Google Scholar - Holland, J. J., de la Torre, J. C., Clarke, D. K. & Duarte, E. Quantitation of relative fitness and great adaptability of clonal populations of RNA viruses. J. Virol. 65, 2960–2967 (1991).
Article CAS PubMed PubMed Central Google Scholar - Domingo, E., Escarmis, C., Menendez-Arias, L. & Holland, J. in Origin And Evolution of Viruses (eds Domingo, E., Webster, R. & Holland, J.) 141–161 (Academic Press, San Diego, 1999).
Book Google Scholar - Harrigan, P. R., Bloor, S. & Larder, B. A. Relative replicative fitness of zidovudine-resistant human immunodeficiency virus type 1 isolates in vitro. J. Virol. 72, 3773–3778 (1998).
Article CAS PubMed PubMed Central Google Scholar - Quinones-Mateu, M. E. & Arts, E. J. Virus fitness: concept, quantification, and application to HIV population dynamics. Curr. Top. Microbiol. Immunol. 299, 83–140 (2006).
CAS PubMed Google Scholar - Clarke, D. K. et al. The red queen reigns in the kingdom of RNA viruses. Proc. Natl Acad. Sci. USA 91, 4821–4824 (1994).
Article CAS PubMed PubMed Central Google Scholar - Novella, I. S. et al. Exponential increases of RNA virus fitness during large population transmissions. Proc. Natl Acad. Sci. USA 92, 5841–5844 (1995).
Article CAS PubMed PubMed Central Google Scholar - Chao, L. Fitness of RNA virus decreased by Muller's ratchet. Nature 348, 454–455 (1990).
Article CAS PubMed Google Scholar - Domingo, E. & Holland, J. J. RNA virus mutations and fitness for survival. Annu. Rev. Microbiol. 51, 151–178 (1997).
Article CAS PubMed Google Scholar - Yuste, E., Sanchez-Palomino, S., Casado, C., Domingo, E. & Lopez-Galindez, C. Drastic fitness loss in human immunodeficiency virus type 1 upon serial bottleneck events. J. Virol. 73, 2745–2751 (1999).
Article CAS PubMed PubMed Central Google Scholar - Mullins, J. I. & Jensen, M. A. Evolutionary dynamics of HIV-1 and the control of AIDS. Curr. Top. Microbiol. Immunol. 299, 171–192 (2006).
CAS PubMed Google Scholar - Wei, X. et al. Viral dynamics in human immunodeficiency virus type 1 infection. Nature 373, 117–122 (1995).
Article CAS PubMed Google Scholar - Betts, M. R. et al. Analysis of total human immunodeficiency virus (HIV)-specific CD4+ and CD8+ T-cell responses: relationship to viral load in untreated HIV infection. J. Virol. 75, 11983–11991 (2001).
Article CAS PubMed PubMed Central Google Scholar - Rosenberg, E. S. et al. Immune control of HIV-1 after early treatment of acute infection. Nature 407, 523–526 (2000).
Article CAS PubMed Google Scholar - Goulder, P. J. et al. Substantial differences in specificity of HIV-specific cytotoxic T cells in acute and chronic HIV infection. J. Exp. Med. 193, 181–194 (2001).
Article CAS PubMed PubMed Central Google Scholar - Goulder, P. J. & Watkins, D. I. HIV and SIV CTL escape: implications for vaccine design. Nature Rev. Immunol. 4, 630–640 (2004).
Article CAS Google Scholar - Cao, K. et al. Differentiation between African populations is evidenced by the diversity of alleles and haplotypes of HLA class I loci. Tissue Antigens 63, 293–325 (2004).
Article CAS PubMed Google Scholar - Moore, C. B. et al. Evidence of HIV-1 adaptation to HLA-restricted immune responses at a population level. Science 296, 1439–1443 (2002).
Article CAS PubMed Google Scholar - Goulder, P. J. et al. Evolution and transmission of stable CTL escape mutations in HIV infection. Nature 412, 334–338 (2001).
Article CAS PubMed Google Scholar - Leslie, A. J. et al. HIV evolution: CTL escape mutation and reversion after transmission. Nature Med. 10, 282–289 (2004).
Article CAS PubMed Google Scholar - Martinez-Picado, J. et al. Fitness cost of escape mutations in p24 Gag in association with control of human immunodeficiency virus type 1. J. Virol. 80, 3617–3623 (2006).
Article CAS PubMed PubMed Central Google Scholar - Troyer, R. M. et al. The fitness cost of CTL escape: not a terrible hardship on HIV-1? [online], (XVI International AIDS Conference, Toronto, Canada 13–18 August, 2006)
- Sheehy, A. M., Gaddis, N. C., Choi, J. D. & Malim, M. H. Isolation of a human gene that inhibits HIV-1 infection and is suppressed by the viral Vif protein. Nature 418, 646–650 (2002).
Article CAS PubMed Google Scholar - Stremlau, M. et al. The cytoplasmic body component TRIM5α restricts HIV-1 infection in Old World monkeys. Nature 427, 848–853 (2004).
Article CAS PubMed Google Scholar - Markowitz, M. et al. Infection with multidrug resistant, dual-tropic HIV-1 and rapid progression to AIDS: a case report. Lancet 365, 1031–1038 (2005).
Article PubMed Google Scholar - Van de, P. P. Viral and host determinants of HIV-1 pathogenesis. AIDS 20, 933–934 (2006).
Article Google Scholar - Muller, V. & De Boer, R. J. The integration hypothesis: an evolutionary pathway to benign SIV infection. PLoS Pathog. 2, e15 (2006).
Article PubMed PubMed Central CAS Google Scholar - Muller, V. et al. Stable virulence levels in the HIV epidemic of Switzerland over two decades. AIDS 20, 889–894 (2006).
Article PubMed Google Scholar - Kannangara, S., DeSimone, J. A. & Pomerantz, R. J. Attenuation of HIV-1 infection by other microbial agents. J. Infect. Dis. 192, 1003–1009 (2005).
Article PubMed Google Scholar - Arien, K. K. et al. Replicative fitness of historical and recent HIV-1 isolates suggests HIV-1 attenuation over time. AIDS 19, 1555–1564 (2005).
Article PubMed Google Scholar - Yerly, S. et al. Transmission of antiretroviral-drug-resistant HIV-1 variants. Lancet 354, 729–733 (1999).
Article CAS PubMed Google Scholar - Turner, D. & Wainberg, M. A. HIV transmission and primary drug resistance. AIDS Rev. 8, 17–23 (2006).
PubMed Google Scholar - Eyster, M. E. Test may predict which patients with HIV infection will develop AIDS. Am. Fam. Physician 39, 276 (1989).
CAS PubMed Google Scholar - McCune, J. M. The dynamics of CD4+ T-cell depletion in HIV disease. Nature 410, 974–979 (2001).
Article CAS PubMed Google Scholar - Marlink, R. et al. Reduced rate of disease development after HIV-2 infection as compared to HIV-1. Science 265, 1587–1590 (1994).
Article CAS PubMed Google Scholar - Matheron, S. et al. Factors associated with clinical progression in HIV-2 infected-patients: The French ANRS cohort. AIDS 17, 2593–2601 (2003).
Article PubMed Google Scholar - Gilbert, P. B. et al. Comparison of HIV-1 and HIV-2 infectivity from a prospective cohort study in Senegal. Stat. Med. 22, 573–593 (2003).
Article PubMed Google Scholar - Kanki, P. J. et al. Slower heterosexual spread of HIV-2 than HIV-1. Lancet 343, 943–946 (1994).
Article CAS PubMed Google Scholar - Essex, M. Human immunodeficiency viruses in the developing world. Adv. Virus Res. 53, 71–88 (1999).
Article CAS PubMed Google Scholar - Luo, C. C. et al. HIV-1 subtype C in China. Lancet 345, 1051–1052 (1995).
Article CAS PubMed Google Scholar - Piyasirisilp, S. et al. A recent outbreak of human immunodeficiency virus type 1 infection in southern China was initiated by two highly homogeneous, geographically separated strains, circulating recombinant form AE and a novel BC recombinant. J. Virol. 74, 11286–11295 (2000).
Article CAS PubMed PubMed Central Google Scholar - Soares, E. A. et al. HIV-1 subtype C dissemination in southern Brazil. AIDS 19, S81–S86 (2005).
Article PubMed Google Scholar - Vidal, N. et al. Distribution of HIV-1 variants in the Democratic Republic of Congo suggests increase of subtype C in Kinshasa between 1997 and 2002. J. Acquir. Immune. Defic. Syndr. 40, 456–462 (2005).
Article PubMed Google Scholar - Walker, P. R., Pybus, O. G., Rambaut, A. & Holmes, E. C. Comparative population dynamics of HIV-1 subtypes B and C: subtype-specific differences in patterns of epidemic growth. Infect. Genet. Evol. 5, 199–208 (2005).
Article CAS PubMed Google Scholar - Renjifo, B. et al. Differences in perinatal transmission among human immunodeficiency virus type 1 genotypes. J. Hum. Virol. 4, 16–25 (2001).
CAS PubMed Google Scholar - Renjifo, B. et al. Preferential in utero transmission of HIV-1 subtype C as compared to HIV-1 subtype A or D. AIDS 18, 1629–1636 (2004).
Article CAS PubMed Google Scholar - Yang, C. et al. Genetic diversity of HIV-1 in western Kenya: subtype-specific differences in mother-to-child transmission. AIDS 17, 1667–1674 (2003).
Article PubMed Google Scholar - Eshleman, S. H. et al. Comparison of mother-to-child transmission rates in Ugandan women with subtype A versus D HIV-1 who received single-dose nevirapine prophylaxis. HIV Network For Prevention Trials 012. J. Acquir. Immune. Defic. Syndr. 39, 593–597 (2005).
PubMed Google Scholar - Pope, M. et al. Human immunodeficiency virus type 1 strains of subtypes B and E replicate in cutaneous dendritic cell-T-cell mixtures without displaying subtype-specific tropism. J. Virol. 71, 8001–8007 (1997).
Article CAS PubMed PubMed Central Google Scholar - Dittmar, M. T. et al. Langerhans cell tropism of human immunodeficiency virus type 1 subtype A through F isolates derived from different transmission groups. J. Virol. 71, 8008–8013 (1997).
Article CAS PubMed PubMed Central Google Scholar - Tovanabutra, S. et al. The changing molecular epidemiology of HIV type 1 among northern Thai drug users, 1999 to 2002. AIDS Res. Hum. Retroviruses 20, 465–475 (2004).
Article CAS PubMed Google Scholar - Zaitseva, M. et al. Expression and function of CCR5 and CXCR4 on human Langerhans cells and macrophages: implications for HIV primary infection. Nature Med. 3, 1369–1375 (1997).
Article CAS PubMed Google Scholar - Arien, K. K. et al. The replicative fitness of primary human immunodeficiency virus type 1 (HIV-1) group M, HIV-1 group O, and HIV-2 isolates. J. Virol. 79, 8979–8990 (2005).
Article CAS PubMed PubMed Central Google Scholar - Johnston, E. R. et al. High frequency of syncytium-inducing and CXCR4-tropic viruses among human immunodeficiency virus type 1 subtype C-infected patients receiving antiretroviral treatment. J. Virol. 77, 7682–7688 (2003).
Article CAS PubMed PubMed Central Google Scholar - Gupta, S., Anderson, R. M. & May, R. M. Networks of sexual contacts: implications for the pattern of spread of HIV. AIDS 3, 807–817 (1989).
Article CAS PubMed Google Scholar - Anderson, R. M., Ng, T. W., Boily, M. C. & May, R. M. The influence of different sexual-contact patterns between age classes on the predicted demographic impact of AIDS in developing countries. Ann. N. Y. Acad. Sci. 569, 240–274 (1989).
Article CAS PubMed Google Scholar - Pilcher, C. D., Eron, J. J. Jr, Galvin, S., Gay, C. & Cohen, M. S. Acute HIV revisited: new opportunities for treatment and prevention. J. Clin. Invest. 113, 937–945 (2004).
Article CAS PubMed PubMed Central Google Scholar - Jacquez, J. A., Koopman, J. S., Simon, C. P. & Longini, I. M. Jr. Role of the primary infection in epidemics of HIV infection in gay cohorts. J. Acquir. Immune. Defic. Syndr. 7, 1169–1184 (1994).
CAS PubMed Google Scholar - Koopman, J. S. et al. The role of early HIV infection in the spread of HIV through populations. J. Acquir. Immune. Defic. Syndr. Hum. Retrovirol. 14, 249–258 (1997).
Article CAS PubMed Google Scholar - Ndung'u, T. et al. Infectious simian/human immunodeficiency virus with human immunodeficiency virus type 1 subtype C from an African isolate: rhesus macaque model. J. Virol. 75, 11417–11425 (2001).
Article CAS PubMed PubMed Central Google Scholar - Gray, C. M. et al. Viral dynamics and CD4+ T cell counts in subtype C human immunodeficiency virus type 1-infected individuals from southern Africa. AIDS Res. Hum. Retroviruses 21, 285–291 (2005).
Article CAS PubMed Google Scholar - Neilson, J. R. et al. Subtypes of human immunodeficiency virus type 1 and disease stage among women in Nairobi, Kenya. J. Virol. 73, 4393–4403 (1999).
Article CAS PubMed PubMed Central Google Scholar - Kaleebu, P. et al. Effect of human immunodeficiency virus (HIV) type 1 envelope subtypes A and D on disease progression in a large cohort of HIV-1-positive persons in Uganda. J. Infect. Dis. 185, 1244–1250 (2002).
Article PubMed Google Scholar - Vasan, A. et al. Different rates of disease progression of HIV type 1 infection in Tanzania based on infecting subtype. Clin. Infect. Dis. 42, 843–852 (2006).
Article PubMed Google Scholar - Kaleebu, P. et al. Relationship between HIV-1 Env subtypes A and D and disease progression in a rural Ugandan cohort. AIDS 15, 293–299 (2001).
Article CAS PubMed Google Scholar - Choge, I. et al. Genotypic and phenotypic characterization of viral isolates from HIV-1 subtype C-infected children with slow and rapid disease progression. AIDS Res. Hum. Retroviruses 22, 458–465 (2006).
Article CAS PubMed Google Scholar - Senkaali, D. et al. The relationship between HIV type 1 disease progression and V3 serotype in a rural Ugandan cohort. AIDS Res. Hum. Retroviruses 20, 932–937 (2004).
Article PubMed Google Scholar - Arts, E. J. et al. Infection with subtype C HIV-1 of lower replicative fitness as compared to subtypes A and D leads to slower disease progression in Zimbabwean and Ugandan women. [online], (XVI International AIDS Conference, Toronto, Canada 13–18 August, 2006).
- Pierson, T., McArthur, J. & Siliciano, R. F. Reservoirs for HIV-1: mechanisms for viral persistence in the presence of antiviral immune responses and antiretroviral therapy. Annu. Rev. Immunol. 18, 665–708 (2000).
Article CAS PubMed Google Scholar - Finzi, D. et al. Identification of a reservoir for HIV-1 in patients on highly active antiretroviral therapy. Science 278, 1295–1300 (1997).
Article CAS PubMed Google Scholar - Li, D. Q., Zheng, X. W. & Zhang, G. Y. Study on the distribution HIV-1 C subtype in Ruili and other counties, Yunnan, China (Translation). Zhonghua Liu Xing. Bing. Xue. Za Zhi. 17, 337–339 (1996).
CAS PubMed Google Scholar - Li, X. J. et al. Molecular epidemiology of the heterosexual HIV-1 transmission in Kunming, Yunnan Province of China suggests origin from the local IDU epidemic. AIDS Res. Hum. Retroviruses 21, 977–980 (2005).
Article CAS PubMed Google Scholar - Van Harmelen, J. H. et al. A predominantly HIV type 1 subtype C-restricted epidemic in South African urban populations. AIDS Res. Hum. Retroviruses 15, 395–398 (1999).
Article CAS PubMed Google Scholar - Rainwater, S. et al. No evidence for rapid subtype c spread within an epidemic in which multiple subtypes and intersubtype recombinants circulate. AIDS Res. Hum. Retroviruses 21, 1060–1065 (2005).
Article PubMed Google Scholar
Acknowledgements
We thank Miguel Quinones-Mateu, Luc Kestens, Robert Colebunders and Guido van der Groen for their helpful suggestions in the development of these attenuation hypotheses. We also thank Aslam Syed and Lora Angelova in the Arts laboratory for their contributions to the supplementary data.
Author information
Author notes
- Kevin K. Ariën
Present address: the Department of Clinical Chemistry, Microbiology and Immunology, Faculty of Medicine and Health Sciences, Ghent University, De Pintelaan 185, Ghent, B-9000, Belgium
Authors and Affiliations
- the Department of Microbiology, HIV and Retrovirology Research Unit, Institute of Tropical Medicine, Nationalestraat 155, Antwerp, B2000, Belgium
Kevin K. Ariën & Guido Vanham - the Division of Infectious Diseases, Department of Medicine, Case Western Reserve University, 2109, Adelbert Rd, Cleveland, 44195, Ohio, USA
Eric J. Arts
Authors
- Kevin K. Ariën
You can also search for this author inPubMed Google Scholar - Guido Vanham
You can also search for this author inPubMed Google Scholar - Eric J. Arts
You can also search for this author inPubMed Google Scholar
Corresponding author
Correspondence toEric J. Arts.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Supplementary information
Related links
Related links
DATABASES
Entrez Genome Project
FURTHER INFORMATION
Rights and permissions
About this article
Cite this article
Ariën, K., Vanham, G. & Arts, E. Is HIV-1 evolving to a less virulent form in humans?.Nat Rev Microbiol 5, 141–151 (2007). https://doi.org/10.1038/nrmicro1594
- Published: 04 January 2007
- Issue Date: 01 February 2007
- DOI: https://doi.org/10.1038/nrmicro1594